Submitted:
23 February 2025
Posted:
24 February 2025
You are already at the latest version
Abstract
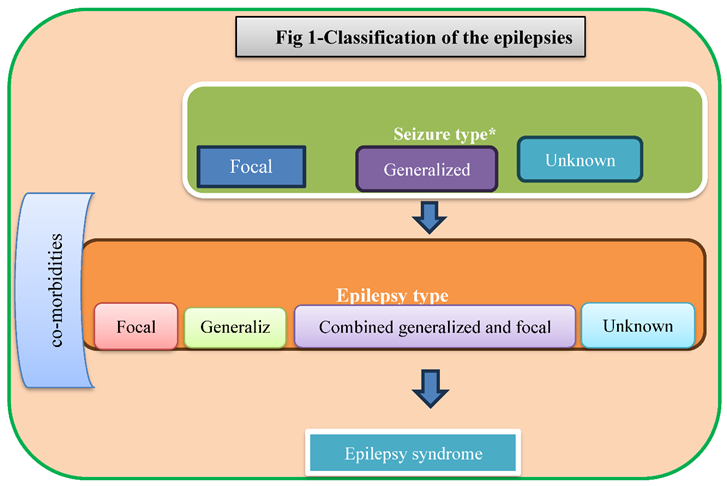
Pregnancy is the period of time when a fetus develops inside a woman's uterus. When counting from the last menstrual cycle through delivery, a pregnancy typically lasts around 40 weeks, or slightly over 9 months. Pregnancy is divided into three trimesters, as described by healthcare professionals. First trimester: from conception to 12 weeks; second trimester: from 13 to 28 weeks; third trimester: from 29 to 40 weeks. Seizures are a defining feature of the illness, however not all seizures are caused by epilepsy, such as febrile seizures or seizures brought on by drugs. The multilevel categorization of epilepsies was developed to facilitate categorizing epilepsy in varied clinical contexts. There are three types of seizures: those with undetermined onset, generalized onset, and focal onset. The second level is epilepsy type, which introduces the new categories of generalized epilepsy, focal epilepsies, and unknown. A variety of seizure forms, including absence, myoclonic, atonic, tonic, and tonic-clonic seizures, can occur in generalized epilepsies. An epilepsy syndrome diagnosis comes in third place. An epilepsy syndrome is a collection of symptoms that includes seizure types, EEG patterns, and imaging characteristics that frequently co-occur. This review underwent a narrative evaluation, for which papers from the Cochrane library, PubMed, Google Scholar, and Web of Science were gathered. Epilepsy is treated with antiepileptic medications (AEDs). There is evidence that suggests some antiepileptic drugs (AEDs) increase the chance of congenital malformation and induce teratology. The risk of malformation is increased by medications including carbamazepine, phenobarbital, phenytoin, topiramate, and valproate, but not by lamotrigine, gabapentin, levetiracetam, oxcarbazepine, primidone, or zonisamide. Lacosamide, Eslicarbazepine, Clonazepam, Clobazam, and Rivaracetam did not either.
Keywords:
Introduction
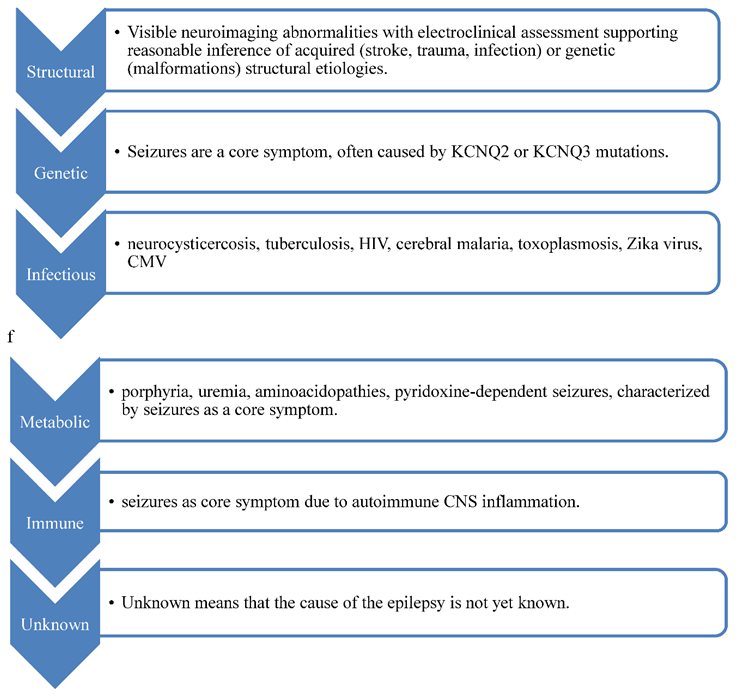
- Etiology(2)
- Antiepileptic drugs (AEDs):
Method
Result
Literature Finding
Conclusion
References
- Manford M. Recent advances in epilepsy. J Neurol. 2017 Aug;264(8):1811–24.
- Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia [Internet]. 2017 Apr [cited 2023 May 17];58(4):512–21. Available from: . [CrossRef]
- Perucca E. An Introduction to Antiepileptic Drugs: INTRODUCTION TO ANTIEPILEPTIC DRUGS. Epilepsia [Internet]. 2005 Jun 6 [cited 2023 May 17];46:31–7. Available from: . [CrossRef]
- Weston J, Bromley R, Jackson CF, Adab N, Clayton-Smith J, Greenhalgh J, et al. Monotherapy treatment of epilepsy in pregnancy: congenital malformation outcomes in the child. Cochrane Epilepsy Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2016 Nov 7 [cited 2023 May 14];2017(4). Available from: . [CrossRef]
- Veroniki AA, Cogo E, Rios P, Straus SE, Finkelstein Y, Kealey R, et al. Comparative safety of anti-epileptic drugs during pregnancy: a systematic review and network meta-analysis of congenital malformations and prenatal outcomes. BMC Med. 2017 May 5;15(1):95. [CrossRef]
- Vajda FJE, O’Brien TJ, Graham JE, Hitchcock AA, Lander CM, Eadie MJ. Antiepileptic drug polytherapy in pregnant women with epilepsy. Acta Neurol Scand. 2018 Aug;138(2):115–21. [CrossRef]
- Meador KJ, Pennell PB, May RC, Gerard E, Kalayjian L, Velez-Ruiz N, et al. Changes in antiepileptic drug-prescribing patterns in pregnant women with epilepsy. Epilepsy Behav. 2018 Jul;84:10–4. [CrossRef]
- Bromley R, Weston J, Adab N, Greenhalgh J, Sanniti A, McKay AJ, et al. Treatment for epilepsy in pregnancy: neurodevelopmental outcomes in the child. Cochrane Epilepsy Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2014 Oct 30 [cited 2023 May 14];2020(6). Available from: . [CrossRef]
- Avachat C, Birnbaum AK. Women of childbearing age: What antiseizure medications are they taking? Brit J Clinical Pharma [Internet]. 2023 Jan [cited 2023 May 14];89(1):46–8. Available from: . [CrossRef]
- Apostolakopoulou L, Bosque Varela P, Rossini F, O’Sullivan C, Löscher W, Kuchukhidze G, et al. Intravenous topiramate for seizure emergencies – First in human case report. Epilepsy & Behavior [Internet]. 2023 May [cited 2023 May 14];142:109158. Available from: . [CrossRef]
- Yang MT, Chou IC, Wang HS. Role of vitamins in epilepsy. Epilepsy & Behavior [Internet]. 2023 Feb [cited 2023 May 14];139:109062. Available from: . [CrossRef]
- Wójcik K, Franciszek Kołek M, Dec-Ćwiek M, Słowik A, Bosak M. Trends in antiseizure medications utilization among women of childbearing age with epilepsy in Poland between 2015 and 2019. Epilepsy & Behavior [Internet]. 2023 Feb [cited 2023 May 14];139:109091. Available from: . [CrossRef]
- Hoeltzenbein M, Slimi S, Fietz AK, Stegherr R, Onken M, Beyersmann J, et al. Increasing use of newer antiseizure medication during pregnancy: An observational study with special focus on lacosamide. Seizure [Internet]. 2023 Apr [cited 2023 May 14];107:107–13. Available from: . [CrossRef]
- Bansal R, Suri V, Chopra S, Aggarwal N, Sikka P, Saha SC, et al. Change in antiepileptic drug prescription patterns for pregnant women with epilepsy over the years: Impact on pregnancy and fetal outcomes. Indian J Pharmacol. 2019;51(2):93–7. [CrossRef]

| Drugs | Blockade of voltage dependent sodium channels | Increase in brain or synaptic GABA levels |
Selective potentiation of GABAA-mediated responses |
Direct facilitation of chloride ion influx |
Blockade of calcium channels | Other actions |
|---|---|---|---|---|---|---|
| Felbamate | ✓✓ | ✓ | ✓ | × | ✓ (L-type) | ✓ |
| Gabapentin | ? | ? | × | × | ✓✓ (N-, P/Q-type) | ? |
| Lamotrigine | ✓✓ | ✓ | × | ✓✓ | ✓✓ (N-, P/Q-, R-, T-type) | ✓ |
| Levetiracetam | × | ? | ✓ | × | ✓ (N-type) | ✓✓ |
| Oxcarbazepine | ✓✓ | ? | × | × | ✓ (N- and P-type) | ✓ |
| Pregabalin | × | × | × | × | ✓✓ (N-, P/Q-type) | × |
| Tiagabine | × | ✓✓ | × | × | × | × |
| Vigabatrin | × | ✓✓ | × | × | × | × |
| Zonisamide | ✓✓ | ? | × | × | ✓✓ (N-,P-,T-type) | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



