Submitted:
25 April 2024
Posted:
08 May 2024
You are already at the latest version
Abstract
People experiencing homelessness are at risk from a number of co-morbidities including traumatic brain injury, mental health disorders and various infections. Little is known about the rehabilitation needs of this population. This study took advantage of unique access to a specialist ‘Access’ GP practice for people experiencing homelessness and a local inclusion health initiative to explore the five year period prevalence of these conditions in a population of people experiencing homelessness, through electronic case record searches; and identify barriers and facilitators to healthcare provision for this population in the context of an interdisciplinary and multi specialist inclusion health team, through semi structured interviews with 12 staff working in primary and secondary care who interact with this population. The five year period prevalence of TBI, infections and mental health disorders was 9.5%, 4% and 22.8% respectively. Of those who had suffered a brain injury only 3, had accessed rehabilitation services. Themes from thematic analysis of interviews included: lack of resource, stigmatisation, under recognised multi-morbidity (including from brain injury) as barriers, trauma-informed, person-centred, adaptable, & integrated and collaborative models of care as facilitators. The combination of quantitative and qualitative data suggests a potential role for rehabilitation medicine in inclusion health initiatives.
Keywords:
rehabilitation
; traumatic brain injury
; inclusion health
; homelessness
; multimorbidity
1. Introduction
People experiencing homelessness (PEH) suffer from a variety of adverse healthcare outcomes, including (but not limited to); increased cardiovascular disease risk, increased risk of a variety of infectious diseases (tuberculosis/human immune deficiency virus/viral hepatitis C/ sexually transmitted infections), psychiatric diseases, and increased health service use more broadly [1,2,3,4,5]. PEH and vulnerably housed people also suffer from increased rates of traumatic brain injury (TBI), and cognitive impairment [4,5,6,7,8,9]. The association between TBI and homelessness is multifaceted, with some evidence suggesting that TBI may be a risk factor for becoming homeless, and brain injuries being associated with greater mortality, morbidity, and social exclusion including incarceration, in PEH [10,11,12,13,14,15]. Whilst there is a significant amount of literature detailing the health and social care needs of this population, there is less focus on identification of the rehabilitation needs of this population particularly in light of the increased prevalence of brain injury within this group.
Rehabilitation following brain injury has been proven to be an effective and cost-effective intervention [16,17]. Despite the recognition of the increased burden of TBI in people experiencing homelessness there is little consensus on how best to address this unmet need. Research looking into the rehabilitation needs of people experiencing homelessness has demonstrated high levels of physical limitation, cognitive and functional impairments. A scoping review also demonstrated there are existing programmes of rehabilitation targeting this population with opportunities to further tailor existing services to better meet the needs of people experiencing homelessness [18,19,20,21]. Policy guidance regarding the health of people experiencing homelessness, is clear that identification of brain injury, and management of its sequelae should be priority areas in inclusion health efforts [2,18]. Despite this, a recent review looking at clinical practice guidelines for management of brain injury, found a majority of guidelines did not have any special provision for management of brain injury in people who are experiencing homelessness [22]. This study took advantage of the unique access to a local specialist ‘access’ primary care provider, specialising in people experiencing homelessness and vulnerably housed people, and a local ‘in reach’ inclusion health service which had a presence in local acute hospitals.
The objectives of the study where to: 1) Estimate five year period prevalence of TBI, in a cohort of vulnerably housed people and people experiencing homelessness registered to a single specialist access primary care provider. 2) Explore the perceived barriers and facilitators to healthcare provision for people experiencing homelessness through interviews with professionals working in a specialist access GP practice for vulnerably housed and homeless individuals, a local brain injury rehabilitation service, and local inclusion health initiative.
2. Materials and Methods
2.1. Quantitative
A retrospective case-record analysis was performed on a cohort (n=2753) of individuals, registered to a single specialist access primary care provider. This involved performing electronic health record searches to determine the five year period prevalence of TBI, Infectious diseases associated with deprivation (HIV, viral hepatitis, tuberculosis and sexually transmitted infections), and mental health disorders (including substance misuse disorders). ICD-10 codes (see Appendix A) corresponding to these diagnoses where you used to identify relevant cases. Case record analysis was done in February 2023 by the e-Health team at the relevant local health board, NHS Lothian (see acknowledgement section) using a structured query language programme to access data from the local health board electronic health record database (TRAK Care ©). Five years was used as a cut off for ease of data extraction, and feasibility.
2.2. Qualitative:
Nine semi-structured face to face interviews were conducted with four nurses, two medical doctors, two occupational therapists, and one administrative staff member. Two interviews involved multiple participants. Interviewees worked across: a local access general practice, a local ‘in-reach; inclusion health service, and a local neurorehabilitation service. All interviews were conducted, using a template questionnaire that was constructed and agreed upon by all authors. Interviews explored the perceived barriers and facilitators to each individual service meeting their objectives, recognition of interaction of co-morbidities within their client group, and extent of collaboration with other services. A purposive and opportunistic approach to sampling was taken. This involved focusing on individuals known to work within local inclusion health and brain injury rehabilitation services, taking into account availability of potential interviewees. All interviews were recorded after prior consent being gained from interviewees. They were subsequently transcribed analysed using a thematic analysis [23] with an inductive approach, to generate themes. Coding, generation of initial themes, and further refinement was done through an iterative process involving four of the authors
3. Results
3.1. Quantitative
Demographic information was collected for the cohort of individuals registered to the access practice. (see Table 1). Of the 2753 patients in the cohort, 628 had at least one diagnosed mental health disorder, 262 had at least one episode of TBI, and 111 had a diagnosis of at least one infection associated with deprivation, within the last five years (five year % period prevalence of 22.8%, 9.5%, and 4% respectively – see Figure 1). Despite the prevalence of TBI, merely three people (0.11%) in the cohort had documented access to brain injury rehabilitation services during this period.
3.2. Qualitative Analysis
Several themes arose from thematic analysis of the qualitative interviews. The themes were broadly categorised into perceived barriers and enablers to health care provision for people experiencing homelessness. Barriers to healthcare provision that were identified included: ‘the perception of stigmatisation and the effect of psychological trauma’, ‘under recognition of the extent of multimorbidity of people experiencing homelessness by health professionals’, ‘lack of integration between services’, and ‘paucity of resources and high resource burden associated with marginalised populations’. Enablers to healthcare provision identified included: ‘trauma informed care’, ‘integrative and collaborative approaches to care’, and ‘patient-centred, adaptable models of care’.
4. Discussion
The prevalence of head mental health disorders and infections was consistent with previous studies [1,3,4]. The prevalence of brain injury in this cohort was also consistent with previous studies exploring TBI in people experiencing homelessness [2,6,7,10]. Previous literature largely relied on methodology based on self reports of head injury that may not necessarily be corroborated and easily verifiable. This is often further complicated if injuries occur in the context of intoxication, as is often the case in this population. Given the above limitations, a pragmatic approach was taken to identify cases of TBI through searching for ICD 10 clinical codes associated with a traumatic head injury (see table). It is possible that hospital episodes which included head injury in the context of polytrauma, or coincidence of head injury with other diagnoses may not have been coded to reflect this. Additionally the methodology used only captures hospital treated brain injury which may also contribute to underestimation due to individuals not presenting to secondary care services following head injury. The low number of individuals in the cohort accessing rehabilitation services following a TBI was particularly noteworthy. Whilst the benefits of rehabilitation following brain injury are becoming increasingly clear, there is little data on the demographic characteristics of patients accessing rehabilitation services. Several studies demonstrate significant functional impairment in people experiencing homelessness [8,20,24,25,26] and some studies have demonstrated some benefit from a rehabilitative approach focused on addressing functional impairments both due to brain injury and other causes.
Barriers to Healthcare Provision for PEH
The effect of psychological trauma and stigmatisation was identified in most interviews as a barrier to service delivery for PEH. There was a recognition that previous experiences and treatment of PEH by various services contributes to this. The lack of identification of this trauma, and appropriate response by healthcare staff, limit the potential therapeutic relationships that necessarily underpin health and social care. The impact of trauma andstigmatisation is explored in other qualitative studies exploring healthcare for PEH and more broadly [27,28,29,30,31].
“Many of our clients, particularly those with addictions, feel quite stigmatised. So, the environment in general can be quite difficult for them and just feeling they've got somebody there who's on their side and advocating for them can make a huge difference.” Inclusion Health Programme Manager
“ One of the biggest challenges is getting to engage in the 1st place, you know, just getting them to trust those services because that's been broken in the past, previous experiences in mainstream GP practices where they've stigmatised, and they've just turned away for the wee least outburst. Whereas, we have quite a high tolerance level for people's behaviour. I don't mean we accept really bad behaviour; we accept that somebody's in distress a lot more and we try.” Nurse at Access GP Practice
“Yes, so main obstacles ... a lot of mistrust like. A lot of people feel that they have had Negative experiences with other GP surgeries, and there have felt a lot of stigma, yeah. So, it's all about that trust building, isn't it?” Nurse Access GP Practice
Under recognition of the needs of PEH was recognised as a barrier. This was manifest in two ways. Firstly, there was expression of the perception that health services underestimate the extent of medical co-morbidity within this cohort. As stated by multiple interviewees the population of PEH has an extent of multi-morbidity usually associated with much older populations, however unlike the older population, they do not tend to have the same recognition of this among health care professionals. The impact of frailty secondary to multimorbidity has been explored in other studies [32,33].
“...the average age of death in Edinburgh if you're homeless is 41 for a woman and 47 for men,87% had morbidities of the same number as a cohort of the over 80s. So huge, huge multi-morbidity, very frail, but young cohort, and so all the services available to elderly patients, which are not available [to them].” Doctor working within local inclusion health ‘in reach’ service
Secondly, in the context of recognition of the sequelae of brain injury specifically, interviewees from various services noted a perception of underestimation of the prevalence of brain injury in this population. This lack of recognition may account for the relatively small numbers of PEH in the cohort who had access to rehabilitation services, and suggests a potential need for more comprehensive screening for the rehabilitation needs of PEH.
“I think brain injury in general is vastly under-recognized, if you compare it to something like stroke or maybe cancer services, you know you're talking about equally life changing illnesses and [they] also affect… usually affecting younger people. So, they are going to live with this for a longer period of time, so, no brain injury is vastly under-recognized and under-resourced, I would say...” Specialist Brain Injury Occupational Therapist
“...our inclusion health huddle on a wednesday, we have Hepatitis in reach, nurse drug liaison who are really important third sector. I mean, we haven't really thought about neurorehabilitation. But now I am...” Doctor working within local ‘in reach’ inclusion health service
“...people will often. Maybe not have been really assessed for a brain injury because if they have presented previously following an accident and self-discharged any assessments quite difficult...” Inclusion Health Programme Manager
The issue of resource is a pertinent one across the health service and cited by staff across various services as a barrier to care. This was manifest in the context of a recognition of limited resources for services providing care for people experiencing homelessness and other marginalised groups including people who had suffered brain injuries. There was a sense that a lack of adequate resources, was potentially leading to less positive outcomes for clients than might be achieved with more resource allocation. This view is supported by evidence from a study looking at health resource allocation and its impact on health inequalities in the UK [34].
“I think it’s true of all aspects of the NHS, but resources, you know, not having enough people to be able to see patients and have, you know, particularly people with quite significant cognitive impairment, you would want to be able to do repetition to try and support some need to improve and cope and build strategies, but if you don't, you're not able to do that repetition because you don't have adequate staffing to do that either as an inpatient or an outpatient. I think that leads to like skewed outcomes for patients.” Specialist Brain Injury Occupational Therapist
“Oh yes, we are always up to capacity. The difficulty is because we're a small team and we've had. In three years, we have had about 13 14 hundred referrals, so the difficulty we have is that we can offer that long term support to everybody.” Inclusion Health Programme Manager
Enablers of Healthcare Provision in PEH
Collaboration and integration were the major enabling factors identified in our analysis. This was the most consistent theme across services and throughout the interviews. Collaboration was a clear facilitator both within the context of viewing the care of patients as an endeavour requiring partnership and as an important factor for the various services involved with the population of PEH. Integration was recognised as an important factor within organisations, physically within buildings and across different organisations.
“..yes so there’s a number of different things, one of the challenges is they’ve got a lot of other pressures going on in their lives as well so if you're looking at health side of things we are now integrated with social work, health and housing which supposedly makes access a bit better.” Primary care doctor
Training in ‘trauma-informed care’ was seen as a major enabler in improving outcomes and care in this group of PEH. This approach is well recognised in other services and is clearly adopted in inclusion medicine. It involves a 5-stage approach: trauma awareness; safety and trustworthiness; choice and collaboration; building skills and resilience; recognition of wider cultural, historical, and gender issues (intersectionality) [35].
“Mental health is a big issue and anxiety, and I would argue that we try to be as trauma informed as we can and have started the whole process and becoming more trauma informed...” Nurse GP Access Practice
“I've done some trauma informed practise training of my own back.” Doctor working within local ‘in reach’ inclusion health service
“...we try to be as trauma informed as we can and you know have it, have started the whole process and becoming more trauma informed.”Doctor working within local ‘in reach’ inclusion health service
Patient-centred care is a core theme in many policy documents around organisation of healthcare services including rehabilitation services [36,37,38]. However, the extent to which patient-centred care is implemented in healthcare systems, including rehabilitation, is unclear [39]. The importance of centering patients and offering a degree of flexibility in care to ensure the needs of the most vulnerable are met, was emphasised by staff in multiple interviews. The importance of adopting a pro-active and flexible model to healthcare delivery was something that was cited as a strength within the collaborative inclusion health model which involved integration between various different teams working across in-patient, community healthcare, and social services. Rehabilitation services collaboration within such efforts may lead to further appropriate input with PEH in the context of rehabilitation following TBI, particularly noting the relative paucity of rehabilitation input identified from the quantitative aspect of the study.
“So, what healthcare can we deliver in an alternative setting in that situation?... So, we have to get rid of that gold standard treatment... those guidelines are written in without the patient really in mind. And if that's not tolerable, then what's the next best thing?” Doctor working within local ‘in reach’ inclusion health service
“There’s a lot of people who come incredibly sporadically who are most needy. Given we have an opportunistic service they might see housing, social work and health and the nurse and a welfare advisor all in one morning.” Nurse GP Access Practice
5. Conclusions
This study is unique in several ways: firstly it is novel in its approach of identification of TBI through clinical coding rather than reliance on self-reporting, as far as the authors are aware it is also the first to explore access to rehabilitation post brain injury in people experiencing homelessness. The authors mixed methodology approach allowed us to assess prevalence of TBI and other conditions whilst simultaneously gaining insights into the perceptions of the relationship between brain injury, other conditions, and homelessness. We believe that this study suggests a potential role for integration of brain injury rehabilitation services into existing pathways of inclusion health as a means of mitigating the significant level of morbidity within PEH and other marginalised groups at increased risk of brain injury. Rehabilitation medicine specialists’ focus on all aspects of disability (impairment, function & participation), and expertise makes the speciality particularly well suited to support inclusion health efforts in a holistic fashion traversing the biopsychosocial paradigm [40,41]. Such models coincide with the identified enablers to healthcare provision for people experiencing homelessness. The presence of embedded local inclusion health teams in primary care with a significant at risk population, provide a significant opportunity for further work to screen for TBI and its resultant impairments and design rehabilitation interventions with the aim of mitigating the effects of these. Further research combining qualitative and qualitative methodology should involve existing stakeholders, most importantly service users, to explore how this might best be acheived [42,43].
Author Contributions
Conceptualization, all authors. Methodology, all authors. Formal analysis, all authors. Investigation, data curation all authors ; writing—original draft preparation, Edwin Eshun, Alasdair FitzGerald; writing—review and editing, Edwin Eshun, Alasdair FitzGerald; supervision, Edwin Eshun, Alasdair FitzGerald. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Ethical review and approval were waived for this study due to the nature of the project being an undergraduate medical student selected component (SSC) as part of the MBBS degree programme which was supervised. The project was approved by the named medical school, the University of Edinburgh medical school, following submission of an ethics form from the supervising authors.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors would like to acknowledge the contributions of the eHealth Programmes & Development team at NHS Lothian, in particular Alistair Stewart and Andy Johnston, for their help in data collection for the quantitative aspect of the study.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
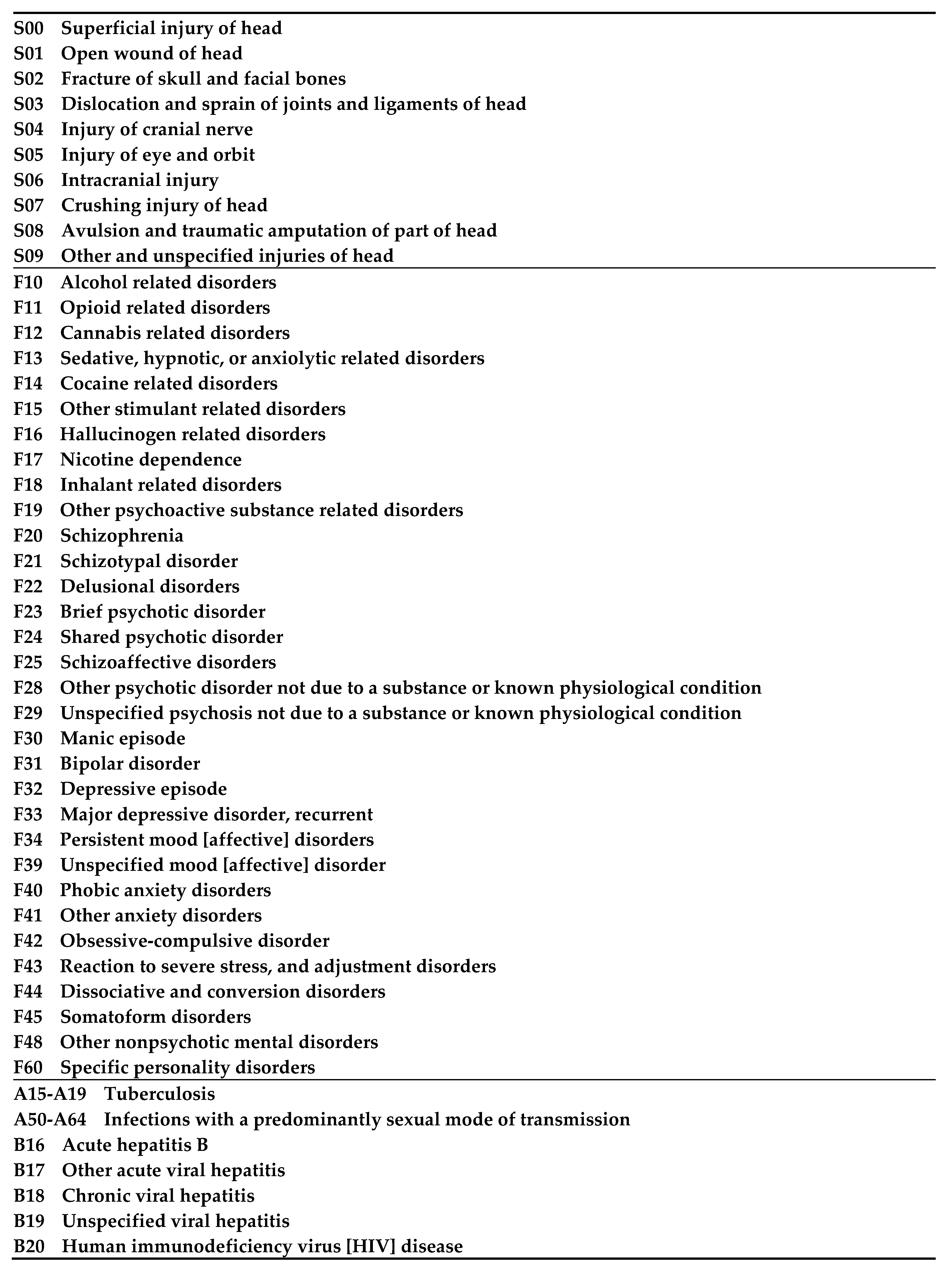
Figure A1.
ICD 10 Codes used to identify traumatic brain injury, mental disorders, and diseases associated with deprivation.
Figure A1.
ICD 10 Codes used to identify traumatic brain injury, mental disorders, and diseases associated with deprivation.
References
- Beijer U, Wolf A, Fazel S. Prevalence of tuberculosis, hepatitis C virus, and HIV in homeless people: a systematic review and meta-analysis. Lancet Infect Dis. 2012 Nov;12(11):859-70. Epub 2012 Aug 20. PMID: 22914343; PMCID: PMC3494003. [CrossRef]
- Fazel S, Geddes JR, Kushel M. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet. 2014 Oct 25;384(9953):1529-40. PMID: 25390578; PMCID: PMC4520328. [CrossRef]
- Fazel S, Khosla V, Doll H, Geddes J. The prevalence of mental disorders among the homeless in western countries: systematic review and meta-regression analysis. PLoS Med. 2008 Dec 2;5(12):e225. PMID: 19053169; PMCID: PMC2592351. [CrossRef]
- Williams SP, Bryant KL. Sexually Transmitted Infection Prevalence among Homeless Adults in the United States: A Systematic Literature Review. Sex Transm Dis. 2018 Jul;45(7):494-504. PMID: 29465661; PMCID: PMC6367672. [CrossRef]
- Luchenski S, Maguire N, Aldridge RW, Hayward A, Story A, Perri P, Withers J, Clint S, Fitzpatrick S, Hewett N. What works in inclusion health: overview of effective interventions for marginalised and excluded populations. Lancet. 2018 Jan 20;391(10117):266-280. Epub 2017 Nov 12. PMID: 29137868. [CrossRef]
- Oddy M, Moir JF, Fortescue D, Chadwick S. The prevalence of traumatic brain injury in the homeless community in a UK city. Brain Inj. 2012;26(9):1058-64. Epub 2012 May 9. PMID: 22571822. [CrossRef]
- Stubbs JL, Thornton AE, Sevick JM, Silverberg ND, Barr AM, Honer WG, Panenka WJ. Traumatic brain injury in homeless and marginally housed individuals: a systematic review and meta-analysis. Lancet Public Health. 2020 Jan;5(1):e19-e32. Epub 2019 Dec 2. Erratum in: Lancet Public Health. 2019 Dec 18;: PMID: 31806487. [CrossRef]
- Mahmood Z, Vella L, Maye JE, Keller AV, Van Patten R, Clark JMR, Twamley EW. Rates of Cognitive and Functional Impairments Among Sheltered Adults Experiencing Homelessness. Psychiatr Serv. 2021 Mar 1;72(3):333-337. Epub 2021 Jan 5. PMID: 33397143; PMCID: PMC7952028. [CrossRef]
- Stone B, Dowling S, Cameron A. Cognitive impairment and homelessness: A scoping review. Health Soc Care Community. 2019 Jul;27(4):e125-e142. Epub 2018 Nov 13. PMID: 30421478; PMCID: PMC6849546. [CrossRef]
- Topolovec-Vranic J, Ennis N, Colantonio A, Cusimano MD, Hwang SW, Kontos P, Ouchterlony D, Stergiopoulos V. Traumatic brain injury among people who are homeless: a systematic review. BMC Public Health. 2012 Dec 8;12:1059. PMID: 23216886; PMCID: PMC3538158. [CrossRef]
- Dell KC, Staph J, Hillary FG. Traumatic brain injury in the homeless: health, injury mechanisms, and hospital course. Brain Inj. 2021 Aug 24;35(10):1192-1200. Epub 2021 Aug 30. PMID: 34460346. [CrossRef]
- McMillan TM, Laurie M, Oddy M, Menzies M, Stewart E, Wainman-Lefley J. Head injury and mortality in the homeless. J Neurotrauma. 2015 Jan 15;32(2):116-9. Epub 2014 Oct 9. PMID: 25010750. [CrossRef]
- To MJ, OʼBrien K, Palepu A, Hubley AM, Farrell S, Aubry T, Gogosis E, Muckle W, Hwang SW. Healthcare Utilization, Legal Incidents, and Victimization Following Traumatic Brain Injury in Homeless and Vulnerably Housed Individuals: A Prospective Cohort Study. J Head Trauma Rehabil. 2015 Jul-Aug;30(4):270-6. PMID: 24651000. [CrossRef]
- Mackelprang JL, Harpin SB, Grubenhoff JA, Rivara FP. Adverse outcomes among homeless adolescents and young adults who report a history of traumatic brain injury. Am J Public Health. 2014 Oct;104(10):1986-92. Epub 2014 Aug 14. PMID: 25122029; PMCID: PMC4167112. [CrossRef]
- Hwang SW, Colantonio A, Chiu S, Tolomiczenko G, Kiss A, Cowan L, Redelmeier DA, Levinson W. The effect of traumatic brain injury on the health of homeless people. CMAJ. 2008 Oct 7;179(8):779-84. PMID: 18838453; PMCID: PMC2553875. [CrossRef]
- Turner-Stokes L, Pick A, Nair A, Disler PB, Wade DT. Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database Syst Rev. 2015 Dec 22;2015(12):CD004170. PMID: 26694853; PMCID: PMC8629646. [CrossRef]
- Turner-Stokes L, Williams H, Bill A, Bassett P, Sephton K. Cost-efficiency of specialist inpatient rehabilitation for working-aged adults with complex neurological disabilities: a multicentre cohort analysis of a national clinical data set. BMJ Open. 2016 Feb 24;6(2):e010238. PMID: 26911586; PMCID: PMC4769383. [CrossRef]
- Chan V, Estrella MJ, Baddeliyanage R, Shah R, Babineau J, Colantonio A. Rehabilitation among individuals experiencing homelessness and traumatic brain injury: A scoping review. Front Med (Lausanne). 2022 Nov 11;9:916602. PMID: 36438043; PMCID: PMC9692012. [CrossRef]
- Carroll Á, O'Brien S, Harrington D, Cheallaigh CN, Lawlee AM, Sukumar P. The Unmet Rehabilitation Needs in an Inclusion Health Integrated Care Programme for Homeless Adults in Dublin, Ireland. Int J Environ Res Public Health. 2021 Jul 27;18(15):7917. PMID: 34360210; PMCID: PMC8345505. [CrossRef]
- Mahmood Z, Vella L, Maye JE, Keller AV, Van Patten R, Clark JMR, Twamley EW. Rates of Cognitive and Functional Impairments Among Sheltered Adults Experiencing Homelessness. Psychiatr Serv. 2021 Mar 1;72(3):333-337. Epub 2021 Jan 5. PMID: 33397143; PMCID: PMC7952028. [CrossRef]
- Kiernan S, Mockler D, Ní Cheallaigh C, Broderick J. Physical functioning limitations and physical activity of people experiencing homelessness: A scoping review. HRB Open Res. 2021 Mar 1;3:14. PMCID: PMC7934094. [CrossRef]
- Chan V, Estrella MJ, Hanafy S, Colclough Z, Joyce JM, Babineau J, Colantonio A. Equity considerations in clinical practice guidelines for traumatic brain injury and homelessness: a systematic review. EClinicalMedicine. 2023 Aug 24;63:102152.
- Virginia Braun & Victoria Clarke (2006) Using thematic analysis in psychology, Qualitative Research in Psychology, 3:2, 77-101. [CrossRef]
- Brown RT, Guzman D, Kaplan LM, Ponath C, Lee CT, Kushel MB. Trajectories of functional impairment in homeless older adults: Results from the HOPE HOME study. PLoS One. 2019 Aug 13;14(8):e0221020. PMID: 31408488; PMCID: PMC6692032. [CrossRef]
- Ennis N, Roy S, Topolovec-Vranic J. Memory impairment among people who are homeless: a systematic review. Memory. 2015;23(5):695-713. Epub 2014 Jun 9. PMID: 24912102. [CrossRef]
- Cimino T, Steinman MA, Mitchell SL, Miao Y, Bharel M, Barnhart CE, Brown RT. The Course of Functional Impairment in Older Homeless Adults: Disabled on the Street. JAMA Intern Med. 2015 Jul;175(7):1237-9. PMID: 26011591; PMCID: PMC4494897. [CrossRef]
- Purkey E, MacKenzie M. Experience of healthcare among the homeless and vulnerably housed a qualitative study: opportunities for equity-oriented health care. Int J Equity Health. 2019 Jul 1;18(1):101. PMID: 31262310; PMCID: PMC6604349. [CrossRef]
- Nyblade L, Stockton MA, Giger K, Bond V, Ekstrand ML, Lean RM, Mitchell EMH, Nelson RE, Sapag JC, Siraprapasiri T, Turan J, Wouters E. Stigma in health facilities: why it matters and how we can change it. BMC Med. 2019 Feb 15;17(1):25. PMID: 30764806; PMCID: PMC6376713. [CrossRef]
- Reilly J, Ho I, Williamson A. A systematic review of the effect of stigma on the health of people experiencing homelessness. Health Soc Care Community. 2022 Nov;30(6):2128-2141. Epub 2022 Jun 28. PMID: 35762196. [CrossRef]
- Martins DC. Experiences of homeless people in the health care delivery system: a descriptive phenomenological study. Public Health Nurs. 2008 Sep-Oct;25(5):420-30. PMID: 18816359. [CrossRef]
- Pendyal A, Rosenthal MS, Spatz ES, Cunningham A, Bliesener D, Keene DE. "When you're homeless, they look down on you": A qualitative, community-based study of homeless individuals with heart failure. Heart Lung. 2021 Jan-Feb;50(1):80-85. Epub 2020 Aug 10. PMID: 32792114; PMCID: PMC7738391. [CrossRef]
- Suh K, Beck J, Katzman W, Allen DD. Homelessness and rates of physical dysfunctions characteristic of premature geriatric syndromes: systematic review and meta-analysis. Physiother Theory Pract. 2022 Jul;38(7):858-867. Epub 2020 Aug 24. PMID: 32835565. [CrossRef]
- Mantell R, Hwang YIJ, Radford K, Perkovic S, Cullen P, Withall A. Accelerated aging in people experiencing homelessness: A rapid review of frailty prevalence and determinants. Front Public Health. 2023 Mar 16;11:1086215. PMID: 37006541; PMCID: PMC10061143. [CrossRef]
- Barr B, Bambra C, Whitehead M. The impact of NHS resource allocation policy on health inequalities in England 2001-11: longitudinal ecological study. BMJ. 2014 May 27;348:g3231. PMID: 24865459; PMCID: PMC4035504. [CrossRef]
- Purkey E, Patel R, Phillips SP. Trauma-informed care: Better care for everyone. Can Fam Physician. 2018 Mar;64(3):170-172. PMID: 29540379; PMCID: PMC5851387.
- Coulter A, Oldham J. Person-centred care: what is it and how do we get there? Future Hosp J. 2016 Jun;3(2):114-116. PMID: 31098200; PMCID: PMC6465833. [CrossRef]
- Fernandes JB, Vareta D, Fernandes S, Almeida AS, Peças D, Ferreira N, Roldão L. Rehabilitation Workforce Challenges to Implement Person-Centered Care. Int J Environ Res Public Health. 2022 Mar 8;19(6):3199. PMID: 35328886; PMCID: PMC8950126. [CrossRef]
- Terry G, Kayes N. Person centered care in neurorehabilitation: a secondary analysis. Disabil Rehabil. 2020 Aug;42(16):2334-2343. Epub 2019 Jan 29. PMID: 30696295. [CrossRef]
- Cummins C, Payne D, Kayes NM. Governing neurorehabilitation. Disabil Rehabil. 2022 Aug;44(17):4921-4928. Epub 2021 May 14. PMID: 33989096. [CrossRef]
- Wade DT. What is rehabilitation? An empirical investigation leading to an evidence-based description. Clin Rehabil. 2020 May;34(5):571-583. Epub 2020 Feb 10. PMID: 32037876; PMCID: PMC7350200. [CrossRef]
- Janette McDougall , Virginia Wright & Peter Rosenbaum (2010) The ICF model of functioning and disability: Incorporating quality of life and human development, Developmental Neurorehabilitation, 13:3, 204-211. [CrossRef]
- Jagpal P, Saunders K, Plahe G, Russell S, Barnes N, Lowrie R, Paudyal V. Research priorities in healthcare of persons experiencing homelessness: outcomes of a national multi-disciplinary stakeholder discussion in the United Kingdom. Int J Equity Health. 2020 Jun 5;19(1):86. PMID: 32503544; PMCID: PMC7275401. [CrossRef]
- Gunner E, Chandan SK, Marwick S, Saunders K, Burwood S, Yahyouche A, Paudyal V. Provision and accessibility of primary healthcare services for people who are homeless: a qualitative study of patient perspectives in the UK. Br J Gen Pract. 2019 Aug;69(685):e526-e536. Epub 2019 Jul 15. PMID: 31307999; PMCID: PMC6650120. [CrossRef]
Figure 1.
Five year period prevalence of Infectious Diseases, Traumatic Brain Injury and Mental Health disorders among cohort (n=2753).
Figure 1.
Five year period prevalence of Infectious Diseases, Traumatic Brain Injury and Mental Health disorders among cohort (n=2753).
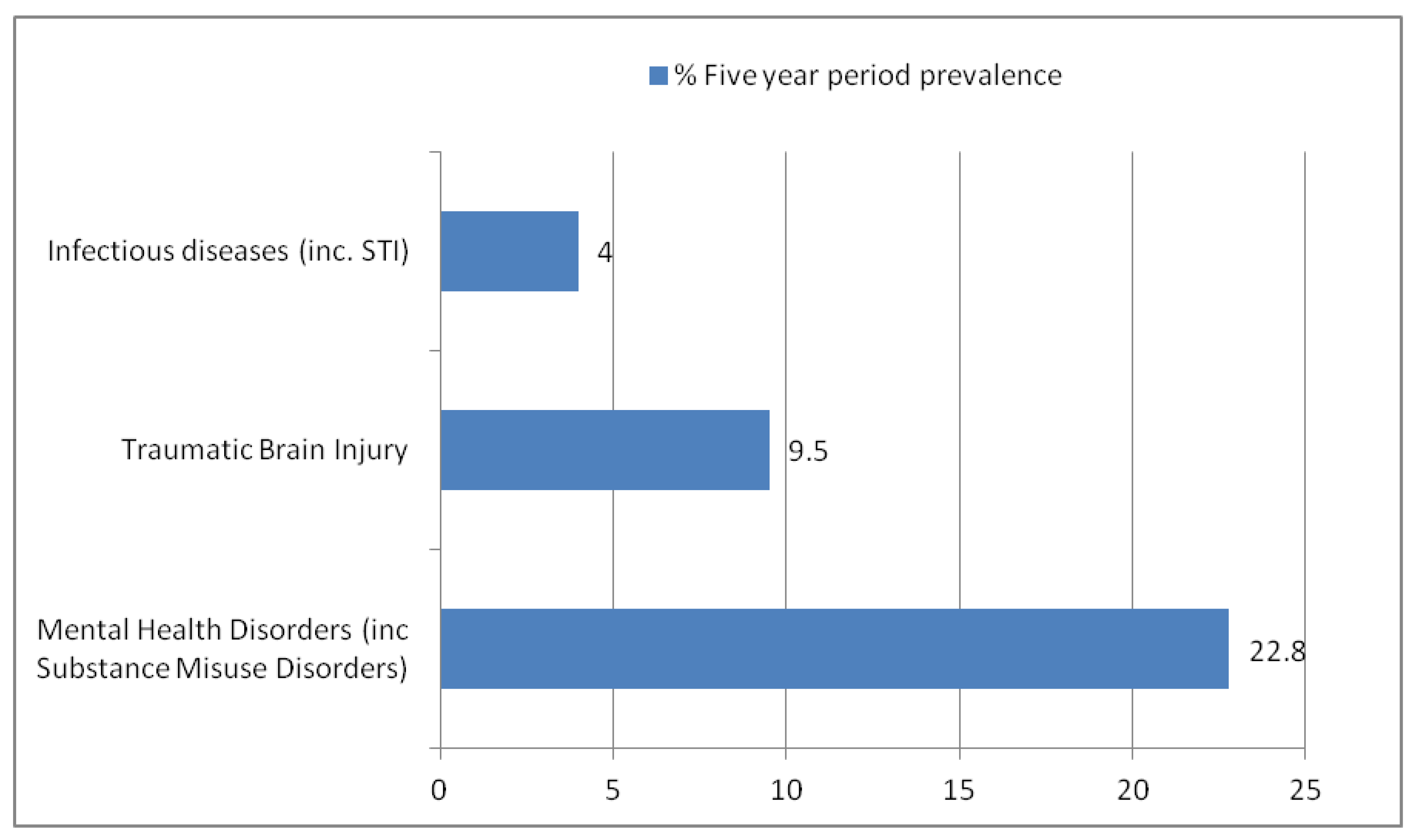

Table 1.
Demographic Information of Access GP Practice Patient Cohort (n=2753).
| Ratio of Female:Male | 1:3.1* |
| Average age | 47 |
| Ethnicity** |
African, African Scottish or African British - 11 Any mixed or multiple ethnic group – 9 Any other white ethnic group - 17 Arab - 1 Australasia (Australia, New Zealand) -2 Bangladeshi, Bangladeshi Scottish or Bangladeshi British -1 Black, Black Scottish or Black British – 5 Chinese – 1 Chinese, Chinese Scottish or Chinese British – 4 E Europe exc Poland (eg Balkans, Russia) – 36 Indian, Indian Scottish or Indian British – 1 N Europe (eg Denmark, Norway, Sweden) – 2 Other Asian – 4 Other Black – 5 Pakistani, Pakistani Scottish or Pakistani British – 2 S Europe (eg Cyprus, Greece, Italy, Spain, Turkey) – 16 W Europe (eg France, Germany, Netherlands) – 6 White British – 238 White English – 30 White Irish – 8 White Northern Irish – 2 White Scottish – 532 White Welsh – 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



