
Submitted:
13 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Wheat, a component of the staple diet globally, is a common food allergen in children. The symptoms of wheat allergy (WA) range from skin rash to shortness of breath, significantly impairing quality of life. Following initial clinical suspicion, individuals may undergo wheat allergen-specific skin prick test (SPT), blood test for serum immunoglobulin E (sIgE) levels or oral food challenge. Conventional management of WA lies in wheat avoidance, yet accidental consumption may be inevitable owing to the ubiquity of wheat in various food products. This article aims to provide an overview of the immunologic pathway of WA, followed by its novel diagnostic methods, namely alcohol-soluble SPT extracts, component-resolved diagnosis and basophil activation test (BAT). The mechanisms underlying wheat allergen-specific oral immunotherapy (OIT) as well as a summary of the efficacy, tolerability and safety of related clinical trials will then be discussed.
Keywords:
Component-resolved diagnosis
; desensitization
; immunology
; oral immunotherapy
; wheat allergy
1. Introduction
Wheat (Triticum aestivum) plays an important role in the global human diet due to its nutritional value and adaptability to diverse climatic conditions. However, the prevalence of wheat allergy (WA) poses significant concern. Wheat is identified as one of the top five triggers of allergic reactions in children. In Germany and Japan, it ranks as the third most common food allergen, after milk and eggs [1]; according to Yu et al, WA is in fact the top cause of anaphylaxis in Japan and Korea [2]. A European meta-analysis of food allergy prevalence revealed that the overall lifetime prevalence of self-reported WA was around 1.6% (95% confidence interval [CI] 0.9-2.3) with the highest being among preschool children aged 2-5 years, while the point prevalence of food challenge-verified WA was 0.1% (95% CI 0.01-0.2) [3]. The lifetime prevalence for self-reported WA was lower than those of cow’s milk (5.7%, 4.4-6.9) and egg (2.4%, 1.8-3.0) and comparable to the respective figures for peanut allergy (1.5%, 1.0-2.1) and fish (1.4%, 0.8-2.0).
Wheat allergy is an immune-mediated adverse reaction triggered by the consumption of wheat or wheat-based products [4]. It includes three main types: immunoglobulin E (IgE)-mediated, non-IgE-mediated, and mixed-IgE-mediated forms [2]. The latter two types are less common with mechanisms yet to be delineated, and thus are not detailed here. IgE-mediated WA involves two stages, namely sensitization and elicitation. Sensitization occurs upon initial exposure to wheat, leading to the production of wheat protein-specific IgE antibodies. During the elicitation phase, subsequent exposure triggers the interaction between cell-bound IgE and the same wheat proteins, resulting in the release of allergic mediators from mast cells and basophils. Gut microbiota appears to play a role in modulating allergic responses [2,4-7], as reflected by the increased prevalence of certain microorganisms in the gut of wheat-allergic children [8]. These processes lead to a range of clinical manifestations within minutes to hours after wheat consumption, including erythema, pruritus, gastrointestinal reactions, oropharyngeal symptoms, urticaria, angioedema, atopic dermatitis, rhinitis, asthma; in severe cases, WA may escalate to life-threatening anaphylaxis [5].
Current treatment for WA primarily relies on strict avoidance of wheat and prompt management of adverse reactions resulting from accidental exposure [9]. However, challenges arise since wheat is widely used to manufacture various food products, increasing the likelihood of inadvertent exposure. Therefore, alternative desensitization treatments are needed. Immunotherapy, comprising oral immunotherapy (OIT), sublingual immunotherapy (SLIT), and epicutaneous immunotherapy (EPIT), holds promise in this regard [9]; in particular, OIT has been extensively studied for WA. Oral immunotherapy aims at inducing oral tolerance to allergenic foods by modulating both innate and adaptive immune mechanisms [2,7,10], reflected by reduced secretion of inflammatory mediators from mast cells and basophils, increased levels of wheat allergen-specific immunoglobulin G 4 (IgG4) and wheat allergen-specific IgE levels that initially elevate then decrease [10].
To date, wheat allergen-specific OIT is yet to be incorporated into clinical practice due to its early stage in research. Nonetheless, this article will review the immunologic pathways of WA and mechanism of wheat allergen-specific OIT correspondingly, on a molecular level. Novel diagnostic methods and treatment options will also be introduced, with a specific focus on oral immunotherapy.
2. Immune Mechanism and Interaction with Microbiota
2.1. Sensitization
The process of IgE-mediated WA involves two stages — sensitization upon initial exposure to wheat allergens and elicitation when encountering re-exposure. Sensitization occurs when wheat allergens enter the body following digestion and absorption at the gastrointestinal tract. Epithelial-derived inflammatory cytokines, such as interleukin (IL)-25, IL-33, and thymic stromal lymphopoietin (TSLP), act on dendritic cells (DCs) and other cells to skew the immune response [7,11,12]. The tumor necrosis factor receptor superfamily member 4 (OX40) ligand (OX40L), upregulated on DCs, induces differentiation of naive T cells into T helper 2 (Th2) cells instead of regulatory T (Treg) cells, which would elicit tolerogenic responses [13]. This Th2-biased immune dysregulation results in the production of IL-4, IL-5, and IL-13, promoting class switching of B cells to produce more wheat allergen-specific IgE. These IgE antibodies bind to mast cells and basophils via their high-affinity IgE receptors (FcεRI) [14-17]. Upon re-exposure to wheat allergens, allergen-antibody binding triggers IgE crosslinking and hence the activation of tissue-residing mast cells and blood-circulating basophils, swiftly releasing inflammatory and vasoactive mediators such as histamine, platelet-activating factor, and leukotrienes to induce local or systemic allergic reactions [5,17-20] (Figure 1).
2.2. Desensitization by Immunotherapy
Immunotherapy desensitizes the immune systems of individuals via modulating the humoral immune response and activities of T cells and DCs [2,7,9]. In immunotherapy, IgE levels rise transiently then fall. The allergen-specific IgG levels, especially serum IgG4 (sIgG4), however steadily increase [21-23], likely due to steady release from the upstream IL-10 and allergen-specific regulatory B (Breg) cell pathways. The IgG isotypes also dampen IgE-mediated responses by binding to FcγRIIb and suppressing IgE-mediated activation of basophils and mast cells [2,24-26]. Allergen-specific immunoglobulin A (IgA) supports antigen exclusion and enhances the specificity of desensitization [7].
Repeated allergen exposures during OIT also induce apoptosis and anergy of allergen-specific Th2 cells alongside further activation of allergen-induced Treg cell functions. As abovenamed, Treg cells are tolerogenic, hindering mast cell activation directly via OX40-OX40L interaction and inhibiting DCs required for effector T cell activation [2,27]; clinically, they protect individuals from anaphylaxis. The synergistic effects of immunoglobulins and T cells facilitate allergen desensitization in immunotherapy. Further studies, however, are required to observe for any wheat allergen-specific mechanisms of desensitization in wheat immunotherapy.
2.3. Microbiota
The role of microbiota in food allergy has been increasingly studied in recent years. Environmental factors such as delivery mode, antibiotic use, and diet may trigger microbial dysbiosis, predisposing individuals to allergic sensitization [7,28-30]. The gut microbiota plays a crucial role in modulating allergic responses to food antigens by activating DCs on the gut mucosal surface. These activated DCs produce IL-10 and IL-22 to stimulate maturation of naive T cells into Treg cells and enhance the production of anti-microbial and food allergen-specific IgA, establishing food tolerance. Conversely, an imbalance of gut microbiota in the intestinal epithelium may lead to elevated levels of IL-4, IL-33, and allergen-specific IgE, driving Th2 cell-biased responses and stimulating basophil activation in the intestine [6,30-32].
Studies have shown alterations in gut microbiota in children with WA compared to those without [33]. A study by Kanchongkittiphon et al revealed statistically significant enrichment of Anaerostripes, Erysipelatoclostridium, Prevotella 2, Ruminiclostridium 5, and Clostridium innnocuum species in children with physician-diagnosed WA [8]. The specific bacterial groups or species involved in the induction of Treg cells in the intestinal mucosa remain unknown. It appears that genera such as Lactobacillus, Bifidobacterium, and Clostridium, along with microbial fermentation products like butyrate stimulate Treg cells and alleviate food allergy symptoms [30,34,35]. Further large-scale studies may elucidate the role of the microbiome in WA-associated immune regulation.
3. Clinical Features and Related Disorders
Allergic responses to wheat can manifest in a variety of clinical symptoms, ranging from localized to severe systemic reactions occurring within minutes to hours after wheat exposure [2,5,36,37]. Typical immediate symptoms include gastrointestinal discomfort (nausea, abdominal pain, vomiting, and/or diarrhea), respiratory difficulties (rhinitis, wheezing, and/or asthma) and skin manifestations (eczema, redness, itching, urticaria, and/or angioedema). In severe cases, systemic reactions such as hypotension, hypothermia or anaphylaxis may also occur; the latter affects multiple organ systems and can rapidly become life-threatening.
Wheat-dependent exercise-induced anaphylaxis (WDEIA), a distinct form of WA presenting as asthma, dyspnea, urticaria, angioedema, syncope, and more rarely shock, is typically diagnosed in adults but occasionally also in older children [38-40]. WDEIA may occur 10 to 60 minutes after physical activity when preceded by wheat ingestion 10 minutes to four hours ago, or upon wheat consumption immediately after exercise. Matsuo et al. found that exercise might accentuate allergic reactions in WDEIA by increasing gliadin absorption from the gastrointestinal tract [41], while another Japanese study suggested a role for filaggrin in WDEIA [42]. The severity of clinical manifestations may be dependent on the amount of wheat ingested and exercise intensity. Alcohol and non-steroidal anti-inflammatory drugs such as aspirin have been identified as significant risk factors for WDEIA and can trigger episodes even without exercise in a subset of patients [43,44].
4. Diagnosis
4.1. Conventional Diagnostic Strategies
The diagnostic algorithm of WA follows the sequence of history taking, general assessment, then further investigations (Figure 2). The two screening tests are skin prick test (SPT) and blood test for measuring serum IgE (sIgE) levels, while oral food challenge (OFC) is performed for confirmation. While the double-blind, placebo-controlled food challenge test (DBPCFC) is considered the gold standard to achieve a definitive diagnosis of WA, an objectively measured open-label OFC may suffice in certain clinical scenarios [45-47]. In OFCs, individuals receive incremental doses of whole wheat extracts in a stepwise manner, from one to 50 milligrams (mg) of wheat-specific protein to larger hourly doses, with a cumulative dose of up to 0.5-1 gram (g) of wheat protein [39]. Wheat allergy is diagnosed when (1) the OFC result is positive and (2) symptoms manifest within two hours after ingestion. Although clinical trials have demonstrated the tolerability of wheat allergen-specific OFC, on-site standby of trained healthcare providers may provide subjects with more reassurance, in the event of rare near-fatal adverse events.
The most commonly adopted diagnostic methods of WA are SPT and sIgE measurement. Although the latter enjoys higher sensitivity, these tests are both of low specificity [48]. A postulation for such drawback may be that commercially prepared wheat extracts fail to contain the salt-insoluble major wheat allergens, i.e. gliadins and glutenins [48-50]. This concern has been addressed by novel wheat extract formulations with gliadin and glutenin-solubilizing properties, which yielded better accuracy for diagnosing WA in children than their preceding commercial wheat extracts [51-53]. Another postulation is that extensive allergen cross-reactivity between wheat flour and grass pollen may lower the specificity of SPT and sIgE to wheat. More than 60% of subjects with grass pollen allergy showed false positive results in sIgE to wheat, although they were all clinically asymptomatic [54,55]. Another observation unique to WA is that the wheat allergen-specific IgE levels may be falsely elevated in wheat-tolerant individuals — in children who previously had WA but developed tolerance, about 27% to 40% still display elevated levels of sIgE to whole wheat extract (>50 kU/L) in one to two years [56,57]. These altogether account for the low specificity of conventional SPT and sIgE measurements.
4.2. Wheat Allergens and Component-Resolved Diagnosis
Wheat belongs to the grass family Poaceae and contains numerous allergenic proteins, which can be classified into two main fractions based on solubility in salt [4,37,58]. The salt-soluble fraction, constituting 15-20% of total proteins, includes albumins and globulins containing proteins such as α-Amylase/Trypsin inhibitors (ATIs) and lipid transfer proteins (LTPs). In contrast, the salt-insoluble fraction, comprising approximately 80% of wheat protein content, consists of gliadins and glutenins. Gliadins can be categorized into α/β, γ, and ω-gliadins based on their electrophoretic mobility under acidic conditions. Additionally, ω-gliadins can be further subdivided into ω1, ω2, and ω5 components. Glutenins can be separated via electrophoresis into high molecular weight (HMW) and low molecular weight (LMW) glutenin subunits.
In recent years, component-resolved diagnosis (CRD) has been utilized to identify specific components that can predict clinical reactions in cases of IgE-mediated WA and WDEIA. Commercial tests are now available to measure IgE sensitization to Tri a 19 (ω-5 gliadin) and Tri a 14 (non-specific LTP). Wheat ω-5 gliadin (Tri a 19) is well understood as the major allergen in WDEIA-affected individuals [38,59-61]. Studies have also revealed that ω-5 gliadin-specific sIgE is a strong predictor of immediate WA in children, with elevated levels correlating with positive results in OFC; ω-5 gliadin-specific IgE was detected in more than 80% of children with WA [46,49,62]. Meanwhile, wheat flour non-specific LTP is an important allergen for IgE-mediated WA, WDEIA, and Baker’s asthma; this protein exhibits resistance to heat and enzymatic degradation, retaining their allergenic potential even after food processing and digestion. Non-specific LTP also does not cross-react with grass pollen; thus, measurement of non-specific LTP may help differentiate wheat sensitization from pollen allergies, which is crucial in patients with high levels of grass pollen-specific IgE [4,36,39]. Furthermore, positive sIgE responses to glutenins, α-, β-, and γ-gliadins, as well as α-Amylase/Trypsin inhibitors have been found in wheat allergic children, yet none has reached a high specificity and sensitivity in WA diagnosis [48,63,64]. So far, CRD is mainly used in scientific research, and further studies are required to better understand these allergens.
4.3. Cell-Based Diagnosis
A new in-vitro test to complement WA diagnosis is the basophil activation test (BAT) by fluorescence-based flow cytometry [65-68]. In BAT, basophils are activated with whole blood and stimulated with an allergen-containing solution, leading to upregulated expression of cell surface proteins, namely CD63 and CD203c upon basophil degranulation, the latter also expresses in resting basophils [65,69]. Basophil activation test is established as a sensitive biomarker which corresponds to the clinical severity of anaphylactic reactions. Measurement of basophil CD203c expression induced by various preparations of wheat proteins, particularly ω-5 gliadin, is useful in predicting causative allergens in patients with WA and WDEIA [69,70]. Particular caution is required for subjects to completely avoid wheat intake before BAT as otherwise subjects’ basophils can be substantially activated at baseline. This problem can influence the accuracy of BAT results that assess the fold changes in CD63 or CD203c expression on basophils from baseline to after in-vitro wheat exposure. Meanwhile, the mast cell activation test (MAT) is similar to BAT, but MAT uses plasma or serum to sensitize mast cells instead of whole blood [45,68]. The application of MAT in clinical research is sparse [71], but may be a novel field of study in the coming years.
5. Management
5.1. Natural History of Wheat Allergy
Despite the high prevalence of WA, a considerable proportion of wheat-allergic children develop tolerance later in childhood, reflecting WA has a better prognosis than other allergies (e.g. peanuts, shellfish or fish) which often persist into adulthood. Several studies have shown that the median age of tolerance to wheat allergens is approximately six years old [56,57]. Resolution rates were found to be 20-29% by four years, 52-56% by eight years, 65-66% by 12 years, and 76% by 18 years. The progress of tolerance can be assessed by measuring wheat allergen-specific sIgE titers repeatedly while on elimination diet. As the wheat allergen-specific sIgE concentration rises, tolerance development becomes less likely, whereas declining sIgE titers suggest a higher likelihood of tolerance [36]. Studies have shown that for children with peak wheat sIgE levels below 20 kU/L, the median age of tolerance development was 2.6 years; for those with peak sIgE levels between 20 and 49 kU/L, it was 4.5 years; and for those with peak sIgE levels ≥ 50 kU/L, it was 12.1 years old [56]. The abovementioned suggests that peak wheat sIgE level is a useful predictor of tolerance development.
5.2. Therapeutic Strategies
The current management approach for IgE-mediated WA primarily involves strict avoidance of wheat-containing foods. Patients need to be educated to accurately identify wheat allergens in food labels and written instructions should be provided to effectively eliminate wheat from their diet [4,9]. Individuals with WDEIA individuals should especially refrain from exercising for up to six hours after consuming wheat or wheat-containing products; sometimes, complete wheat avoidance may even be recommended [5].
However, adhering to a wheat-free diet poses challenges due to the ubiquitous presence of wheat in various food items, including cakes, noodles, pasta, bread and condiments like soy sauce. Severe accidental exposure to wheat allergens may occur, necessitating the use of epinephrine autoinjectors to manage allergic reactions and subsequent emergency department admission for close monitoring [4]. Antihistamines, glucocorticoids and β-agonists are considered adjunctive treatments for anaphylaxis which may be used alone or in combination depending on the severity of the reaction [9].
5.3. Immunotherapy
Immunotherapy is a promising method for treating food allergies, with three main routes of administration — oral immunotherapy (OIT), sublingual immunotherapy (SLIT), and epicutaneous immunotherapy (EPIT) [9,72], among which OIT is the most studied. Oral immunotherapy works by inducing oral tolerance to allergenic foods through modification of both innate and adaptive immune response and adopts the abovementioned desensitization mechanism. While Tomsitz et al reported that SLIT increased reaction thresholds in three WDEIA-affected patients [73], there has not been any reported studies on EPIT for WA. However, the feasibility of SLIT in inducing unresponsiveness to wheat can be limited by the daily dosing of wheat that subjects can receive. Oral administration of OIT is the natural way through which subjects are exposed to wheat in their diet, and hence the plethora of research data that evaluated the potential usefulness of OIT in treating WA. As discussed above, several probiotics were a feasible treatment option for food allergy via the stimulation of Treg cells [30,34,35]. An Australian multi-center clinical trial reported safety benefit of a probiotic adjuvant during OIT for peanut allergy, while it did not improve the occurrence of sustained unresponsiveness [74]. There has not been any clinical trial that investigated the therapeutic benefits from a combination of probiotics and wheat OIT.
5.3.1. OIT Protocol
Standard OIT protocols typically comprise the rush, long-term build-up and maintenance phases (Figure 3) [10]. During the rush phase, patients first consume a very small dose of the test food (equivalent to the eliciting dose from DBPCFC), followed by a gradual increase in the dosage with six to eight doses per day. This phase is usually conducted in a hospital due to the high risk of systemic reactions. Once completed, patients are advised on a safe starting dose for self-administration at home. The subsequent build-up phase involves incremental increase in immunotherapy dosage every one to two weeks, typically by 20-30 percent increment per visit, until the maintenance dose (usually one serving dose) is reached. Patients maintain this dose for at least one to two years, followed by evaluation for desensitization and tolerance [also known as sustained unresponsiveness (SU)]. Desensitization indicates subjects’ ability to tolerate the maintenance dose when regularly consuming the food, whereas SU reflects their ability to tolerate doses even after discontinuing regular dosing. Throughout the treatment process, oral food challenge tests are performed to assess desensitization. Subjects with established SU should discontinue the allergenic food doses for at least 2 weeks before undergoing another oral food challenge [10]. The occurrence of SU is the closest surrogate for immunological tolerance as subjects are only intermittently exposed to the previously allergic food item. Nonetheless, long-term follow up of subjects for at least 1-2 years is required to ascertain if they have achieved immunological tolerance.
5.3.2. Clinical Trials
Table 1 summarizes the published clinical trials for wheat OIT protocols demonstrating wide variability, with efficacy being defined differently between trials [21-23,50,75-83]. For example, the types of wheat products utilized for the immunotherapy varied among studies — some used pasta, others used udon and bread, to name a few. Additionally, the target maintenance doses in different OIT trials ranged from 53 mg to 13 g of wheat protein (WP). Most studies used a maintenance dose of 5-6 g of WP [22,76,77,82], which is approximately equivalent to two to three slices of bread. The varying dosages may have been affected by the degree of wheat sensitization and reports on subjects’ tolerance level. For instance, in a wheat DBPCFC trial by Rodrigeuz del Rio et al. with higher threshold doses (ranging from 0.8 g to 12.5 g of WP), subjects were reported to be tolerant even to high maintenance doses of wheat (13 g of WP) without experiencing systemic reactions [75]; this may be attributed to a lower degree of wheat sensitization among this group of patients. Furthermore, maintenance durations varied widely, ranging from two months to three years. Some trials defined their primary endpoint as desensitization to a maintenance dose of OIT, with effectiveness ranging from 30% to 100%. Others defined their primary endpoint as SU to an oral wheat challenge after abstaining from wheat consumption for at least two weeks, with efficiency ranging from 13% to 100%. These altogether accounted for the varying degrees of measured efficacy and effectiveness, posing challenges for head-to-head comparison across trials.
Analysis from independent studies suggests that therapeutic outcomes are more dependent on the target dose of wheat protein and the duration of maintenance rather than the type of wheat products used. OIT trials employing higher maintenance doses and longer durations have demonstrated higher rates of desensitization. In a multicenter randomized controlled trial comparing lower (1445 mg) to higher dose (2748 mg) OIT, 30.4% versus 57.1% of subjects were able to tolerate a challenge of 7443 mg of WP respectively [78]. In another study which children were randomly
Assigned to the low-dose (650 mg) versus high-dose (2.6 g) OIT groups, 17% and 50% of subjects achieved SU after one year respectively [79]. In terms of OIT safety, the incidence of total adverse reactions per total ingestion time was significantly lower in the low-dose OIT compared to the high-dose OIT (4.76% vs 8.82%), suggesting that the low-dose protocol may be safer despite lower effectiveness. Furthermore, the duration of treatment may also impact OIT effectiveness. Nagakura et al reported that during OIT treatment, the proportion of patients achieving short-term unresponsiveness increased by 7%, 28%, and 41% after one, two and three years respectively [80]. Moreover, the frequency of adverse reactions per OIT dosing significantly decreased annually, indicating that the longer OIT protocol may be more effective and safer. Overall, exploring the maintenance dose and the duration of OIT will crucially impact the optimization of wheat OIT protocol.
Apart from influencing individuals’ clinical response to allergens, the efficacy of wheat OIT is also reflected by changes in the SPT and sIgE test results. Several studies, though not all, have reported initial increase and subsequent decrease in sIgE levels to wheat or ω-5 gliadin over the course of OIT [21,22]. Some studies reported reduction in sIgE levels to wheat or ω-5 gliadin upon completion of the OIT regimen [23,76,79-83]. However, in many cases, individuals still exhibited elevated sIgE levels even when upon desensitization or sustained unresponsiveness. Alongside changes in sIgE, decrease in SPT wheal sizes were reported in some wheat OIT trials [21,22,77], although this was not observed in several other studies [74,77,82]. Levels of sIgG4 to wheat and ω-5 gliadin generally increased with wheat OIT [23,75,78], but such finding was not consistent in other studies [79,83,84]. In summary, OIT may bring about changes in SPT, sIgE and sIgG4 levels to wheat or ω-5 gliadin in some cases which can estimate treatment efficacy, although the correlation of these changes with desensitization or SU remains unclear. Apart from SPT and serum Ig levels, the basophil activation test is another possible biomarker of wheat OIT treatment response, yet little has been researched in this area. These diagnostic fields present interesting questions for future research to address.
5.3.3. Precautions for OIT
Exercise should be avoided after wheat ingestion in individuals undergoing OIT, even in those who have achieved short-term SU, since they may be at risk of WDEIA or exhibit exercise-induced allergic reactions on desensitization (EIARDs). A study evaluating the two-year follow-up prognosis for WA patients who achieved short-term SU after receiving wheat OIT revealed six out of eight symptomatic patients experienced adverse allergic reactions after exercise and three of them developed anaphylaxis [85]. Studies reported that EIARDs occurred not only after rush OIT but also after slow OIT for wheat, with 66.7% (14/21) and 48.4% (15/31) of WA patients developing EIARDs respectively [86,87]. Therefore, exercising after wheat intake may be the primary trigger for allergic symptoms during or after OIT.
5.4. Other Therapeutic Approaches
The combination of biologics with food OIT is a heated research topic, yet the use of omalizumab that removes circulating IgE antibodies for wheat OIT has not been tested to date. A case report demonstrated that administering omalizumab three weeks before increasing the wheat dose helped achieve higher build-up doses [88]. Chinuki et al suggested that short-term (12 weeks) omalizumab inhibited wheat allergen-induced basophil activation in hydrolyzed wheat protein-allergy patients, but the effect diminished after treatment cessation [66]. In a long-term (48 weeks) omalizumab study involving 20 adult patients with WDEIA, over 80% of the subjects achieved a basophil activation rate of less than 10% against all fractionated wheat preparations, with 68.8% spared from any allergic reactions [67]. Further studies with larger sample sizes and controlled trials are needed to fully evaluate the efficacy of omalizumab in conjunction with wheat OIT. Meanwhile, several strategies have been proposed to improve outcomes in wheat OIT, including wheat modification, adjunct medications such as antihistamines or leukotriene antagonists, and probiotics [4], but the safety and effectiveness profiles of these treatments are yet to be presented.
6. Conclusions and Future Trends
IgE-mediated WA is characterized by an immune dysregulation leading to the release of inflammatory mediators from mast cells and basophils, with microbial dysbiosis also potentially playing a role in its pathogenesis. It can manifest as a spectrum of allergic reactions which impair individuals’ quality of life. For children with IgE-mediated WA, the prognosis is generally positive. The diagnosis of WA involves SPT and serum Ig measurement to wheat extracts, yet in view of their low specificity, novel approaches like alcohol-soluble extracts for SPT, component-resolved diagnosis and the basophil activation test are under research. While the principal management strategy for patients lies in dietary wheat avoidance, oral immunotherapy has recently emerged as a promising approach for treating WA, with trials using higher maintenance doses and extended durations showing increased rates of desensitization. Changes in SPT, sIgE and sIgG4 levels to wheat or ω-5 gliadin may help assess treatment efficacy, but the inconsistency in current published trials warrant further confirmation through large-scale studies. BAT could play a potential role in evaluating treatment effectiveness, although more research is needed. Lastly, integrating omalizumab as an adjunctive therapy to wheat OIT holds potential for enhancing OIT effectiveness and represents a future direction of research. Further studies are crucial to determine the optimal OIT protocol that would safely promote tolerance in children with WA.
Author Contributions
T.F. Leung conceptualized the topic and theme of this review. W. Zheng wrote the first draft of this manuscript. W. Zheng, C.Y.Y. Wai, J.K.C. Sit and N.S. Cheng collected and analyzed data. C.W.M. Leung performed extensive editing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Health and Medical Research Fund (reference 10210336), Health Bureau of Hong Kong SAR Government.
Institutional Review Board Statement
Not applicable for this review article.
Informed Consent Statement
Not applicable for this review article that does not involve any individual clinical data.
Data Availability Statement
Not applicable as this review article does not involve any research data.
Acknowledgments
We thank the funder for supporting our wheat allergy project.
Conflicts of Interest
All authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Longo G, Berti I, Burks AW, et al. IgE-mediated food allergy in children. Lancet. 2013, 382, 1656–1664. [Google Scholar] [CrossRef]
- Yu W, Freeland DMH, Nadeau KC. Food allergy: immune mechanisms, diagnosis and immunotherapy. Nat Rev Immunol. 2016, 16, 751–765. [Google Scholar] [CrossRef]
- Spolidoro GC, Ali MM, Amera YT, et al. Prevalence estimates of eight big food allergies in Europe: updated systematic review and meta-analysis. Allergy. 2023, 78, 2361–2417. [Google Scholar] [CrossRef]
- Liu M, Huang J, Ma S, et al. Allergenicity of wheat protein in diet: mechanisms, modifications and challenges. Food Res Int. 2023, 169, 112913. [Google Scholar] [CrossRef]
- Cabanillas, B. Gluten-related disorders: Celiac disease, wheat allergy, and nonceliac gluten sensitivity. Crit Rev Food Sci Nutr. 2020, 60, 2606–2621. [Google Scholar] [CrossRef]
- Berin MC, Sampson HA. Mucosal immunology of food allergy. Curr Biol. 2013, 23, R389–R400. [Google Scholar] [CrossRef]
- Tordesillas L, Berin MC, Sampson HA. Immunology of food allergy. Immunity. 2017, 47, 32–50. [Google Scholar] [CrossRef]
- Kanchongkittiphon W, Nopnipa S, Mathuranyanon R, et al. Characterization of gut microbiome profile in children with confirmed wheat allergy. Characterization of gut microbiome profile in children with confirmed wheat allergy. Asian Pac J Allergy Immunol. 2024. [CrossRef]
- Cianferoni, A. Wheat allergy: diagnosis and management. J Asthma Allergy. 2016, 9, 13–25. [Google Scholar] [CrossRef]
- Pacharn P, Vichyanond P. Immunotherapy for IgE-mediated wheat allergy. Hum Vaccin Immunother. 2017, 13, 2462–2466. [Google Scholar] [CrossRef]
- Paul WE, Zhu J. How are T(H)2-type immune responses initiated and amplified? Nat Rev Immunol. 2010, 10, 225–235.
- Lamiable O, Mayer JU, Munoz-Erazo L, et al. Dendritic cells in Th2 immune responses and allergic sensitization. Immunol Cell Biol. 2020, 98, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Ito T, Wang YH, Duramad O, et al. TSLP-activated dendritic cells induce an inflammatory T helper type 2 cell response through OX40 ligand. J Exp Med. 2005, 202, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Brandt EB, Munitz A, Orekov T, et al. Targeting IL-4/IL-13 signaling to alleviate oral allergen-induced diarrhea. J Allergy Clin Immunol. 2009, 123, 53–58. [Google Scholar] [CrossRef]
- Iwasaki, A. Mucosal dendritic cells. Annu Rev Immunol.
- de Jong NW, Wichers HJ. Update on nutrition and food allergy. Nutrients. 2022, 14. [Google Scholar]
- Eiwegger T, Hung L, San Diego KE, et al. Recent developments and highlights in food allergy. Allergy. 2019, 74, 2355–2367. [Google Scholar] [CrossRef] [PubMed]
- Stone KD, Prussin C, Metcalfe DD. IgE, mast cells, basophils, and eosinophils. J Allergy Clin Immunol. 2010, 125 (Suppl 2), S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Galli SJ, Tsai M. IgE and mast cells in allergic disease. Nat Med. 2012, 18, 693–704. [Google Scholar] [CrossRef]
- Oyoshi MK, Oettgen HC, Chatila TA, et al. Food allergy: insights into etiology, prevention, and treatment provided by murine models. J Allergy Clin Immunol. 2014, 133, 309–317. [Google Scholar] [CrossRef]
- Rekabi M, Arshi S, Bemanian MH, et al. Evaluation of a new protocol for wheat desensitization in patients with wheat-induced anaphylaxis. Immunotherapy. 2017, 9, 637–645. [Google Scholar] [CrossRef]
- Babaie D, Ebisawa M, Soheili H, et al. Oral wheat immunotherapy: long-term follow-up in children with wheat anaphylaxis. Int Arch Allergy Immunol. 2022, 183, 306–314. [Google Scholar] [CrossRef]
- Nagakura KI, Yanagida N, Sato S, et al. Low-dose-oral immunotherapy for children with wheat-induced anaphylaxis. Pediatr Allergy Immunol. 2020, 31, 371–379. [Google Scholar] [CrossRef]
- Burton OT, Logsdon SL, Zhou JS, et al. Oral immunotherapy induces IgG antibodies that act through FcγRIIb to suppress IgE-mediated hypersensitivity. J Allergy Clin Immunol. 2014, 134, 1310–1317. [Google Scholar] [CrossRef]
- van de Veen W, Stanic B, Yaman G, et al. IgG4 production is confined to human IL-10-producing regulatory B cells that suppress antigen-specific immune responses. J Allergy Clin Immunol. 2013, 131, 1204–1212. [Google Scholar] [CrossRef]
- Nouri-Aria KT, Wachholz PA, Francis JN, et al. Grass pollen immunotherapy induces mucosal and peripheral IL-10 responses and blocking IgG activity. J Immunol. 2004, 172, 3252–3259. [Google Scholar] [CrossRef]
- Gri G, Piconese S, Frossi B, et al. CD4+CD25+ regulatory T cells suppress mast cell degranulation and allergic responses through OX40-OX40L interaction. Immunity. 2008, 29, 771–781. [Google Scholar] [CrossRef]
- Hua X, Goedert JJ, Pu A, et al. Allergy associations with the adult fecal microbiota: Analysis of the American Gut Project. EBioMedicine. 2016, 3, 172–179. [Google Scholar] [CrossRef]
- Ling Z, Li Z, Liu X, et al. Altered fecal microbiota composition associated with food allergy in infants. Appl Environ Microbiol. 2014, 80, 2546–2554. [Google Scholar] [CrossRef]
- Zubeldia-Varela E, Barker-Tejeda TC, Obeso D, et al. Microbiome and allergy: new insights and perspectives. J Investig Allergol Clin Immunol. 2022, 32, 327–344. [Google Scholar] [CrossRef]
- Iweala OI, Nagler CR. The microbiome and food allergy. Annu Rev Immunol. 2019, 37, 377–403. [Google Scholar] [CrossRef] [PubMed]
- Bunyavanich S, Berin MC. Food allergy and the microbiome: current understandings and future directions. J Allergy Clin Immunol. 2019, 144, 1468–1477. [Google Scholar] [CrossRef]
- Tanaka M, Korenori Y, Washio M, et al. Signatures in the gut microbiota of Japanese infants who developed food allergies in early childhood. FEMS Microbiol Ecol. 2017, 93. [Google Scholar]
- Lozano-Ojalvo D, Berin C, Tordesillas L. Immune basis of allergic reactions to food. J Investig Allergol Clin Immunol. 2019, 29, 1–14. [Google Scholar] [CrossRef]
- Berni Canani R, Sangwan N, Stefka AT, et al. Lactobacillus rhamnosus GG-supplemented formula expands butyrate-producing bacterial strains in food allergic infants. Isme j. 2016, 10, 742–750. [Google Scholar] [CrossRef]
- Czaja-Bulsa G, Bulsa M. What do we know now about IgE-mediated wheat allergy in children? Nutrients. 2017, 9. [Google Scholar]
- Pasha I, Saeed F, Sultan MT, et al. Wheat allergy and intolerence: recent updates and perspectives. Crit Rev Food Sci Nutr. 2016, 56, 13–24. [Google Scholar] [CrossRef]
- Matsuo H, Dahlström J, Tanaka A, et al. Sensitivity and specificity of recombinant omega-5 gliadin-specific IgE measurement for the diagnosis of wheat-dependent exercise-induced anaphylaxis. Allergy. 2008, 63, 233–236. [Google Scholar] [CrossRef]
- Matricardi PM, Kleine-Tebbe J, Hoffmann HJ, et al. EAACI molecular allergology user's guide. Pediatr Allergy Immunol. 2016, 27 (Suppl 23), 1–250. [Google Scholar] [CrossRef]
- Faihs V, Kugler C, Schmalhofer V, et al. Wheat-dependent exercise-induced anaphylaxis: subtypes, diagnosis, and management. J Dtsch Dermatol Ges. 2023, 21, 1131–1135. [Google Scholar]
- Matsuo H, Morimoto K, Akaki T, et al. Exercise and aspirin increase levels of circulating gliadin peptides in patients with wheat-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2005, 35, 461–466. [Google Scholar] [CrossRef]
- Mizuno O, Nomura T, Ohguchi Y, et al. Loss-of-function mutations in the gene encoding filaggrin underlie a Japanese family with food-dependent exercise-induced anaphylaxis. J Eur Acad Dermatol Venereol. 2015, 29, 805–808. [Google Scholar] [CrossRef]
- Christensen MJ, Eller E, Mortz CG, et al. Wheat-dependent cofactor-augmented anaphylaxis: a prospective study of exercise, aspirin, and alcohol efficacy as cofactors. J Allergy Clin Immunol Pract. 2019, 7, 114–121. [Google Scholar] [CrossRef]
- Du Z, Gao X, Li J, et al. Clinical features and outcomes of patients with wheat-dependent exercise-induced anaphylaxis: a retrospective study. Allergy Asthma Clin Immunol. 2022, 18, 61. [Google Scholar] [CrossRef]
- Santos AF, Riggioni C, Agache I, et al. EAACI guidelines on the diagnosis of IgE-mediated food allergy. Allergy. 2023, 78, 3057–3076. [Google Scholar] [CrossRef]
- Ito K, Futamura M, Borres MP, et al. IgE antibodies to omega-5 gliadin associate with immediate symptoms on oral wheat challenge in Japanese children. Allergy. 2008, 63, 1536–1542. [Google Scholar] [CrossRef]
- Scibilia J, Pastorello EA, Zisa G, et al. Wheat allergy: a double-blind, placebo-controlled study in adults. J Allergy Clin Immunol. 2006, 117, 433–439. [Google Scholar] [CrossRef]
- Mäkelä MJ, Eriksson C, Kotaniemi-Syrjänen A, et al. Wheat allergy in children - new tools for diagnostics. Clin Exp Allergy. 2014, 44, 1420–1430. [Google Scholar] [CrossRef]
- Palosuo K, Varjonen E, Kekki OM, et al. Wheat omega-5 gliadin is a major allergen in children with immediate allergy to ingested wheat. J Allergy Clin Immunol. 2001, 108, 634–638. [Google Scholar] [CrossRef]
- Kulmala P, Pelkonen AS, Kuitunen M, et al. Wheat oral immunotherapy was moderately successful but was associated with very frequent adverse events in children aged 6-18 years. Acta Paediatr. 2018, 107, 861–870. [Google Scholar] [CrossRef]
- Phisitbuntoon T, Jirapongsananuruk O, Pacharn P, et al. A potential role of gliadin extract skin prick test in IgE-mediated wheat allergy. Asian Pac J Allergy Immunol. 2023, 41, 37–44. [Google Scholar]
- Pacharn P, Siripipattanamongkol N, Pannakapitak N, et al. Accuracy of in-house alcohol-dissolved wheat extract for diagnosing IgE-mediated wheat allergy. Asian Pac J Allergy Immunol. 2020, 38, 102–107. [Google Scholar]
- Pacharn P, Kumjim S, Tattiyapong P, et al. Identification of wheat sensitization using an in-house wheat extract in Coca-10% alcohol solution in children with wheat anaphylaxis. Asian Pac J Allergy Immunol. 2016, 34, 153–158. [Google Scholar]
- Constantin C, Quirce S, Poorafshar M, et al. Micro-arrayed wheat seed and grass pollen allergens for component-resolved diagnosis. Allergy. 2009, 64, 1030–1037. [Google Scholar] [CrossRef]
- Nilsson N, Nilsson C, Ekoff H, et al. Grass-allergic children frequently show asymptomatic low-level IgE co-sensitization and cross-reactivity to wheat. Int Arch Allergy Immunol. 2018, 177, 135–144. [Google Scholar] [CrossRef]
- Keet CA, Matsui EC, Dhillon G, et al. The natural history of wheat allergy. Ann Allergy Asthma Immunol. 2009, 102, 410–415. [Google Scholar] [CrossRef]
- Czaja-Bulsa G, Bulsa M. The natural history of IgE mediated wheat allergy in children with dominant gastrointestinal symptoms. Allergy Asthma Clin Immunol. 2014, 10, 12. [Google Scholar] [CrossRef]
- Tatham AS, Shewry PR. Allergens to wheat and related cereals. Clin Exp Allergy. 2008, 38, 1712–1726. [Google Scholar] [CrossRef]
- Park HJ, Kim JH, Kim JE, et al. Diagnostic value of the serum-specific IgE ratio of ω-5 gliadin to wheat in adult patients with wheat-induced anaphylaxis. Int Arch Allergy Immunol. 2012, 157, 147–150. [Google Scholar] [CrossRef]
- Scherf KA, Brockow K, Biedermann T, et al. Wheat-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2016, 46, 10–20. [Google Scholar] [CrossRef]
- Morita E, Matsuo H, Mihara S, et al. Fast omega-gliadin is a major allergen in wheat-dependent exercise-induced anaphylaxis. J Dermatol Sci. 2003, 33, 99–104. [Google Scholar] [CrossRef]
- Daengsuwan T, Palosuo K, Phankingthongkum S, et al. IgE antibodies to omega-5 gliadin in children with wheat-induced anaphylaxis. Allergy. 2005, 60, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Nilsson N, Sjölander S, Baar A, et al. Wheat allergy in children evaluated with challenge and IgE antibodies to wheat components. Pediatr Allergy Immunol. 2015, 26, 119–125. [Google Scholar] [CrossRef]
- Takahashi H, Matsuo H, Chinuki Y, et al. Recombinant high molecular weight-glutenin subunit-specific IgE detection is useful in identifying wheat-dependent exercise-induced anaphylaxis complementary to recombinant omega-5 gliadin-specific IgE test. Clin Exp Allergy. 2012, 42, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Gabler AM, Gebhard J, Eberlein B, et al. The basophil activation test differentiates between patients with wheat-dependent exercise-induced anaphylaxis and control subjects using gluten and isolated gluten protein types. Clin Transl Allergy. 2021, 11, e12050. [Google Scholar] [CrossRef] [PubMed]
- Chinuki Y, Yagami A, Adachi A, et al. In vitro basophil activation is reduced by short-term omalizumab treatment in hydrolyzed wheat protein allergy. Allergol Int. 2020, 69, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Chinuki Y, Kohno K, Hide M, et al. Efficacy and safety of omalizumab in adult patients with wheat-dependent exercise-induced anaphylaxis: Reduction of in vitro basophil activation and allergic reaction to wheat. Allergol Int. 2023, 72, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Sindher SB, Long A, Chin AR, et al. Food allergy, mechanisms, diagnosis and treatment: Innovation through a multi-targeted approach. Allergy. 2022, 77, 2937–2948. [Google Scholar] [CrossRef] [PubMed]
- Tokuda R, Nagao M, Hiraguchi Y, et al. Antigen-induced expression of CD203c on basophils predicts IgE-mediated wheat allergy. Allergol Int. 2009, 58, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Chinuki Y, Kaneko S, Dekio I, et al. CD203c expression-based basophil activation test for diagnosis of wheat-dependent exercise-induced anaphylaxis. J Allergy Clin Immunol. 2012, 129, 1404–1406. [Google Scholar] [CrossRef]
- Bahri R, Custovic A, Korosec P, et al. Mast cell activation test in the diagnosis of allergic disease and anaphylaxis. J Allergy Clin Immunol. 2018, 142, 485–496. [Google Scholar] [CrossRef]
- Leeds S, Liu EG, Nowak-Wegrzyn A. Wheat oral immunotherapy. Curr Opin Allergy Clin Immunol. 2021, 21, 269–277. [Google Scholar] [CrossRef]
- Tomsitz D, Biedermann T, Brockow K. Sublingual immunotherapy reduces reaction threshold in three patients with wheat-dependent exercise-induced anaphylaxis. Allergy. 2021, 76, 3804–3806. [Google Scholar] [CrossRef]
- Loke P, Orsini F, Lozinsky AC, et al. Probiotic peanut oral immunotherapy versus oral immunotherapy and placebo in children with peanut allergy in Australia (PPOIT-003): a multicentre, randomised, phase 2b trial. Lancet Child Adolesc Health. 2022, 6, 171–184. [Google Scholar] [CrossRef]
- Rodríguez del Río P, Díaz-Perales A, Sanchez-García S, et al. Oral immunotherapy in children with IgE-mediated wheat allergy: outcome and molecular changes. J Investig Allergol Clin Immunol. 2014, 24, 240–248. [Google Scholar]
- Sato S, Utsunomiya T, Imai T, et al. Wheat oral immunotherapy for wheat-induced anaphylaxis. J Allergy Clin Immunol. 2015, 136, 1131–1133. [Google Scholar] [CrossRef]
- Khayatzadeh A, Gharaghozlou M, Ebisawa M, et al. A Safe and Effective Method for Wheat Oral Immunotherapy. Iran J Allergy Asthma Immunol. 2016, 15, 525–535. [Google Scholar]
- Nowak-Węgrzyn A, Wood RA, Nadeau KC, et al. Multicenter, randomized, double-blind, placebo-controlled clinical trial of vital wheat gluten oral immunotherapy. J Allergy Clin Immunol. 2019, 143, 651–661. [Google Scholar] [CrossRef]
- Ogura K, Yanagida N, Sato S, et al. Evaluation of oral immunotherapy efficacy and safety by maintenance dose dependency: A multicenter randomized study. World Allergy Organ J. 2020, 13, 100463. [Google Scholar] [CrossRef]
- Nagakura KI, Yanagida N, Miura Y, et al. Long-term follow-up of fixed low-dose oral immunotherapy for children with wheat-induced anaphylaxis. J Allergy Clin Immunol Pract. 2022, 10, 1117–1119. [Google Scholar] [CrossRef]
- Sugiura S, Kitamura K, Makino A, et al. Slow low-dose oral immunotherapy: threshold and immunological change. Allergol Int. 2020, 69, 601–609. [Google Scholar] [CrossRef]
- Sharafian S, Amirzargar A, Gharagozlou M, et al. The efficacy of a new protocol of oral immunotherapy to wheat for desensitization and induction of tolerance. Iran J Allergy Asthma Immunol. 2022, 21, 232–240. [Google Scholar]
- Pourvali A, Arshi S, Nabavi M, et al. Sustained unresponsiveness development in wheat oral immunotherapy: predictive factors and flexible regimen in the maintenance phase. Eur Ann Allergy Clin Immunol. 2023, 55, 174–179. [Google Scholar] [CrossRef]
- 84. Christensen MJ, Eller E, Mortz CG, et al. Clinical and serological follow-up of patients with WDEIA. Clin Transl Allergy.
- Makita E, Yanagida N, Sato S, et al. Long-term prognosis after wheat oral immunotherapy. J Allergy Clin Immunol Pract. 2020, 8, 371–374. [Google Scholar] [CrossRef]
- Furuta T, Tanaka K, Tagami K, et al. Exercise-induced allergic reactions on desensitization to wheat after rush oral immunotherapy. Allergy. 2020, 75, 1414–1422. [Google Scholar] [CrossRef]
- Kubota S, Kitamura K, Matsui T, et al. Exercise-induced allergic reactions after achievement of desensitization to cow's milk and wheat. Pediatr Allergy Immunol. 2021, 32, 1048–1055. [Google Scholar] [CrossRef]
- Pacharn P, Siripipattanamongkol N, Veskitkul J, et al. Successful wheat-specific oral immunotherapy in highly sensitive individuals with a novel multirush/maintenance regimen. Asia Pac Allergy. 2014, 4, 180–183. [Google Scholar] [CrossRef]
Figure 1.
Pathophysiology of wheat allergy. Abbreviations: FcεRI, high-affinity IgE receptors; IgE, immunoglobulin E; IL, interleukin; OX40L, ligand for tumor necrosis factor receptor superfamily member 4; Th2, T helper 2; Treg, regulatory T; TSLP, thymic stromal lymphopoietin.
Figure 1.
Pathophysiology of wheat allergy. Abbreviations: FcεRI, high-affinity IgE receptors; IgE, immunoglobulin E; IL, interleukin; OX40L, ligand for tumor necrosis factor receptor superfamily member 4; Th2, T helper 2; Treg, regulatory T; TSLP, thymic stromal lymphopoietin.
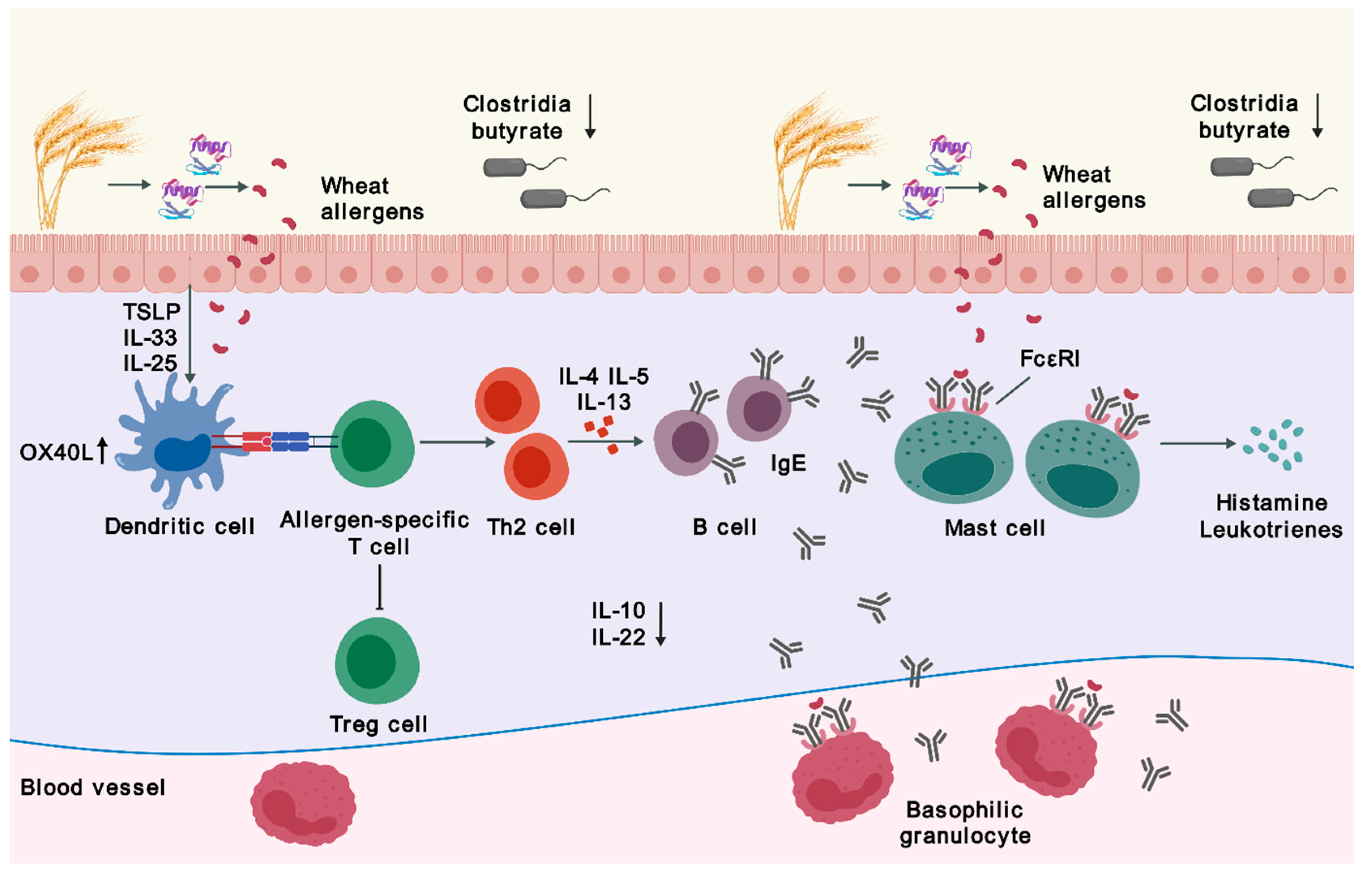
Figure 2.
Diagnostic algorithm of wheat allergy. Abbreviations: DBPCFC, double-blind, placebo-controlled food challenge; LTP, lipid transfer protein; OFC, oral food challenge; sIgE, serum immunoglobulin E; SPT, skin prick test.
Figure 2.
Diagnostic algorithm of wheat allergy. Abbreviations: DBPCFC, double-blind, placebo-controlled food challenge; LTP, lipid transfer protein; OFC, oral food challenge; sIgE, serum immunoglobulin E; SPT, skin prick test.
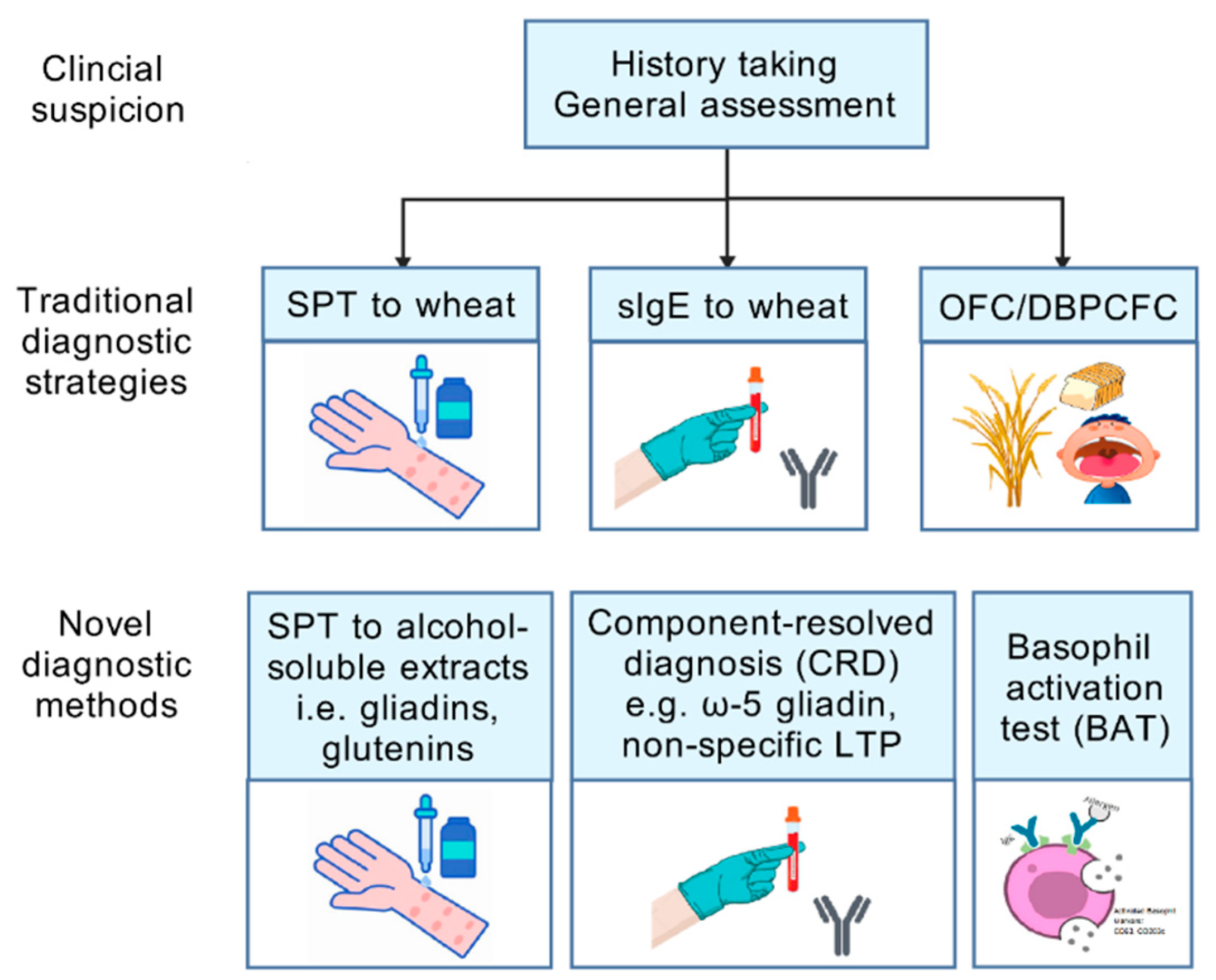
Figure 3.
Schematic view on study design of oral immunotherapy for wheat allergy. Abbreviations: DBPCFC, double-blind, placebo-controlled food challenge; g, gram; IgE, immunoglobulin E; IgG4, immunoglobulin G 4; OFC, oral food challenge.
Figure 3.
Schematic view on study design of oral immunotherapy for wheat allergy. Abbreviations: DBPCFC, double-blind, placebo-controlled food challenge; g, gram; IgE, immunoglobulin E; IgG4, immunoglobulin G 4; OFC, oral food challenge.
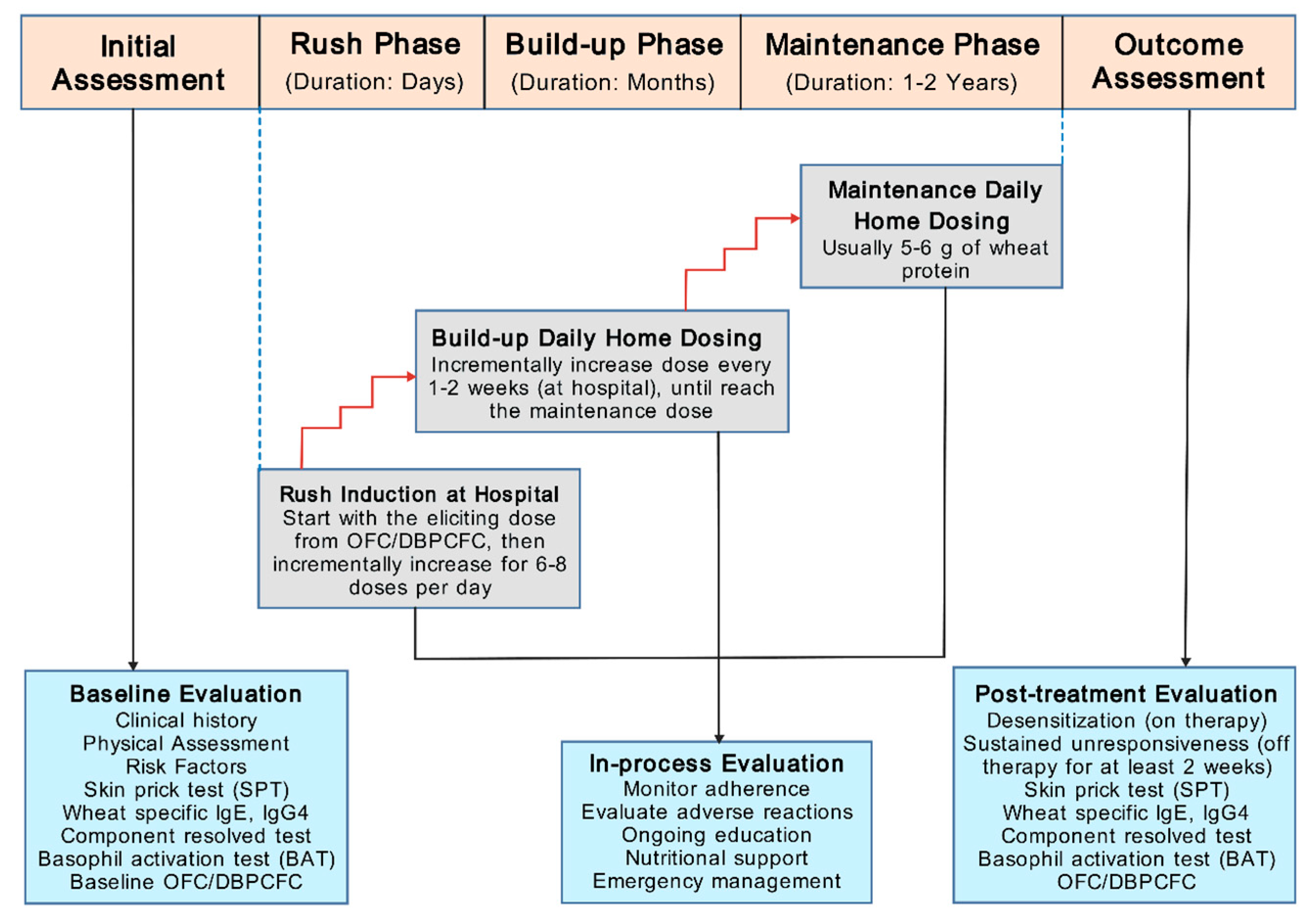

Table 1.
Overview of wheat oral immunotherapy trials.
| Study | Design | Patients treated with OIT, n | Age, mean (range) | Form ofwheat use | Up-dosing phase | Maintenance phase | Target dose | Changes in SPT scores(mean/median) | Changes in sIgE (mean/median) | Changes in sIgG(mean/median) | Efficacy after OIT, %desensitization | Efficacy after OIT, %sustained unresponsiveness | Adverse reaction (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rodríguez del Río (2014) [75] | Open-label,nonrandomized, no control | 6 | 5.5 (5-11) years | Semolina porridge andboiled semolina pasta | 3-24 days | 6 months | 13 g of WP | No significant changes but showed a trend (6 mm vs 2 mm) after 6 months | No significant changes in sIgE to wheat but showed a trend of increase after up-dosing, followed by a decrease after 6-month follow-up (47.5 vs 84.55 vs 28.75 kUA/L) | Increased sIgG4 and sIgG1 to wheat and a panel of wheat proteins in all patients after 6 months | 83% | Not assessed | 6.25% of doses during up-dosing, none treated with IM epi | |
| Sato (2015) [76] | Open-label,nonrandomized, historical control | 18 | 9.0 (5.9-13.6) years | Boiled udon noodles | 5 days | >3 months | 5.2 g of WP | Not assessed | Decreased sIgE to wheat (>100 vs 43.5 kU/L) after 2 years | Not assessed | 88.9% | OIT: 61.1%Historical control: 9.1% | 26.4% of inpatient doses, 6.8% of outpatient doses with 1 treated with IM epi | |
| Khayatzadeh (2016) [77] | Open-label,nonrandomizednon-placebo control | Rush method: n=8Outpatient method: n=5 | 7 (5.5-19) years | Bread | Rush method: 3-6 daysOutpatient method: 66-87 days | 3 months | 5.2 g of WP | Rush method: decreased (9 mm vs 6.6 mm) after 3 months;Outpatient method: decreased (9 mm vs 6.8 mm) after 5 months | Not available | Not assessed | 92.3% | Not assessed | Rush method: 29.6% of doses during up-dosing, with 5.6% treated with IM epiOutpatient method: 2.5% of doses during up-dosing, none treated with IM epi | |
| Rekabi (2017) [21] | Open-label,nonrandomized, no control | 12 | 2.25 (2-10) years | Semolina flour andspaghetti (containing pasta) | 6.5 months | 18 months | 70 g of pasta | Decreased (10 mm vs 3 mm) after 2 years | Decreased total IgE (490 vs 338.5 IU/mL) after 2 years.sIgE to wheat increased after desensitization, followed by a decrease after follow-up phase (55.9 vs 65.1 vs 4.6 IU/mL) | Not assessed | 100% | Not assessed | 0.06% of doses during up-dosing | |
| Kulmala (2018) [50] | Multicenter, open-label, nonrandomized, no control | 100 | 11.6 (6.1-18.6) years | Boiled wheat spaghetti | 4.3 months | 12 months | 2 g of WP | Not assessed | Three samples available showed decreased sIgE to wheat, gluten, and ω-5 gliadin after OIT | Not assessed | 57% | Not assessed | 94% of patients, 11 patients used 12 doses of IM epi | |
| Nowak-Węgrzyn (2019) [78] | Multicenter,double-blind,randomized,placebo-control | Low dose group: n=23Placebo group: n=23, then crossed-over to high dose after 1 year | 8.7 (4.2-22.3) years | Vital wheat gluten | 11 months | 2-14 months | Low dose: 1445 mg of WPHigh dose: 2748 mg of WP | No significant differences in SPT scores between groups at year 1 | No significant differences in sIgE to wheat and ω-5 gliadin between groups at year 1 | Increased sIgG4 to wheat and ω-5 gliadin in OIT group at year 1 | Placebo group: 0% after 1 year Low dose: 30.4% after 2 years;High dose: 57.1% after 1 year | Low dose: 13.0% after 2 years | Low dose: 15.4% of doses at year 1 with 0.08% treated with IM epi, 3.1% at year 2 and none treated with IM epi;High dose: 13.4% of doses after 1 year with 0.07% treated with IM epi | |
| Nagakura (2020) [23] | Open-label,nonrandomized,historical control | 16 | 6.7 (5.8-10.7) years | Boiled udon noodles | 1 month | 11 months | 53 mg of WP | Not assessed | Decreased sIgE to wheat (293 vs 153.5 kUA/L) and ω-5 gliadin (7.5 vs 4.1 kUA/L) after 1 year | Increased sIgG to wheat (19.8 vs 24.1 mgA/L) and ω-5 gliadin (6.0 vs 7.3 mgA/L) after 1 month. Increased sIgG4 to wheat (2.07 vs 4.7 mgA/L) and ω-5 gliadin (0.07 vs 0.09 mgA/L) after 1 month | 88% | OIT: 69%Historical control: 9% | 32.1% of inpatient doses and 4.1% of outpatient doses, none treated with IM epi | |
| Ogura (2020) [79] | Multicenter, open-label,randomized,non-placebo control | Low dose group: n=12High dose group: n=12 | Low dose group: 5.5 (4.5-5.8) yearsHigh dose group: 5.0 (3.7-5.5) years | Boiled udon noodles, boiled pasta and bread | 24 months | Low dose: 650 mg of WP; High dose: 2.6 g of WP | Not assessed | Decreased sIgE to wheat after 1 year in both groups and decreased sIgE to ω-5 gliadin in low dose group | No changes in sIgG and sIgG4 to wheat or ω-5 gliadin in both groups | Low dose group: 66.7%;High dose group: 33.3% at year 1 | Low dose group: 16.7% at year 1, 58.3% at year 2;High dose group: 50.0% at year 1, 58.3% at year 2 | Low dose group: 4.76% of doses with 0.02% treated with IM epi;High dose group: 8.82% of doses, none treated with IM epi | ||
| Sugiura (2020) [81] | Open-label,nonrandomized,non-placebo control | 35 | 5 (4-6) years | Boiled udon and somen noodles | 12 months | 10 times greater than the initial dose | Not assessed | Decreased sIgE to wheat (97.0 vs 51.9 UA/mL) and ω-5 gliadin (4.8 vs 1.4 UA/mL) after 12-15 months | Not assessed | OIT: 37.5%Control (wheat avoidance): 10.0% | Not assessed | 0.64% of doses, none treated with IM epi | ||
| Babaie (2022) [22] | Open-label,nonrandomized, no control | 20 | 6 (2-17) years | Cake and bread | Not mentioned | 3-27 months | 5.28 g of WP | Decreased (9.8 mm vs 4.3 mm) after 3-month maintenance phase | sIgE to wheat increased after up-dosing, followed by a decrease after 3-month maintenance phase | Not assessed | Not mentioned | 47.1% after 3 months, 82.4% after 15 months, 100% after 27 months | 7.2% of doses during up-dosing, with 0.4% treated with IM epi | |
| Nagakura (2022) [80] | Open-label,nonrandomized, historical control | 29 | 6.7 (6.3-7.9) years | Boiled udon noodles | 1 month | 35 months | 53 mg of WP | Not assessed | Decreased sIgE to wheat (278 vs 89.3 kUA/L), gluten (358 vs 86.9 kUA/L), and ω-5 gliadin (12.7 vs 3.5 kUA/L) after 3 years | Not assessed | 100% | OIT: 7% at year 1, 28% at year 2, 41% at year 3;Historical control: 0% | 7.7% of doses at year 1, 3.9% at year 2, 2.4% at year 3, and 0.03% treated with IM epi at year 1 | |
| Sharafian (2022) [82] | Open-label,nonrandomized, no control | 26 | 6.2 (4-11) years | Bread | 6 days | 12 months | 5.2 g of WP | Not assessed | Decreased sIgE to wheat (90.4 vs 66.5 IU/mL) after 1 year | Not assessed | 100% | 93.3% | 21.4% of doses, 23.8% of reactions treated with IM epi | |
| Pourvali (2023) [83] | Open-label,nonrandomized, no control | 19 | 6.6 (2.4-16.6) years | Bread and boiled spaghetti | 6-7.5 months | 7-9 months | 5-10 g of WP | No changes after OIT | Decreased sIgE to wheat (108 vs 24.6 kU/L) after OIT | No changes in sIgG4 to wheat after OIT | 68.4% | 68.4% | Not mentioned | |
Abbreviations: g, gram; IM epi, intramuscular epinephrine; mg, milligram; mm, millimeter; OIT, oral immunotherapy; sIgE, serum immunoglobulin E; sIgG, serum immunoglobulin G; SPT, skin prick test; WP, wheat protein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



