Submitted:
28 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
Handwriting abnormalities in children with attention deficit hyperactivity disorder (ADHD) have sometimes been reported both (i) at product level (i.e., quality/legibility of the written trace and speed of writing) and (ii) at process level (i.e., dynamic and kinematic features such as on-paper and in-air durations, pen pressure and velocity peaks, etc.). Conversely, other works have failed to reveal any differences between ADHD and typically developing children. The question of the presence and nature of handwriting disorders in ADHD remains open and merits an in-depth examination. The aim of this systematic review was therefore to identify studies investigating the product and/or process of handwriting in children with ADHD compared with typically developing individuals. This review was conducted and reported in accordance with the PRISMA statement. A literature search was carried out using three electronic databases. The methodological quality of the studies was systematically assessed using Critical Appraisal Skills Program (CASP) criteria. Twenty-one articles were identified. Of these, 17 described handwriting quality/legibility, 12 focused on speed and 14 analyzed the handwriting process. All studies (100%) with satisfactory methodology procedures reported impaired product and process in children with ADHD while 25% evidenced difference in speed of production. Most importantly, the studies differed widely in their methodological approach. Substantial gaps remain, particularly with regard to ascertaining comorbidities, ADHD subtypes and the medical status of included children. The lack of overall homogeneity in samples calls for higher quality studies. We conclude with recommendations for further studies.

Keywords:
ADHD
; Handwriting
; Dysgraphia
; Product of handwriting
; Process of handwriting
1. Introduction
1.1. Attention Deficit Hyperactivity Disorder (ADHD)
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by marked symptoms of inattention and/or impulsivity-hyperactivity (APA, 2015; Faraone et al., 2015) in children with preserved intellectual abilities in the absence of any physical or sensory abnormalities. ADHD affects around 5-7% of children (Willcutt, 2012; Polanczyk et al., 2014; Thomas et al., 2015) and involves developmentally extreme and cross-situational displays of (a) inattention and/or (b) hyperactivity–impulsivity that manifest in more than one setting (e.g., home, school, sport, leisure or other social environments). The DSM-5 criteria define four presentations of ADHD: inattentive (ADHD/I), hyperactive-impulsive (ADHD/HI) and combined presentations (ADHD/C). Other forms will be classified as unspecified ADHD.
It is a lifelong disorder and around one child out of two will still experience symptoms in adolescence and adulthood (Fayyad et al., 2017; Polanczyk et al., 2015). Neurodevelopmental etiology is no longer debated (Breda et al., 2020; Faraone et al., 2021) although many environmental risk factors are known to interact with genetic susceptibility (Faraone et al., 2010). Comorbidities are common (Tistarelli et al., 2020) with Autism Spectrum Disorders (ASD), psycho-emotional disturbances or Developmental Coordination Disorder (DCD) being the best known examples. Children with ADHD often experience significant academic impairments (Daley et al., 2010) and 45% meet the criteria for a comorbid learning disability (DuPaul et al., 2013; Tannock, 2013).
1.2. Handwriting Disorders in ADHD
Among learning difficulties, researchers have been paying increasing attention in recent years to handwriting disorders which often include lack of legibility in letter form production, spacing, spelling, syntactic and composition disturbances whether or not associated with insufficient speed production. These characteristics are generally encapsulated under the generic term "dysgraphia". However, some authors have suggested a more precise definition for this disorder which is mainly based on having impaired letter form production through hand and is therefore focused on quality/legibility (e.g., Berninger et al., 2015). In line with this perspective, Hamstra-Bletz & Blöte (1993) had already defined dysgraphia as a written language disorder which affects mechanical writing skills in children with no distinct neurological deficit.
Currently, dysgraphia diagnosis implies handwriting product and process evaluation (Figure 1). Product refers to the static features of the written trace such as letter form and size, spatial organization of the text, number of erasures, etc. A quantitative measure of handwriting speed is also considered, mainly based on the number of characters written in a given period of time. The process of handwriting describes the analysis of dynamic and kinematic components involved in the movement of writing. A number of variables can be analyzed: cognitive abilities (e.g., working memory, inhibition) posture, finger and arm movements, pen grip and finger pressure on the pen, in-air and on-paper durations, pen velocity, pen pressure, etc. Several handwriting processes can be assessed via digitizing tablets as has been done in a growing number of studies (e.g., Asselborn et al., 2020; Guilbert et al., 2019; Rosenblum & Dror, 2016).
Some studies suggest that 50 to 70% of ADHD children demonstrate disturbances in handwriting legibility and speed (Brossard-Racine et al., 2008; Brossard-Racine et al., 2015; Graham et al., 2016; Mayes et al., 2018). Greater variability, slowness of writing, poor rhythm and flow of writing, poor organization of written material, poor alignment, poor overall legibility, pronounced variability in spatial components, poor spacing within and between words, poorly formed letters, inconsistent letter size and shape, letter omissions, insertions, inversions or substitutions, frequent omissions of words or frequent erasures have all been reported (see Kaiser et al., 2015; Graham et al., 2016; Lelong et al., 2021 for a review). However, when examining these studies more in detail, it becomes apparent that they provide unclear or even discordant results. One striking example concerns writing speed: the conclusions drawn from a comparison between ADHD and typically developing children are contradictory. Some works demonstrated no difference (Shen et al., 2012) while others found that children with ADHD write more slowly (Adi-Japha et al., 2007; Brossard-Racine et al., 2011; Hung & Chang, 2022; Tucha & Lange, 2004). Others studies even revealed that children with ADHD write faster (Rosenblum, Epsztein & Josman, 2008; Brossard-Racine et al., 2008). How can such results be explained? Are the studies really comparable? Are there confounding variables that the authors did not consider? In addition, it seems difficult to extract the exact number of ADHD children who display handwriting impairment due to the apparent paucity of studies examining this aspect. Finally, the fact that several studies evaluated ADHD children who were on medication while others did not adds confusion to the overall picture because handwriting skills may be sensitive to methylphenidate (Brossard-Racine et al., 2008; Brossard-Racine et al., 2012).
1.3. Aim of the Systematic Review
Taken together, there is partial evidence for handwriting abnormalities in subjects with ADHD although results are often equivocal, maintaining a certain vagueness. A systematic review was therefore needed to examine the quality of the evidence as well as include relevant studies up to 2023 that used paper-and-pen assessment, questionnaires and/or digitizing tablets. To sum up, the specific objectives of the present work were to: (i) conduct a systematic review of the ADHD literature focusing on handwriting skills; (ii) examine the methodological quality of the relevant studies; (iii) describe whether the evidence for a deficit in handwriting product and process is convincing enough to conclude that children with ADHD have dysgraphia; (iv) determine whether all children with ADHD are affected and; (v) make informed recommendations for future research.
2. Method
2.1. Search Strategy
To include all relevant articles in this systematic review, a search was carried out using the PubMed, Web of Science and CENTRAL electronic databases with no restrictions on the year of publication and only limited to English language articles. We selected these databases for their broad spectrum of disciplines which regularly publish research pertinent to the topic of this review in ADHD. Manual searches were also conducted to find further references of appropriate articles. The final search included publications dating to September 2023. The following keywords were inputted: “("handwriting" OR "dysgraphia" OR "written production" OR "fine motor abilities" OR "fine motor skills") AND ("attention deficit hyperactivity disorder" OR "ADHD") AND ("children" NOT "adults").
2.2. Identification
The database search pinpointed a total of 814 records. After removing duplicates (n=61), a total of 753 records were identified. On the basis of abstract, title and in- and exclusion criteria, 36 potentially relevant articles were recognized. Based on full-text, 16 of these 36 were selected for this systematic review and were supplemented with 5 articles found in the reference lists. This resulted in a total of 21 included articles. Twenty were case control studies while one was a retrospective cohort-based study. Details can be found in the flow chart of included and excluded studies (Figure 2).
2.3. Study Selection
An evaluation of titles and abstracts was conducted to decide whether or not the articles were eligible for the review. The inclusion criteria were that publications had to: (1) report data linked to handwriting characteristics in children with ADHD regarding product and/or process (e.g., legibility, spatial components, correction errors, letters size, speed of handwriting, amplitude of movement, in-air time and other kinematic features, pen pressure, etc.); (2) contain data on handwriting characteristics whether or not the children had taken methylphenidate and regardless of the presentation of ADHD (e.g., inattentive or hyperactive-impulsive presentation) and; (3) provide a comparison between children with formal diagnosis of ADHD according to international criteria (e.g., based on DSM-5, APA, 2013) and a typically developing control group. Exclusion criteria were: (1) qualitative and case studies; (2) no handwriting measures; (3) absence of typically developing control group; (4) absence of formal diagnosis of ADHD and; (5) subjects older than 18 years of age.
2.4. Methodological Quality
All included publications were evaluated using the Critical Appraisal Skills Program (CASP) dedicated to experimental studies (CASP, 2010). The CASP questionnaire enables assessment of study validity via three main sections asking the following questions: 1) Are the results of the study valid? (Section A); 2) What are the results (Section B); 3) Would the results help locally? (Section C). In this way, methodological quality, presentation of results and external validity are systematically examined in order to check whether comparisons may reasonably be made from one study to another if necessary. A few adaptations have been proposed in terms of formulation for acquiring a rapid answer (Yes, No, or Can’t Tell) to the questions which are listed in Table 1. Results of validity between studies are displayed in Table 2.
3. Results
Characteristics of the included studies are presented in Table 3, with first author, year of publication, sample size, mean age, gender, inclusion and exclusion criteria, ADHD presentation, medication state, and handwriting measures. Statistically significant main results are reported in Table 4. Figure 3 provides a quick summary as to whether product and/or process are impaired in children with ADHD when compared to typically developing subjects.
For each domain (product and process of writing), the study characteristics, methodological quality and results are discussed. Questions 6 (Have the authors taken account of the potential confounding factors in the design and/or in their analysis?) and 9 (Do you believe the results?) on the CASP checklist were essential to decide whether studies should be retained before drawing conclusions. These methodological considerations prompted us to analyze the conclusions of each study twice (see Flow Chart, Figure 2), before (Step 1) and after (Step 2) excluding those which were not sufficiently satisfactory for each domain studied. Figure 3 states high methodological biases per domain for each study by a means of a warning symbol. Figure 4 and Figure 5 show results for each domain using pie charts for both Step 1 and Step 2 analyses.
A great heterogeneity is observed in terms of sample characteristics, assessment tools and medication status. Inclusion and exclusion criteria for the ADHD groups varied across studies. Some authors only excluded potential comorbid reading problems (e.g., Adi-Japha et al., 2007) whereas others were much more restrictive and excluded intellectual disabilities, methylphenidate medication, learning disability, mathematical or reading disorders, neurological, sensory, motor, psychiatric or mood disorders (e.g., Borella et al., 2011). ADHD presentation was either specified (e.g., Hung & Chang, 2022; Shen et al., 2012) or not stated (e.g., Laniel et al., 2020; Okuda et al., 2011). Some authors mentioned whether methylphenidate was taken (e.g., Frings et al., 2010) while others did not (e.g., Farhangnia et al., 2020; Lofty et al., 2011) and in one study (Lange & Tucha, 2001), the handwriting skills of ADHD children were tested twice, with and without methylphenidate. It is important to observe a wide diversity of assessment tools and conditions: paper-and-pen material (e.g., Capodieci et al., 2019), digitizing tablet (e.g., Langmaid et al., 2014) and even questionnaires for parents (Åsberg Johnels et al., 2014) were proposed to assess handwriting characteristics. With respect to writing conditions, spontaneous letter production (Langmaid et al., 2016), copy tasks (e.g., Rosenblum et al., 2008) or dictation tasks (e.g., Capodieci et al., 2019) were suggested.
3.1. Roduct of Handwriting Results
3.1.1. Quality/Legibility
Seventeen out of 21 studies examined quality/legibility (Adi-Japha et al., 2007; Åsberg Johnels et al., 2014; Borella et al., 2011; Capodieci et al., 2018; Capodieci et al., 2019; Dirlokov et al., 2017; Farhangnia et al., 2020; Flapper et al., 2006; Frings et al., 2010; Hung & Chang, 2022; Johnson et al., 2013; Laniel et al., 2020; Lofty et al., 2011; Okuda et al., 2011; Rosenblum et al., 2008; Shen et al., 2012; Tucha & Lange, 2001; Yoshimasu et al., 2011). The findings of 6 studies cannot be considered for Step 2 as a result of major methodological biases: the study by Farhangnia et al. (2020) for absence of inclusion/exclusion criteria; the study conducted by Flapper et al. (2006) due to associated DCD for all ADHD children, making it impossible to determine whether handwriting difficulties resulted from ADHD per se or DCD; the study by Frings et al. (2010) owing to absence of clear exclusion criteria; studies by Laniel et al., (2020), Okuda et al. (2011) and Rosenblum et al. (2008) on account of insufficiently detailed inclusion/exclusion criteria and reduced samples size (n < 15), thereby implying the presence of potential critical confounding factors and methodological weakness. Tucha & Lange (2001) pointed out two results: ADHD children showed a significantly poorer quality of handwriting without treatment than control boys but presented no difference with methylphenidate. All studies (100%) reported differences between ADHD children and the control groups either before (17/17 studies) or after (11/11) exclusion.
3.1.2. Primary Conclusions with Respect to Quality/Legibility of Handwriting
Beyond the observed methodological heterogeneity and after exclusion of works presenting important biases, it is reasonable to assume that handwriting quality is indeed impaired in ADHD. Nevertheless, very few studies have reported effect sizes, making it impossible to precisely quantify the significance of these difficulties. Finally, it is not possible to tell whether all ADHD children manifested impairment in quality/legibility of handwriting due to an absence of individualized data uncovering potential inter-individual variability in writing performance.
3.1.3. Speed of Handwriting
Twelve included studies out of 21 focused on speed of handwriting (Adi-Japha et al., 2007; Borella et al., 2011; Capodieci et al., 2018; Capodieci et al., 2018; Capodieci et al., 2019; Dirlokov et al., 2017; Farhangnia et al., 2020; Flapper et al., 2006; Hung & Chang, 2022; Johnson et al., 2013; Laniel et al., 2020; Rosenblum et al., 2008; Shen et al., 2012; Yoshimasu et al., 2011). After analyzing the findings independently of methodological quality, 8 out of 12 studies (66.7%) reported no difference between ADHD children and control groups versus 33.3% in favor of a variation in writing speed. The latter proportion dropped to 25% on Step 2 after studies with major methodological biases were excluded (i.e., Farhangnia et al., 2020; Flapper et al., 2006; Laniel et al., 2020; Rosenblum et al., 2008). The only work showing a significant difference with a slower writing speed in well-identified non-medicated ADHD children arose from the study by Borella et al. (2011). In research conducted by Hung & Chang (2022), it was unclear whether or not ADHD children were on medication which hindered our ability to draw a clear conclusion.
3.1.4. Primary Conclusions with Respect to Speed of Handwriting
After excluding studies with major biases, the trend therefore pointed towards an absence of difference in handwriting speed between unmedicated children with ADHD and typically developing subjects. As observed earlier, we cannot state whether all children with ADHD manifested problems in the speed domain due to an absence of individual data in the included studies. The overall results considering product (i.e., quality/legibility) and speed of handwriting before and after exclusion of studies with major methodological biases are displayed in Figure 4.
3.2. Process of Handwriting
Fourteen studies out of 21 examined the handwriting process (Adi-Japha et al., 2007; Borella et al., 2011; Capodieci et al., 2018; Capodieci et al., 2019; Dirlokov et al., 2017; Hung & Chang, 2022; Johnson et al., 2013; Langmaid et al., 2014; Langmaid et al., 2016; Laniel et al., 2020; Rosenblum et al., 2008; Shen et al., 2012; Tucha & Lange, 2001; Tucha & Lange, 2004). There were various targeted variables: working memory load, strokes duration, ballisticity, in-air time or pen pressure. Only one study (Johnson et al., 2013) reported absence of difference (considering the coefficient of variability in phrase height and width). Tucha & Lange (2001) found that methylphenidate use led to handwriting process deterioration but following withdrawal, the results of ADHD children did not differ from control groups. Before exclusion (Step 1), 13 out of 14 studies (92.9%) indicated variations between ADHD children and control groups. This score remained at 91.7% at Step 2 after exclusion of studies by Laniel et al. (2020) and Rosenblum et al. (2008) for the same reasons as those mentioned previously (Figure 3). Authors highlighted that ADHD children demonstrated increased pen pressure (Adi-Japha et al., 2007), greater variability in acceleration-deceleration phases (Borella et al., 2011) and in stroke length (Langmaid et al., 2014) or more inversions in the direction of their velocity profiles, thereby indicating a lack of automation (Tucha & Lange, 2004) when compared to the control groups.
3.2.1. Primary Conclusions Regarding Process of Handwriting
Evidence clearly favors impaired handwriting process in children with ADHD. When available, the effect sizes indicated a significant impact of ADHD on handwriting process, thereby highlighting important disturbances beyond product per se (e.g., Capodieci et al., 2018; Capodieci et al., 2019; Hung & Chang, 2022; Shen et al., 2012). In regard to evaluation of handwriting product performance, the studies did not provide individual data that would have enabled us to confirm any inter-individual variability in the handwriting process. The results considering handwriting process before and after exclusion of studies with major methodological biases are displayed in Figure 5.
4. Discussion
The two main objectives of this systematic review were to: (i) describe whether the evidence for a deficit in writing product and process is compelling enough to conclude that children with ADHD manifest dysgraphia and; (ii) determine whether all children with ADHD are affected.
4.1. Is Handwriting Performance in Children with ADHD Really Impaired?
This systematic review shows that 100% (17/17 for Step 1, 11/11 for Step 2) of studies comparing ADHD and typically developing children reported altered quality of written trace in ADHD individuals; 33.3% (4/12 for Step 1) and 25% (2/8 of studies for Step 2) revealed altered speed of production while 92.9% (13/14 for Step 1) and 91.7% (11/12 for Step 2) of studies described impaired handwriting process.
ADHD children therefore clearly seem to experience problems both in the product and process of handwriting. These results are in line with recent works in typically developing school-aged children, showing that handwriting quality and speed significantly correlate with various process characteristics (e.g., the number of strokes, reaction time, duration, on-paper duration, pen pressure, vertical and horizontal sizes, absolute velocity, etc.). In the study by Coradinho et al. (2023), poorer handwriting quality was notably associated with a higher average absolute pen velocity, larger vertical or horizontal sizes and lower relative on-paper duration. This suggests that kinematic abnormalities could at least partly account for difficulties in terms of quality and/or speed of handwriting. If we consider writing performance along a continuum as outlined above, such associations between handwriting quality and kinematic variables may be even more pronounced in ADHD children. In our review, the finding that around 100% of studies detected abnormalities in the handwriting product and process of children with ADHD compared to control groups also implies close links between the two spheres. It is important to note that effect sizes indicated a considerable impact on process due to ADHD (e.g., Capodieci et al., 2018; Capodieci et al., 2019; Hung & Chang, 2022; Shen et al., 2012). Likewise, all these observations do not really stand up to scrutiny when considering writing speed. Indeed, only 25% of studies with valid methodology (Step 2) reported a difference in handwriting speed between ADHD and typically developing children. This calls for caution and further studies with better methodological quality when clarifying the characteristics of ADHD subjects in the domain of handwriting speed.
Our results overall should be considered with great caution. Firstly, very few studies reported effect sizes when considering product. It is therefore extremely difficult – if not impossible – to determine whether the differences observed between ADHD children and control groups are important or not. Moreover, handwriting problems associated with ADHD might be due to a comorbid DCD where handwriting difficulties are well-identified (Lopez et al., 2018; O’Hare & Khalid, 2022; Vaivre-Douret et al., 2011; Bieber et al., 2016; Biotteau et al., 2019). More generally, comorbidities have not been screened rigorously in studies although their impact on the handwriting skills of ADHD children may be crucial. In addition, since most studies did not use standardized tools, it is also complicated to know whether ADHD children display mild difficulties or severe dysgraphia. The approach of identifying handwriting difficulties along a continuum ranging from mild to severe dysgraphia is gaining support. From this perspective, recent studies argue against a dichotomic classification of children as non-dysgraphic on the one hand and dysgraphic on the other (e.g., Lopez et al., 2018). Additional works will have to detect where each ADHD child is situated along on this continuum. Finally, although there is no gold standard for diagnosing dysgraphia, it has to be noted that a number of qualitative tests have been developed (Rosenblum et al. 2003) which assess both product and process with available norms and acceptable reliability (Feder & Majnemer, 2003). Our review shows that some more subjective or esoteric evaluations were rather used, hindering comparability of the results.
An intriguing question, even if it is out of the scope of our review, lies in the putative beneficial effects of methylphenidate on the handwriting skills of children with ADHD. At best, medication seems effective for a portion of children (e.g., Brossard-Racine et al., 2015) while at worst, there is no impact at all (e.g., Rothe et al., 2023). Again, such equivocal results highlight inter-individual variability regarding mechanisms which underpin handwriting disorders. In some people with attentional and executive deficits, which are very common in ADHD, handwriting disorders could be the direct consequence of impoverish cognitive control. In this case, methylphenidate could largely contribute to improving handwriting skills although fluency seems to deteriorate in parallel (see Tucha & Lange, 2001). Overall, such contradictory findings suggest that there is a need to identify ADHD children who take (or do not take) methylphenidate in studies investigating handwriting skills, given the possible beneficial effect for a number of subjects. From a clinical point of view, it is also very important to realize that methylphenidate will not automatically improve handwriting quality and may even contribute to slowing down speed of production. This warrants an individualized approach for each child when considering all the parameters involved in handwriting, notably cognitive functioning, degree of severity of handwriting difficulties, methylphenidate consumption or non-consumption, alteration in product and/or process, etc.
In summary and in response to the question "Is handwriting performance in children with ADHD really impaired?", we can therefore answer that yes in light of this review, there do seem to be difficulties linked to written trace in ADHD children, especially for quality/legibility. However, almost nothing is known about the degree of severity of these difficulties. Moreover, there is an evident paucity of data regarding the proportion of children with ADHD experiencing impairment in written trace production. Finally, the tendency is to admit that there is no obvious difference in handwriting speed between ADHD and typically developing children but further studies are essential in this area to refine the results.
4.2. Are All Children with ADHD Affected by Handwriting Deficits?
From our review, it is evident that children with ADHD encounter more handwriting problems than non-ADHD children. However, we cannot know the proportion of ADHD children affected by handwriting difficulties since almost all the studies failed to consider potential inter-individual differences. The exception was the study by Lofty et al. (2011) which reported that 50% of ADHD children in their sample experienced mild to moderate difficulties. We are faced with a major issue here since a plethora of studies showed that significant inter-individual variability of outcomes and performance in diverse tasks and contexts is a hallmark of ADHD (Kuntsi & Klein, 2012). It is therefore highly probable that all children with ADHD do not present the same level of written performance although this remains to be demonstrated beyond the study conducted by Lofty et al. (2011). This lack of data is particularly regrettable given that in other neurodevelopmental conditions, the picture is clearer and helps with an overall understanding of the children’s difficulties. In the case of DCD, for example, up to 87–88% of children have handwriting disorders with around 15% experiencing a severe deficit (e.g., Lopez et al., 2018; O’Hare & Khalid, 2022; Vaivre-Douret et al., 2011). Generating the same type of evidence on handwriting skills in ADHD is therefore fundamental to support medical care decision-making and the support required at school. Yet, these difficulties in identifying the prevalence of ADHD children affected by mild handwriting difficulties or severe dysgraphia fall within a more general framework. In truth, it is obvious that the lack of a clear and consensual definition of dysgraphia hinders calculation of a reliable worldwide prevalence. Estimates range from 10 to 30% of school-age children with dysgraphia (Karlsdottir & Stefansson, 2002; Maeland, 1992; Naider-Steinhart & Katz-Leurer, 2007) depending on the definitions used. The disorder is marked by a dearth of precise criteria sets for diagnosis and according to DSM 5, dysgraphia can be diagnosed as “impairment in written expression” (APA, 2015) which is a very broad definition, leaving plenty of scope for subjective views. In studies on writing impairments, different definitions of dysgraphia are therefore used but only 5% of children would be concerned when limiting to strict handwriting difficulties (Katusic et al., 2009). A recent study even found that only 41% of children affected by handwriting difficulties are impaired enough to use the term dysgraphia (Lopez & Vaivre-Douret, 2023), thereby drastically reducing the prevalence of the disorder. It seems duly urgent to clarify the criteria characterizing handwriting difficulties that can culminate in dysgraphia if severe and persistent enough.
In response to the question "Are all children with ADHD affected by dysgraphia?", we can therefore answer that the estimated proportion is still unknown given the evident paucity of data which came to light through our review.
4.3. Suggested Recommendations for the Conduct of Studies on ADHD and Comorbid Handwriting Disorders
The broad range of handwriting impairments across all included studies could reflect discrepancies in letter forms combined with various handwriting educational backgrounds systems in different countries (Gannetion et al., 2022) but is likely to mirror variations between the experimental methods used. There are indeed a number of studies where methodological approaches were deemed to introduce possible biases in the results. Overall, a key finding of our review was that standardized procedures for the conduct of studies in this field are needed. To our knowledge, there are no known guidelines for carrying out studies in dysgraphia comorbidity in general or in strict co-occurrence with ADHD. On the basis of observations arising from our review completed by the Clinical Practice Guideline for the Diagnosis, Evaluation and Treatment of ADHD (Wolraich et al. 2019), we have therefore provided some recommendations for future studies in this domain.
4.3.1. Dysgraphia Evaluation
While ADHD diagnosis criteria were sufficient overall in almost all studies, parameters for dysgraphia case inclusion were not clear. Firstly, according to studies, “dysgraphia” terminology may be used to encompass several disorders ranging from strict handwriting to spelling or reading. Secondly, the profile of children included greatly varied depending on selection criteria and assessment instruments while severity of ADHD was not considered. Thirdly, in a number of included studies, handwriting performance was evaluated using informal qualitative observations by parents and/or teachers. There are as yet a variety of objective measures (formal quantitative standardized tests) to judge children’s handwriting performance at different ages, which measure both legibility and speed of handwriting with acceptable reliability (Feder & Majnemer, 2003). Although observations from both parents and teachers are helpful, self-rated questionnaires can be insufficient (sometimes asking parents to answer only one general question), imprecise (most parents do not possess adequate knowledge for comparison purposes) and above all too subjective. We recommend the use of standardized, valid and reliable tools that provide a quantitative score to determine if children are affected by a handwriting disorder outside the normal range and the severity of impairment.
The issue of those in charge of measuring children’s performance also requires consideration. Even when excluding teachers or parents for the abovementioned reasons, only one evaluator, sometimes with unreported areas of competence, was probably found to assess handwriting skills. This measurement bias could be prevented two-fold by using the expertise of a handwriting specialist and employing a double-blinded method. Accordingly, the examiner should not be informed about whether or not the children have comorbid ADHD and handwriting disorders. Given the subjective nature of some criteria, the use of two independent judges also seems requisite, ideally providing additional intra-class correlations for ensuring homogeneity in the scoring procedure. It should also be noted that coupled product and process analysis is possible when writing is recorded on digitizing tablets. Several kinematic variables can then be computed (e.g., pen grip and finger pressure on the pen, in-air and on-paper durations, velocity, etc.) more objectively (Danna, Paz-Villagrán & Velay, 2013; Paz-Villagrán, Danna & Velay, 2014). We recommend a minimum of two independent blinded trained judges, with expertise in handwriting assessment, to assess handwriting process and product in a less subjective manner. The use of digitizing graphic tablets should be favored. New tools such as deep learning procedure for detecting dysgraphia are also under development (Gemelli et al., 2023) and should improve the scoring procedure in years to come.
Finally, experimental tasks proposed to children varied hugely: writing a continuous repetitive alternated sequence of cursive letters, numbers, words, sentences or text; writing on lined paper-sheets, on blank pages or digitizing tablets; in production/composition, dictation, copying (near-point or far-point copying) tasks, under working memory or cognitive load, etc. This broad variability compromises the comparability of findings. It is of crucial importance to harmonize measurement of key handwriting elements and use common outcome measures to facilitate pooling and comparison between study findings. In addition, experimental methodologies could sometimes fail to represent real school life experience. Studies need a non-artificial evaluation which captures a child’s performance in everyday life settings (i.e., in the most environmentally-friendly conditions possible). We recommend that experimental tasks be as similar as possible from one study to another and that they represent the child’s experiences at school or at home as closely as possible in order to highlight his or her real writing difficulties. The use of longitudinal studies could also provide valuable information as they enable the collection of very detailed information without intervention. Handwriting data could be gathered as part of routine care procedures in standard medical practice rather than experimental frameworks. It seems primordial of course (to ensure the comparability of results) to use matched comparison groups which requires, for these type of comorbid studies (ADHD + handwriting deficit), a control group with typically developing children, another containing ADHD children only and a last group comprising children affected only by handwriting disorders.
4.3.2. Confounding Factors
One of the most striking results of our review was that few studies observed the same handwriting impairments. While the administration of different tasks contributes to this heterogeneity, it does not account for the whole picture. An explanation may also lie in the heterogeneity of samples. In reality, the vast majority of studies failed to explore ADHD subtypes or comorbidities. ADHD often co-occurs with other neurodevelopmental disorders, psychiatric disorders (depression, anxiety disorders) or sleep disturbance (Faraone et al., 2019). If their presence does not rule out a diagnosis of ADHD, such comorbidities could have a real impact on handwriting skills and therefore may induce major biases. Handwriting disorders are actually not specific to children with ADHD and may be recognized in other disorders often comorbid with ADHD such as depression (Mergl et al., 2004), sleep deprivation (Asper et al., 2009) or in DCD (Cousin et al., 2003) among others. The clinical presentation of ADHD (inattentive, hyperactive-impulsive or combined) may also play a role. In fact, patterns of associated disorders differ between ADHD subtypes, ADHD inattentive being more strongly associated with academic impairment and manual dexterity deficits while hyperactive-impulsive symptoms are mainly linked to eagerness and rushing (Willcutt et al., 2012). Handwriting abnormalities are also linked to the severity of ADHD and the more problematic the symptoms, the poorer the handwriting performance (Doyle et al. 1995). However, this factor was not sufficiently accounted for in the studies included. Choice of age ranges as well as gender distribution were also insufficiently reasoned between various studies while handwriting ability acquisition is a long process (Palmis et al., 2017). In addition, gender is known to have an impact at least on handwriting product (legibility) in typically developing children (Feder et al. 2007). Socioeconomic factors can also alter handwriting skills (O’Mahony et al. 2008) as well as ethnicity and cultural background (Gannetion et al., 2022). Therefore, we recommend that individual and demographic factors associated with ADHD or handwriting skills are properly identified and considered in order to minimize possible biases: all possible comorbidities (neurodevelopmental, psychiatric), ADHD presentation, age, gender as well as ethnicity, cultural background, socioeconomic status or familial handwriting habits. Even if handedness has not been identified as a predictor of handwriting quality (Vlachos et al., 2004) or writing speed (O’Mahony et al., 2008), its impact on the handwriting process has been sufficiently studied and this factor should take precedence in future studies.
4.3.3. Medication and Behavioral Treatments
Among ADHD children, a substantial number take medication (methylphenidate continues to be the first-line medication) and/or benefit from behavioral treatment (diversely home-based and school-based behavioral treatments, psychosocial treatment, training interventions, psychoeducation, learning and academic support, parental practices, school accommodation, intervention for management of associated symptoms, etc.). Most worldwide medical organizations suggest beginning with psychoeducation and behavioral management, and thereafter the use (additionally or not) of psychostimulant medications (Thapar et al., 2016). Only US guidelines recommend medication as initial treatment and consequently 60 to 70% of school-aged American ADHD children are taking medication (Danielson et al., 2018). If more data are needed to judge the efficacy of all existing non-medication treatments, a large number of meta-analysis studies found medications to be highly effective in reducing the ADHD symptoms or associated impairments (Faraone et al., 2019). The influence of medication on motor skills (dynamic balance and fine motor skills) is particularly well demonstrated (Kaiser et al., 2015). However, results are more divergent concerning handwriting according to the authors. As a result of our review, we share the opinion that more evidence is needed to affirm that medication has a positive influence on handwriting. Too few studies have considered medication in their analysis and conclusions while none have appraised the possible confounding effects of behavior management on handwriting. Consequently, contemplation of all treatments, past or actual for both ADHD and/or comorbid symptoms, is strongly recommended to observe whether treated children with ADHD possess different handwriting features than their matched peers without treatment. Most significantly, the interaction between handwriting skills and medication should be addressed with great attentiveness given their effects are well-demonstrated on symptoms that beyond the strict framework of ADHD. Once again, the use of real-life longitudinal studies would be a major asset as they would make it possible to compare groups of treated subjects with untreated subjects or make pre-post treatment observations in order to highlight the correlation between the treatment under consideration and the evolution of the handwriting disorder. We recommend that future studies scrupulously identify and consider all past or present medication and non-medication treatment.
A summary of the aforementioned recommendations for future studies in this field is proposed based on the findings of this systematic review in Table 5.
4.4. Theoretical considerations
We close this section with the following aspects that seem important. It would be relevant to support clinical findings with more fundamental work dealing with theoretical models of handwriting, whether it be neural network models (Gangadhar et al., 2007), equilibrium point models (Feldman & Latash, 2005), behavioral models (Schmidt, 1999; van Galen & Teulings, 1983), coupled oscillator models (Kelso, 1995; Zazone et al., 2005), kinematic models (Plamondon & Djioua, 2006), or models exploiting minimization principles (Wada & Kawato, 1995; Engelbrecht, 2001). Such an approach would make it possible to enrich or revise certain models on the basis of clinical data, and verify their applicability in the more specific context of ADHD. In turn, this would provide clinicians with information on the relevance of targeting a particular variable, or making predictions about the probability of success of a given therapeutic approach based on theoretical considerations
5. Conclusions
Although handwriting abnormalities in children with ADHD is frequently cited, a systematic review aimed at identifying and collating strong findings of impaired handwriting process and/or product in this population has been not available to date. Of the 21 articles retrieved, 17 described the quality/legibility in the handwriting of children with ADHD, 12 focused on speed and 14 articles analyzed the process of handwriting. Results reveal that 100% of the studies reported impaired quality of written trace and the handwriting process in ADHD individuals while 25% reported altered speed of production. Legibility of the produced trace was also found to be the most common type of impairment whereas speed of production seemed to be relatively preserved. Prevalence of handwriting disorders in ADHD was not possible to determine on the basis of the studies included. The most general conclusion from our review is that considerable gaps exist in our knowledge of handwriting skills in children with ADHD. Great caution must be exercised when drawing conclusions and more research is needed before making clear statements on whether dysgraphia is actually associated with all children with ADHD. We identified a number of challenges while conducting studies in this field. Most significantly, a wide diversity existed between the experimental conditions or dysgraphia criteria diagnosis or when verifying other comorbid conditions, ADHD subtypes and medical status (treated or non-treated) of included children. This evidently calls for standards while conducting studies on the prevalence of dysgraphia in ADHD to ensure case ascertainment, exact co-occurrence rate and comparison between countries and over time. A summary of recommendations to conduct future studies has been proposed which might produce reduced heterogeneity and better-quality studies on this issue. It has to be noted that, for enabling comparisons between studies, our review was limited to studies exploring handwriting performance when comparing ADHD samples to typically developing children (control groups). In reality, this approach may have excluded some studies investigating the impact of ADHD treatment on dysgraphia and this important issue also absolutely needs to be addressed.
Supplementary Materials
Figure 1. Illustration of Handwriting Process and Product; Figure 2. Flow Chart of Included and Excluded Studies; Figure 3. Rapid Overview of Results of Included Studies.; Figure 4. Pie Charts for Both Step 1 and Step 2 Analyses for Product of Handwriting.; Figure 5. Pie Charts for Both Step 1 and Step 2 Analyses for Process of Handwriting; Table 1: Critical Appraisal Skills Program (CASP); Table 2. Methodological Quality of Included Studies Scored with the CASP List for Systematic Review; Table 3. Characteristics and Results of Included Studies; Table 4. Recommendations for Future Research.
Author Contributions
FP and MB are the Principal Investigators of the review. They conceived the topic and were major contributors in writing the protocol. FP carried out the methodology and wrote the methodology section of the manuscript. FP and MB analyzed and interpreted the data, conceived the first working plan based on results and wrote the manuscript. YC reviewed the final manuscript and proposed some improvements. All the Authors read and approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the Corresponding Author upon reasonable request.
Acknowledgments
We would like to thank the Special Issue Guest Editors Carlone Jolly and Jérémy Danna for their trust and support. The Authors also thank Elan Languages for his careful checking of the English language, and Maxime Masgrau for his beautiful graphic work.
Conflicts of Interest
The Authors declare no conflict of interest.
References
- Adi-Japha, E., Landau, Y. E., Frenkel, L., Teicher, M., Gross-Tsur, V., & Shalev, R. S. (2007). ADHD and dysgraphia: underlying mechanisms. Cortex, 43(6), 700-709. [CrossRef]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author. [CrossRef]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author. [CrossRef]
- Åsberg Johnels, J., Kopp, S., & Gillberg, C. (2014). Spelling difficulties in school-aged girls with attention-deficit/hyperactivity disorder: behavioral, psycholinguistic, cognitive, and graphomotor correlates. Journal of Learning Disabilities, 47(5), 424-434. [CrossRef]
- Asselborn, T., Chapatte, M., & Dillenbourg, P. (2020). Extending the spectrum of dysgraphia: A data driven strategy to estimate handwriting quality. Scientific Reports, 10:3140. [CrossRef]
- Bartoň, M., Fňašková, M., Rektorová, I., Mikl, M., Mareček, R., Rapcsak, S. Z., & Rektor, I. (2020). The role of the striatum in visuomotor integration during handwriting: an fMRI study. Journal of Neural Transmission, 127, 331-337. [CrossRef]
- Berninger, V. W., Richards, T. L., & Abbott, R. D. (2015). Differential diagnosis of dysgraphia, dyslexia, and OWL LD: Behavioral and neuroimaging evidence. Reading and Writing, 28, 1119-1153. [CrossRef]
- Bieber, E., Smits-Engelsman, B. C., Sgandurra, G., Cioni, G., Feys, H., Guzzetta, A., & Klingels, K. (2016). Manual function outcome measures in children with developmental coordination disorder (DCD): Systematic review. Research in Developmental Disabilities, 55, 114-131. [CrossRef]
- Biotteau, M., Danna, J., Baudou, É., Puyjarinet, F., Velay, J. L., Albaret, J. M., & Chaix, Y. (2019). Developmental coordination disorder and dysgraphia: signs and symptoms, diagnosis, and rehabilitation. Neuropsychiatric Disease and Treatment, 1873-1885. [CrossRef]
- Borella, E., Chicherio, C., Re, A. M., Sensini, V., & Cornoldi, C. (2011). Increased intraindividual variability is a marker of ADHD but also of dyslexia: A study on handwriting. Brain and Cognition, 77(1), 33–39. [CrossRef]
- Breda, V., Rohde, L. A., Menezes, A. M. B., Anselmi, L., Caye, A., Rovaris, D. L., et al. (2020). Revisiting ADHD age-of-onset in adults: to what extent should we rely on the recall of childhood symptoms?. Psychological Medicine, 50(5), 857-866. [CrossRef]
- Brossard-Racine, M., Majnemer, A., Shevell, M., & Snider, L. (2008). Handwriting performance in children with attention deficit hyperactivity disorder (ADHD). Journal of Child Neurology, 23(4), 399-406. [CrossRef]
- Brossard-Racine, M., Majnemer, A., Shevell, M., Snider, L., & Bélanger, S. A. (2011). Handwriting capacity in children newly diagnosed with attention deficit hyperactivity disorder. Research in Developmental Disabilities, 32(6), 2927-2934. [CrossRef]
- Brossard-Racine, M., Shevell, M., Snider, L., Bélanger, S. A., & Majnemer, A. (2012). Motor skills of children newly diagnosed with Attention Deficit Hyperactivity Disorder prior to and following treatment with stimulant medication. Research in Developmental Disabilities, 33(6), 2080-2087. [CrossRef]
- Brossard-Racine, M., Shevell, M., Snider, L., Belanger, S. A., Julien, M., & Majnemer, A. (2015). Persistent handwriting difficulties in children with ADHD after treatment with stimulant medication. Journal of Attention Disorders, 19(7), 620-629. [CrossRef]
- Capodieci, A., Lachina, S., & Cornoldi, C. (2018). Handwriting difficulties in children with attention deficit hyperactivity disorder (ADHD). Research in Developmental Disabilities, 74, 41-49. [CrossRef]
- Capodieci, A., Serafini, A., Dessuki, A., & Cornoldi, C. (2019). Writing abilities and the role of working memory in children with symptoms of attention deficit and hyperactivity disorder. Child Neuropsychology, 25(1), 103-121. [CrossRef]
- CASP, 2010. Critical Appraisal Skills Programme – Making Sense of Evidence About Clinical Effectiveness – Case-control Studies. CASP, From https://casp-uk.net/images/checklist/documents/archive/CASP-Randomised-Controlled-Trial-Checklist-2018_fillable_form.pdf.
- Coradinho, H., Melo, F., Almeida, G., Veiga, G., Marmeleira, J., Teulings, H. L., & Matias, A. R. (2023). Relationship between Product and Process Characteristics of Handwriting Skills of Children in the Second Grade of Elementary School. Children, 10(3), 445. [CrossRef]
- Cousins, M., & Smyth, M. M. (2003). Developmental coordination impairments in adulthood. Human Movement Science, 22(4-5), 433-459. [CrossRef]
- Daley, D., & Birchwood, J. (2010). ADHD and academic performance: why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom?. Child: Care, Health and Development, 36(4), 455-464. [CrossRef]
- Danielson, M. L., Visser, S. N., Chronis-Tuscano, A., & DuPaul, G. J. (2018). A national description of treatment among United States children and adolescents with attention-deficit/hyperactivity disorder. The Journal of Pediatrics, 192, 240-246. [CrossRef]
- Danna, J., Paz-Villagrán, V., & Velay, J. L. (2013). Signal-to-Noise velocity peaks difference: A new method for evaluating the handwriting movement fluency in children with dysgraphia. Research in Developmental Dsabilities, 34(12), 4375-4384. [CrossRef]
- Dirlikov, B., Younes, L., Nebel, M. B., Martinelli, M. K., Tiedemann, A. N., Koch, C. A., et al. (2017). Novel automated morphometric and kinematic handwriting assessment: A validity study in children with ASD and ADHD. Journal of Occupational Therapy, Schools, & Early Intervention, 10(2), 185-201. [CrossRef]
- Doyle, S., Wallen, M., & Whitmont, S. (1995). Motor skills in Australian children with attention deficit hyperactivity disorder. Occupational Therapy International, 2(4), 229-240. [CrossRef]
- DuPaul, G. J., Gormley, M. J., & Laracy, S. D. (2013). Comorbidity of LD and ADHD: Implications of DSM-5 for assessment and treatment. Journal of Learning Disabilities, 46(1), 43-51. [CrossRef]
- Engelbrecht, S. E. (2001). Minimum principles in motor control. Journal of Mathematical Psychology, 45(3), 497-542. [CrossRef]
- Faraone, S. V., & Mick, E. (2010). Molecular genetics of attention deficit hyperactivity disorder. Psychiatric Clinics, 33(1), 159-180. [CrossRef]
- Faraone, S. V., Asherson, P., Banaschewski, T., Biederman, J., Buitelaar, J. K., Ramos-Quiroga, J. A. et al. (2015). Attention-deficit/hyperactivity disorder. Nature Reviews Disease Primers, 1(1), 1-23. [CrossRef]
- Faraone, S. V., Banaschewski, T., Coghill, D., Zheng, Y., Biederman, J., Bellgrove, M. A., et al. (2021). The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neuroscience & Biobehavioral Reviews, 128, 789-818. [CrossRef]
- Farhangnia, S., Hassanzadeh, R., & Ghorbani, S. (2020). Handwriting Performance of Children with Attention Deficit Hyperactivity Disorder: The Role of Visual-Motor Integration. International Journal of Pediatrics, 8(11), 12317-12326.
- Fayyad, J., Sampson, N. A., Hwang, I., Adamowski, T., Aguilar-Gaxiola, S., Al-Hamzawi, A., et al. (2017). The descriptive epidemiology of DSM-IV adult ADHD in the world health organization world mental health surveys. ADHD Attention Deficit and Hyperactivity Disorders, 9, 47-65. [CrossRef]
- Feder, K. P., & Majnemer, A. (2003). Children’s handwriting evaluation tools and their psychometric properties. Physical & Occupational Therapy in Pediatrics, 23(3), 65-84.
- Feder, K. P., & Majnemer, A. (2007). Handwriting development, competency, and intervention. Developmental Medicine & Child Neurology, 49(4), 312-317. [CrossRef]
- Feldman, A. G., & Latash, M. L. (2005). Testing hypotheses and the advancement of science: recent attempts to falsify the equilibrium point hypothesis. Experimental Brain Research, 161, 91-103. [CrossRef]
- Flapper, B. C., Houwen, S., & Schoemaker, M. M. (2006). Fine motor skills and effects of methylphenidate in children with attention-deficit–hyperactivity disorder and developmental coordination disorder. Developmental Medicine and Child Neurology, 48(3), 165-169. [CrossRef]
- Frings, M., Gaertner, K., Buderath, P., Christiansen, H., Gerwig, M., Hein-Kropp, C. et al. (2010). Megalographia in children with cerebellar lesions and in children with attention-deficit/hyperactivity disorder. The Cerebellum, 9, 429-432. [CrossRef]
- Gangadhar, G., Joseph, D., & Chakravarthy, V. S. (2007). An oscillatory neuromotor model of handwriting generation. International Journal of Document Analysis and Recognition (ijdar), 10, 69-84. [CrossRef]
- Gannetion, L., Wong, K. Y., Lim, P. Y., Chang, K. H., & Abdullah, A. F. L. (2022). An exploratory study on the handwritten allographic features of multi-ethnic population with different educational backgrounds. PloS one, 17(10), e0268756. [CrossRef]
- Gemelli, A., Marinai, S., Vivoli, E., & Zappaterra, T. (2023, August). Deep-learning for dysgraphia detection in children handwritings. In Proceedings of the ACM Symposium on Document Engineering 2023 (pp. 1-4). [CrossRef]
- Graham, S., Fishman, E.J., Reid, R., & Hebert, M. (2016). Writing Characteristics of Students with Attention Deficit Hyperactive Disorder: A Meta-Analysis. Learning Disabilities Research & Practice, 31(2), 75–89. [CrossRef]
- Guilbert, J., Alamargot, D., & Morin, M. F. (2019). Handwriting on a tablet screen: Role of visual and proprioceptive feedback in the control of movement by children and adults. Human Movement Science, 65, 30-41. [CrossRef]
- Hamstra-Bletz, L., & Blöte, A. W. (1993). A longitudinal study on dysgraphic handwriting in primary school. Journal of Learning Disabilities, 26(10), 689-699. [CrossRef]
- Hung, Y. F., & Chang, C. J. (2022). The performance and predictors of Chinese character writing in children with attention deficit hyperactivity disorder. Research in Developmental Disabilities, 126, 104244. [CrossRef]
- Jasper, I., Häubler, A., Marquardt, C., & Hermsdoerfer, J. (2009). Circadian rhythm in handwriting. Journal of Sleep Research, 18(2), 264-271. [CrossRef]
- Johnson, B. P., Papadopoulos, N., Fielding, J., Tonge, B., Phillips, J. G., & Rinehart, N. J. (2013). A quantitative comparison of handwriting in children with high-functioning autism and attention deficit hyperactivity disorder. Research in Autism Spectrum Disorders, 7(12), 1638-1646. [CrossRef]
- Kaiser, M. L., Schoemaker, M. M., Albaret, J. M., & Geuze, R. H. (2015). What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Research in Developmental Disabilities, 36, 338-357. [CrossRef]
- Karlsdottir, R., & Stefansson, T. (2002). Problems in developing functional handwriting. Perceptual and motor skills, 94(2), 623-662. [CrossRef]
- Katusic, S. K., Colligan, R. C., Weaver, A. L., & Barbaresi, W. J. (2009). The forgotten learning disability: epidemiology of written-language disorder in a population-based birth cohort (1976–1982), Rochester, Minnesota. Pediatrics, 123(5), 1306-1313. [CrossRef]
- Kelso, J. S. (1995). Dynamic patterns: The self-organization of brain and behavior. Cambridge, MA: The MIT Press. [CrossRef]
- Kuntsi, J., & Klein, C. (2012). Intraindividual variability in ADHD and its implications for research of causal links. Behavioral Neuroscience of Attention Deficit Hyperactivity Disorder and its Treatment, 67-91. [CrossRef]
- Langmaid, R. A., Papadopoulos, N., Johnson, B. P., Phillips, J. G., & Rinehart, N. J. (2014). Handwriting in children with ADHD. Journal of Attention Disorders, 18(6), 504-510. [CrossRef]
- Langmaid, R. A., Papadopoulos, N., Johnson, B. P., Phillips, J., & Rinehart, N. J. (2016). Movement scaling in children with ADHD-combined type. Journal of Attention Disorders, 20(2), 131-137. [CrossRef]
- Laniel, P., Faci, N., Plamondon, R., Beauchamp, M. H., & Gauthier, B. (2020). Kinematic analysis of fast pen strokes in children with ADHD. Applied Neuropsychology: Child, 9(2), 125-140. [CrossRef]
- Lelong, M., Zysset, A., Nievergelt, M., Luder, R., Götz, U., Schulze, C., & Wieber, F. (2021). How effective is fine motor training in children with ADHD? A scoping review. BMC pediatrics, 21, 1-21. [CrossRef]
- Lopez, C., & Vaivre-Douret, L. (2023). Exploratory Investigation of Handwriting Disorders in School-Aged Children from First to Fifth Grade. Children, 10(9), 1512. [CrossRef]
- Lopez, C., Hemimou, C., Golse, B., & Vaivre-Douret, L. (2018). Developmental dysgraphia is often associated with minor neurological dysfunction in children with developmental coordination disorder (DCD). Neurophysiologie Clinique, 48(4), 207-217. [CrossRef]
- Lotfy, A. S., Darwish, M. E. S., Ramadan, E. S., & Sidhom, R. M. (2021). The incidence of dysgraphia in Arabic language in children with attention-deficit hyperactivity disorder. Egyptian Journal of Otolaryngology, 37(1), 115. [CrossRef]
- Maeland, A. F. (1992). Handwriting and perceptual-motor skills in clumsy, dysgraphic, and normal children. Perceptual and Motor Skills, 75(3), 1207-1217. [CrossRef]
- Mayes, S. D., Frye, S. S., Breaux, R. P., & Calhoun, S. L. (2018). Diagnostic, demographic, and neurocognitive correlates of dysgraphia in students with ADHD, autism, learning disabilities, and neurotypical development. Journal of Developmental and Physical Disabilities, 30, 489-507. [CrossRef]
- Mergl, R., Juckel, G., Rihl, J., Henkel, V., Karner, M., Tigges, P., … & Hegerl, U. (2004). Kinematical analysis of handwriting movements in depressed patients. Acta Psychiatrica Scandinavica, 109(5), 383-391. [CrossRef]
- Naider-Steinhart, S., & Katz-Leurer, M. (2007). Analysis of proximal and distal muscle activity during handwriting tasks. The American Journal of Occupational Therapy, 61(4), 392-398. [CrossRef]
- O’Hare A, Khalid S (2022). The association of abnormal cerebellar function in children with developmental coordination disorder and reading difficulties. Dyslexia, 8:234-48. [CrossRef]
- Okuda, P. M. M., Pinheiro, F. H., Germano, G. D., Padula, N. A. D. M. R., Lourencetti, M. D., Santos, L. C. A. D., & Capellini, S. A. (2011). Fine motor, sensory and perceptive function of students with attention deficit disorder with hyperactivity. Jornal da Sociedade Brasileira de Fonoaudiologia, 23, 351-357.
- O’Mahony, P., Dempsey, M., & Killeen, H. (2008). Handwriting speed: duration of testing period and relation to socio-economic disadvantage and handedness. Occupational Therapy International, 15(3), 165-177. [CrossRef]
- Palmis, S., Danna, J., Velay, J. L., & Longcamp, M. (2019). Motor control of handwriting in the developing brain: A review. Developmental Dysgraphia, 123-140. [CrossRef]
- Palmis, S., Velay, J. L., Habib, M., Anton, J. L., Nazarian, B., Sein, J., & Longcamp, M. (2021). The handwriting brain in middle childhood. Developmental Science, 24(2), e13046. [CrossRef]
- Paz-Villagrán, V., Danna, J., & Velay, J. L. (2014). Lifts and stops in proficient and dysgraphic handwriting. Human Movement Science, 33, 381-394. [CrossRef]
- Plamondon, R., & Djioua, M. (2006). A multi-level representation paradigm for handwriting stroke generation. Human Movement Science, 25(4-5), 586-607. [CrossRef]
- Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434-442. [CrossRef]
- Rosenblum, S., & Dror, G. (2016). Identifying developmental dysgraphia characteristics utilizing handwriting classification methods. IEEE Transactions on Human-Machine Systems, 47(2), 293-298. [CrossRef]
- Rosenblum, S., Epsztein, L., & Josman, N. (2008). Handwriting performance of children with attention deficit hyperactive disorders: A pilot study. Physical & Occupational Therapy in Pediatrics, 28(3), 219-234. [CrossRef]
- Rosenblum, S., Parush, S., & Weiss, P. L. (2003). Computerized temporal handwriting characteristics of proficient and non-proficient handwriters. The American Journal of Occupational Therapy, 57(2), 129-138. [CrossRef]
- Rothe, J., Kattlun, F. A., Kaufmann, J., Uhlmann, A., Wanderer, S., Bluschke, A. et al. (2023). Effects of methylphenidate and physiotherapeutic treatment on graphomotor movements in children with ADHD. European Child & Adolescent Psychiatry, 1-11. [CrossRef]
- Shen, I. H., Lee, T. Y., & Chen, C. L. (2012). Handwriting performance and underlying factors in children with Attention Deficit Hyperactivity Disorder. Research in Developmental Disabilities, 33(4), 1301-1309. [CrossRef]
- Schmidt, R. A., Lee, T. D., Winstein, C., Wulf, G., & Zelaznik, H. N. (2018). Motor control and learning: A behavioral emphasis.
- Tannock, R. (2013). Rethinking ADHD and LD in DSM-5: Proposed changes in diagnostic criteria. Journal of Learning Disabilities, 46(1), 5-25. [CrossRef]
- Thapar, A., Martin, J., Mick, E., Arias Vásquez, A., Langley, K., Scherer, S. W. et al. (2016). Psychiatric gene discoveries shape evidence on ADHD’s biology. Molecular Psychiatry, 21(9), 1202-1207. [CrossRef]
- Thomas, R., Sanders, S., Doust, J., Beller, E., & Glasziou, P. (2015). Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics, 135(4), e994-e1001. [CrossRef]
- Tistarelli, N., Fagnani, C., Troianiello, M., Stazi, M. A., & Adriani, W. (2020). The nature and nurture of ADHD and its comorbidities: A narrative review on twin studies. Neuroscience & Biobehavioral Reviews, 109, 63-77. [CrossRef]
- Tucha, O., & Lange, K. W. (2001). Effects of methylphenidate on kinematic aspects of handwriting in hyperactive boys. Journal of Abnormal Child Psychology, 29, 351-356. [CrossRef]
- Tucha, O., & Lange, K. W. (2004). Handwriting and attention in children and adults with attention deficit hyperactivity disorder. Motor Control, 8(4), 461-471. [CrossRef]
- Vaivre-Douret, L., Lalanne, C., Ingster-Moati, I., Boddaert, N., Cabrol, D., Dufier, J. L. et al. (2011). Subtypes of developmental coordination disorder: research on their nature and etiology. Developmental Neuropsychology, 36(5), 614-643. [CrossRef]
- Van Galen, G. P., & Teulings, H. L. (1983). The independent monitoring of form and scale factors in handwriting. Acta Psychologica, 54(1-3), 9-22. [CrossRef]
- Vlachos, F., & Bonoti, F. (2004). Handedness and writing performance. Perceptual and Motor Skills, 98(3), 815-824. [CrossRef]
- Vlachos, F., & Bonoti, F. (2004). Handedness and writing performance. Perceptual and Motor Skills, 98(3), 815-824. [CrossRef]
- Wada, Y., & Kawato, M. (1995). A theory for cursive handwriting based on the minimization principle. Biological Cybernetics, 73(1), 3-13. [CrossRef]
- Willcutt, E. G. (2012). The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics, 9(3), 490-499. [CrossRef]
- Wolraich, M. L., Hagan, J. F., Allan, C., Chan, E., Davison, D., Earls, M., et al. (2019). Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 144(4). [CrossRef]
- Yoshimasu, K., Barbaresi, W. J., Colligan, R. C., Killian, J. M., Voigt, R. G., Weaver, A. L., & Katusic, S. K. (2011). Written-language disorder among children with and without ADHD in a population-based birth cohort. Pediatrics, 128(3), e605-e612. [CrossRef]
- Zanone, P-G., Athènes, S., Sallagoity, I. & Albaret, J-M. (2005). Switching among graphic patterns is governed by coordination dynamics of handwriting. Proceedings of the 12th Biennial Conference of the International Graphonomics Society, Salerno, Italy, pp 255-260.
Figure 1.
Handwriting as a complex skill involving activations in the left dorsal premotor cortex, the inferior parietal cortex, the fusiform gyrus, the bilateral inferior frontal gyrus, the right cerebellum, and the primary motor cortex devoted to manual motor output. In the basal ganglia, the striatum mediates visual-motor integration (Bartoň et al., 2020). Children, unlike adults, recruit in addition the prefrontal cortex, notably the anterior cingular cortex to perform writing tasks, which is interpreted as a mark of a lower-level automation between the ages of 8 and 11 (Palmis et al., 2021). Handwriting also involves gestural and kinematic characteristics (i.e., the handwriting process in green in the text) leading to the production of the written trace (i.e., the product of handwriting).
Figure 1.
Handwriting as a complex skill involving activations in the left dorsal premotor cortex, the inferior parietal cortex, the fusiform gyrus, the bilateral inferior frontal gyrus, the right cerebellum, and the primary motor cortex devoted to manual motor output. In the basal ganglia, the striatum mediates visual-motor integration (Bartoň et al., 2020). Children, unlike adults, recruit in addition the prefrontal cortex, notably the anterior cingular cortex to perform writing tasks, which is interpreted as a mark of a lower-level automation between the ages of 8 and 11 (Palmis et al., 2021). Handwriting also involves gestural and kinematic characteristics (i.e., the handwriting process in green in the text) leading to the production of the written trace (i.e., the product of handwriting).
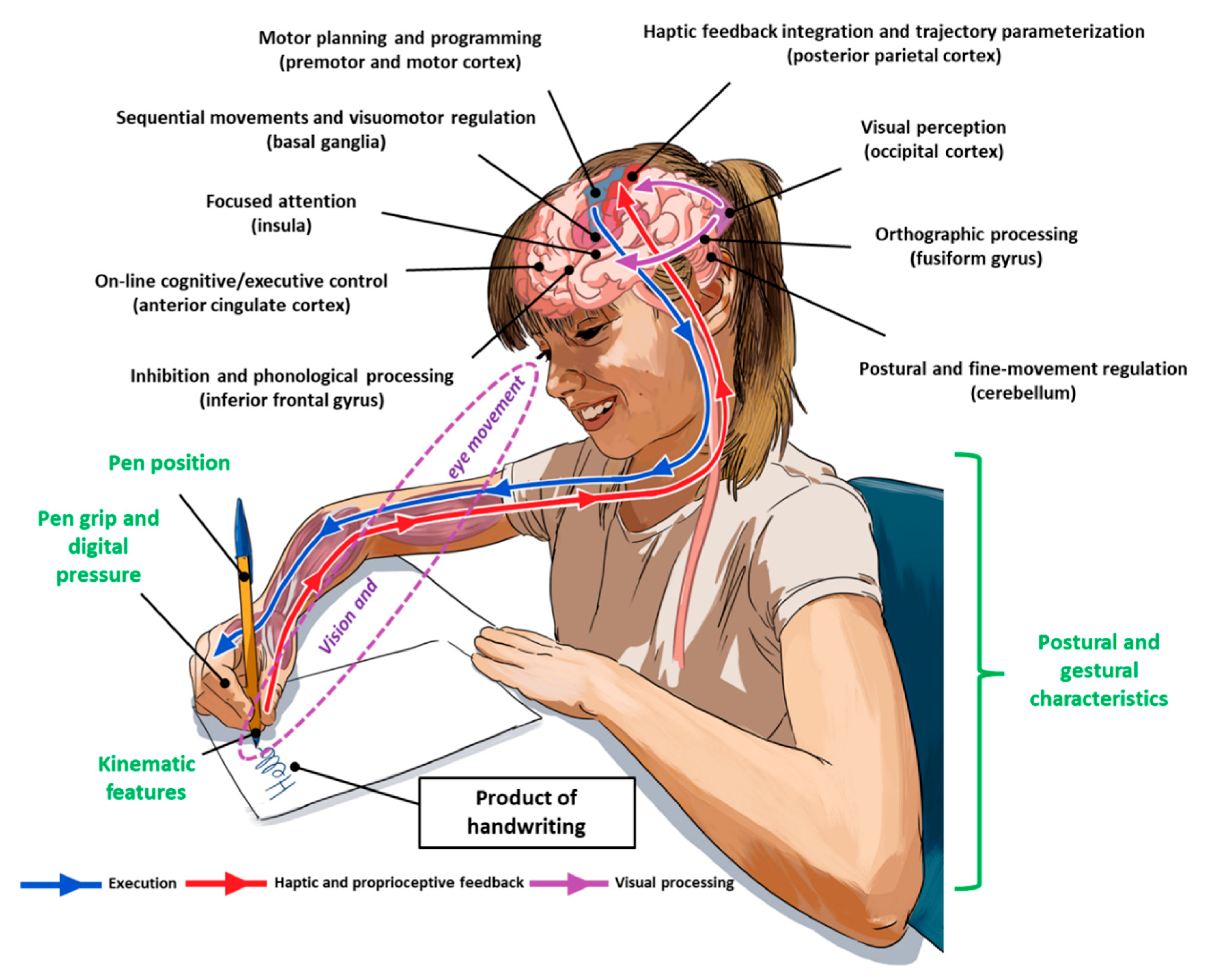
Figure 2.
Flow Chart of Included and Excluded Studies.
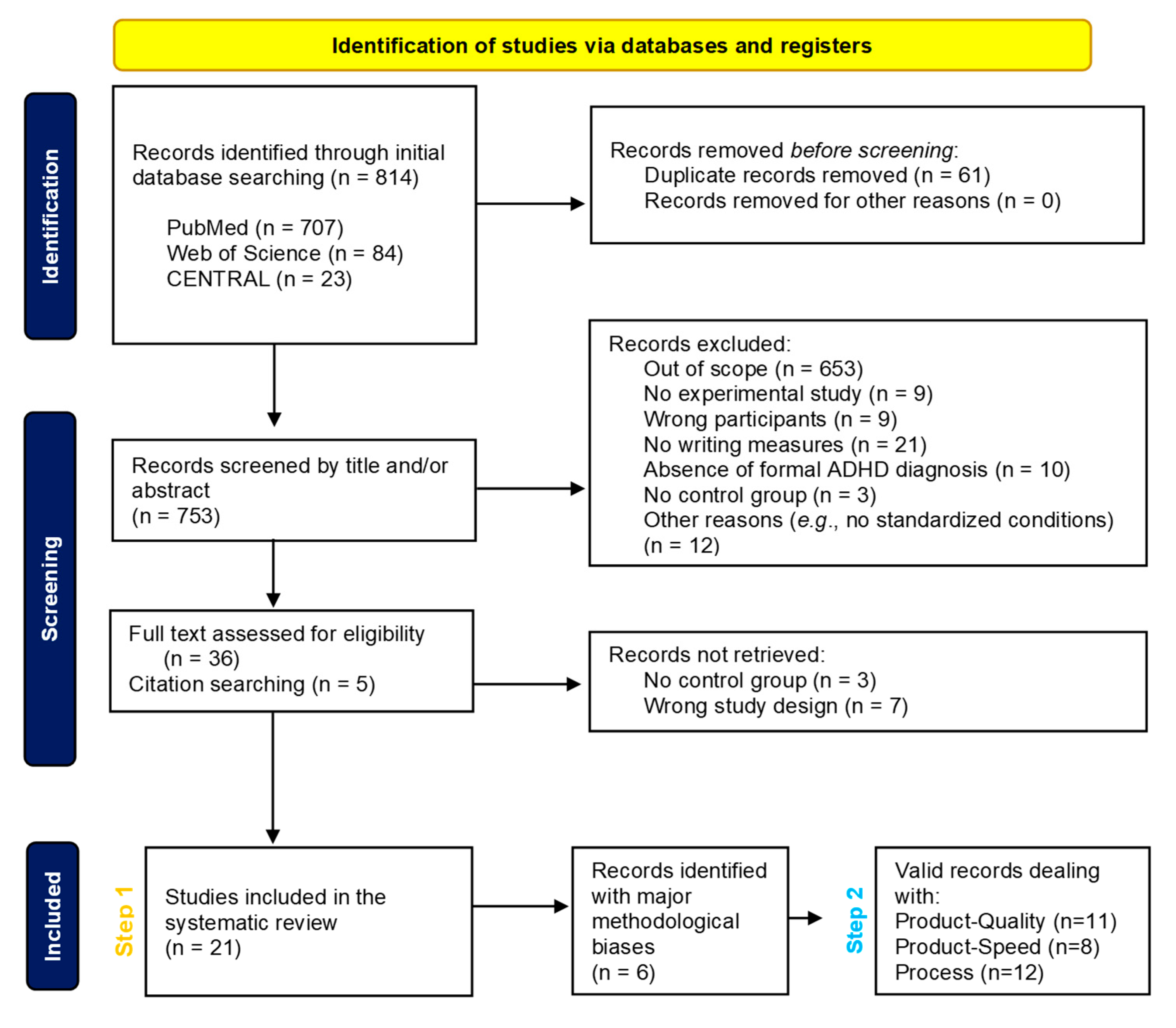
Figure 3.
Rapid Overview of Results of Included Studies. Abbreviations: Q: Quality (Product); S: Speed (Product); P: Process; Green: Non-Impaired; Red: Impaired; ⚠ Methodological Biases Identified; *: Without MPH.
Figure 3.
Rapid Overview of Results of Included Studies. Abbreviations: Q: Quality (Product); S: Speed (Product); P: Process; Green: Non-Impaired; Red: Impaired; ⚠ Methodological Biases Identified; *: Without MPH.
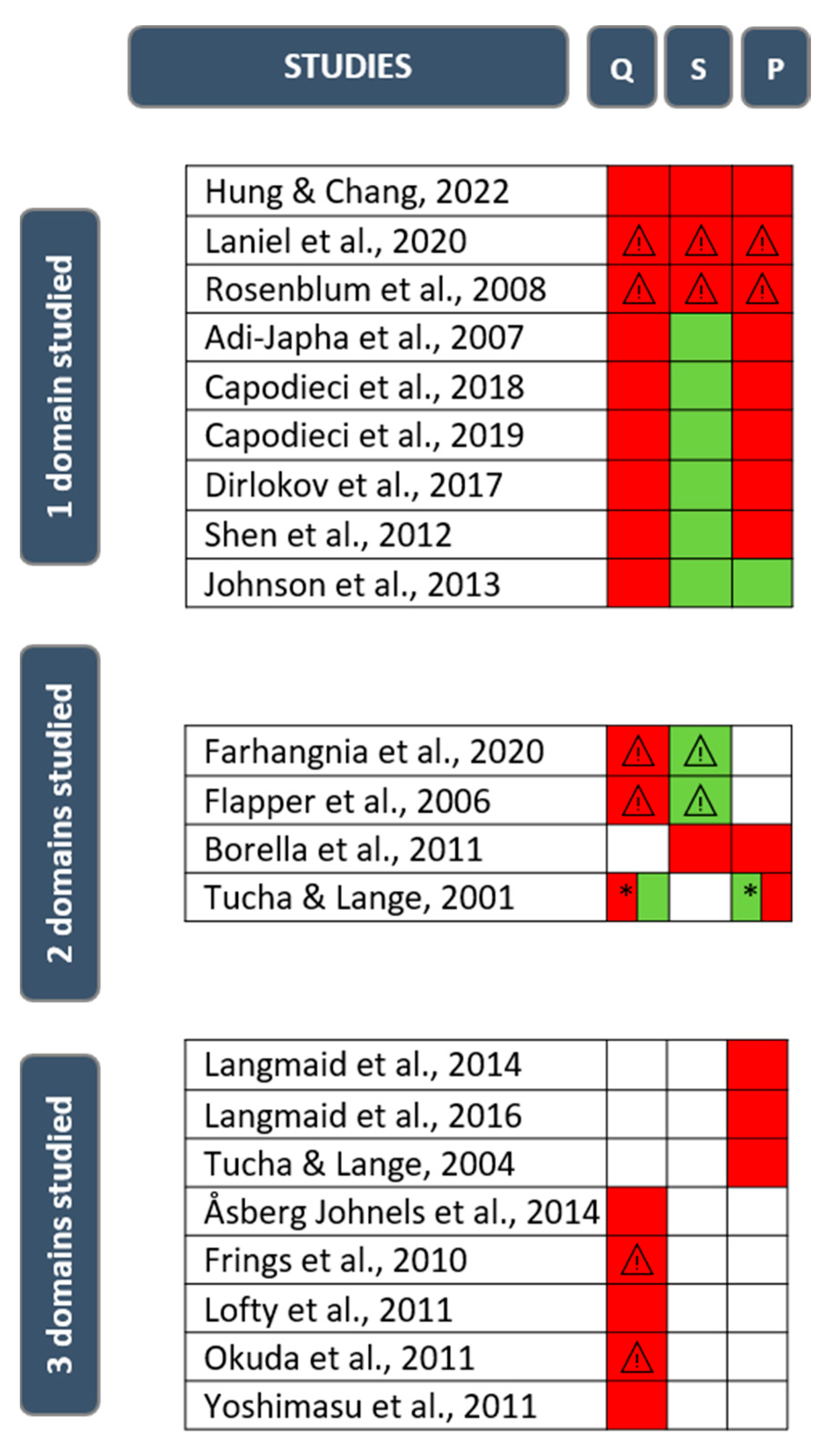
Figure 4.
Pie charts for both Step 1 and Step 2 analyses for product of handwriting. Proportion of studies showing differences between ADHD and typically developing children regarding quality/legibility (Panel A) and speed (Panel B) of handwriting before (Step 1) and after (Step 2) exclusion of unsatisfactory studies due to major methodological biases.
Figure 4.
Pie charts for both Step 1 and Step 2 analyses for product of handwriting. Proportion of studies showing differences between ADHD and typically developing children regarding quality/legibility (Panel A) and speed (Panel B) of handwriting before (Step 1) and after (Step 2) exclusion of unsatisfactory studies due to major methodological biases.
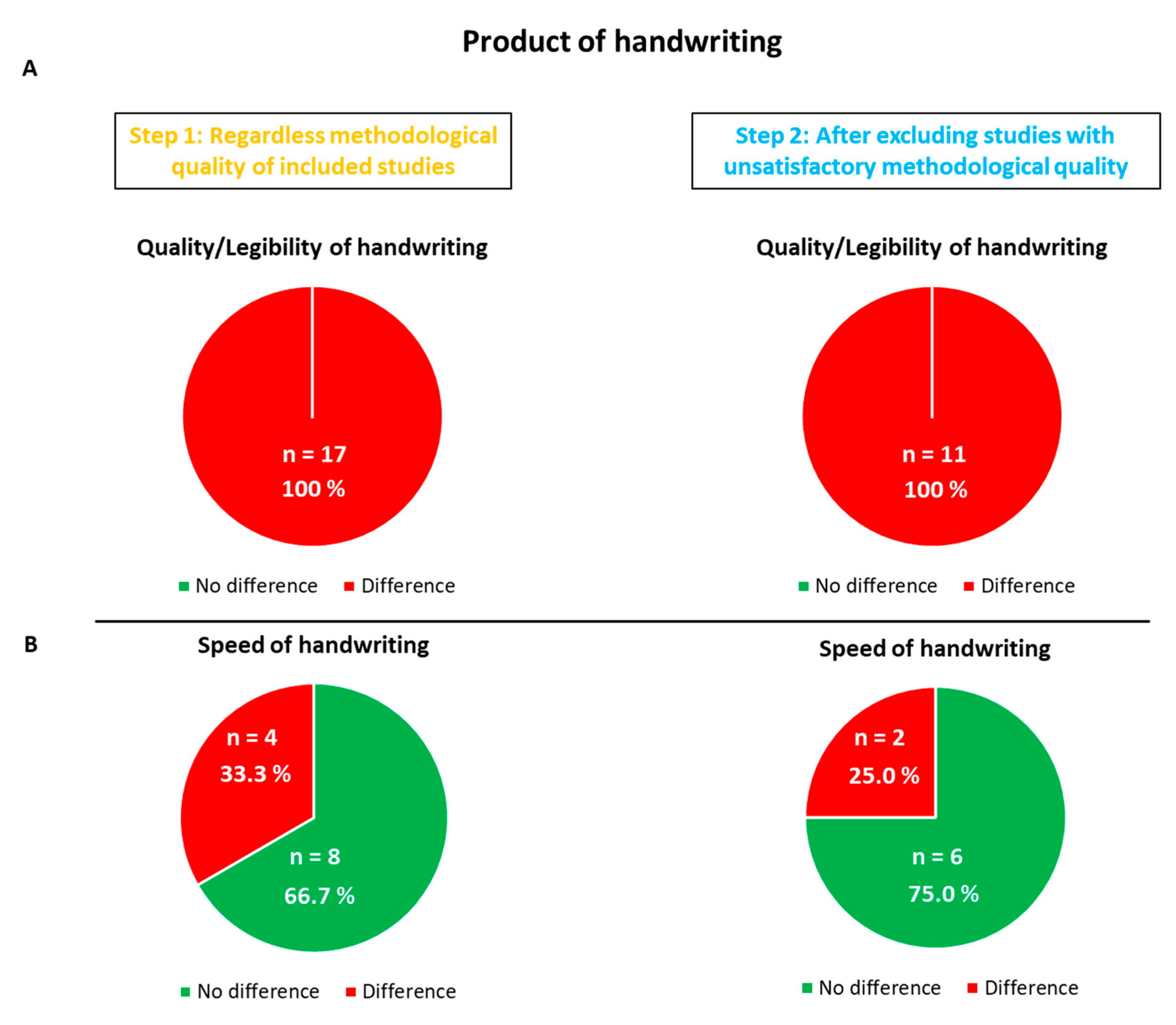
Figure 5.
Pie charts for both Step 1 and Step 2 analyses for process of handwriting. Proportion of studies showing differences between ADHD and typically developing children regarding process of handwriting before (Step 1) and after (Step 2) exclusion of unsatisfactory studies due to major methodological biases.
Figure 5.
Pie charts for both Step 1 and Step 2 analyses for process of handwriting. Proportion of studies showing differences between ADHD and typically developing children regarding process of handwriting before (Step 1) and after (Step 2) exclusion of unsatisfactory studies due to major methodological biases.
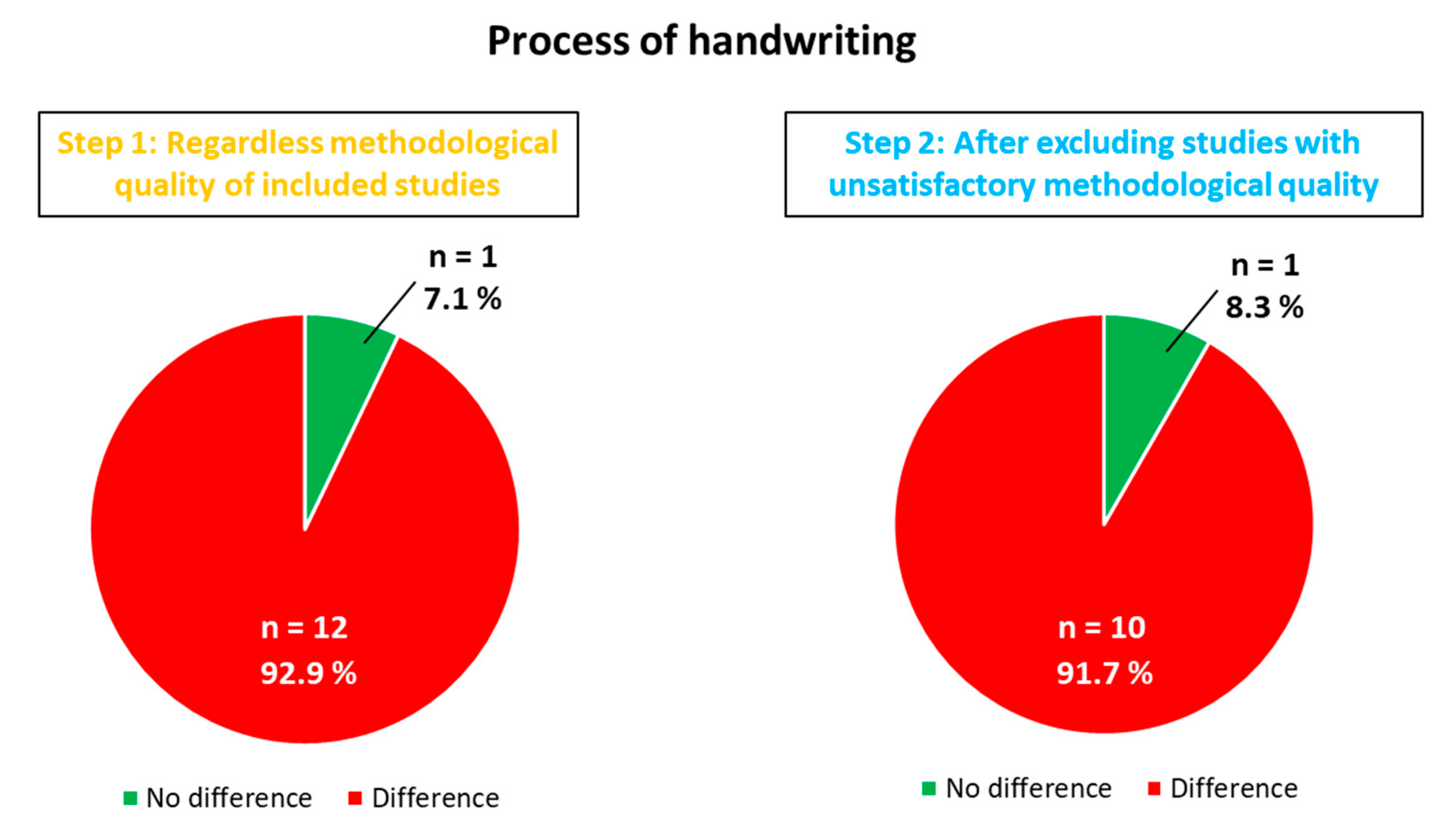

Table 1.
Critical Appraisal Skills Program (CASP).
| Section | Question | Formulation |
|---|---|---|
| A: Are the results of the trial valid? | 1 | Did the study address a clearly focused issue? |
| 2 | Did the authors use an appropriate method to answer their question? | |
| 3a | Were the cases recruited in an acceptable way? | |
| 3b | Was there a sufficient number of cases selected? | |
| 4 | Were the control groups selected in an acceptable way? | |
| 5 | Was the exposure clearly defined and accurately measured? | |
| 6 | Have the authors taken account of the potential confounding factors in the design and/or in their analysis? | |
| B: What are the results? | 7 | Was the group effect large? |
| 8 | Was the estimate of the group effect precise? | |
| 9 | Do you believe the results? | |
| C: Would the results help locally? | 10 | Can the results be applied to the local population? |
| 11 | Do the results of this study fit with other available evidence? |
Table 2.
Methodological Quality of Included Studies Scored with CASP List for Systematic Review.
| Methodological Quality | Presentation of Results | External Validity | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3a | 3b | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Adi-Japha et al., 2007 | Y | Y | Y | Y | Y | Y | Y | C | N | Y | C | Y | ||
| Åsberg Johnels et al., 2014 | Y | Y | Y | Y | Y | Y | Y | C | N | Y | Y | Y | ||
| Borella et al., 2011 | Y | Y | C | Y | Y | Y | Y | C | C | Y | Y | Y | ||
| Capodieci et al., 2018 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Capodieci et al., 2019 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Dirlikov et al., 2017 | Y | Y | Y | Y | Y | Y | Y | C | N | Y | Y | Y | ||
| Farhangnia et al., 2020 | Y | Y | C | Y | Y | Y | N | C | N | C | C | Y | ||
| Flapper et al., 2006 | Y | Y | Y | N | Y | Y | Y | C | N | C | Y | Y | ||
| Frings et al., 2010 | Y | Y | C | N | Y | Y | N | C | N | C | C | Y | ||
| Hung & Chang, 2022 | Y | Y | C | Y | Y | Y | C | Y | Y | Y | Y | Y | ||
| Johnson et al., 2013 | Y | Y | Y | N | Y | Y | Y | C | N | Y | Y | Y | ||
| Langmaid et al., 2014 | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | ||
| Langmaid et al., 2016 | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Laniel et al., 2020 | Y | Y | N | N | Y | Y | N | Y | Y | C | C | Y | ||
| Lofty et al., 2011 | Y | Y | C | Y | C | Y | C | C | N | Y | C | Y | ||
| Okuda et al., 2011 | Y | Y | Y | N | Y | Y | C | C | N | C | C | Y | ||
| Rosenblum et al., 2008 | Y | Y | Y | N | Y | Y | C | C | N | C | C | Y | ||
| Shen et al., 2012 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Tucha & Lange, 2001 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Tucha & Lange, 2004 | Y | Y | Y | N | Y | Y | Y | C | N | Y | C | Y | ||
| Yoshimasu et al., 2011 | Y | Y | Y | Y | Y | Y | N | C | N | Y | C | Y | ||
Abbreviations: Y: Yes; N: No; C: Can’t Tell.
Table 3.
Characteristics and Results of Included Studies.
| Study | Participants (ADHD and Controls) | Experimental Group | Mean Age (SD) | Gender (Male, Female) | Control Group | Mean Age (SD) | Gender | Inclusion and Exclusion Criteria for ADHD | ADHD Presentation | Medication (Psychostimulant) | Handwriting Measures |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adi-Japha et al., 2007 | 40 | 20 | 12.2 (5.7) | 20 M | 20 | 12.8 (3.6) | 20 M | Inclusion criteria: formal diagnosis of ADHD, IQ score > 85, performance within 1.6 SD on a reading test; Exclusion criteria: reading problems | ADHD/C | Off-state for at least a week before the experiment | Graphic production on a digitizing tablet; Letters production |
| Åsberg Johnels et al., 2014 | 55 | 20 | 10 to 16 | 20 F | 35 | 10 to 16 | 35 F | Inclusion criteria: formal diagnosis of ADHD, IQ score > 69; Exclusion criteria: ASD, neuropsychiatric and neurodevelopmental disorders, learning disabilities | n.s | No medication | FTF; Parental ratings |
| Borella et al., 2011 | 30 | 15 | 9.3 (1.4) | 12 M; 4 F | 15 | 9.4 (1.4) | 12 M; 3 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: IQ score < 85, MPH medication, learning disability, mathematical or reading disorders, neurological, sensory, motor, psychiatric or mood disorders | 5 ADHD/I; 10 ADHD/C | No medication | Batteria per la valutazione delle competenze ortografiche nella scuola dell’obbligo; Continuous letters production |
| Capodieci et al., 2018 | 32 | 16 | 10.5 (6.9) | 12 M; 4 F | 16 | 10.1 (6.4) | 12 M; 4 F | Inclusion criteria: formal diagnosis of ADHD for only one child, all others on the basis of ad-hoc questionnaire; Exclusion criteria: neurological, psychiatric or serious psychological problems; No child had a learning disability | n.s | No medication | BVSCO-2; Words production |
| Capodieci et al., 2019 | 52 | 26 | 9.6 (1.2) | 22 M; 4 F | 26 | 9.3 (1.1) | n.s | Inclusion criteria: formal diagnosis of ADHD for all but 3 children; Exclusion criteria: neurological or psychological problems, learning disorders | 10 ADHD/I; 10 ADHD/C; 6 ADHD/HI | No medication | BVSCO-2; Dictation tasks; Sentences and words production; Handwriting Legibility Scale |
| Dirlokov et al., 2017 | 167 | 45 | 9.9 (1.2) | 39 M; 6 F | 65 | 9.9 (1.1) | 56 M; 9 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: intellectual disability, seizure, neurological, chronic medical, genetic, psychiatric (except ODD), speech-related, autistic and psychotic disorders | 7 ADHD/I; 38 ADHD/C | Off-state for at least 24 hrs before the experiment | MHA; Copy task |
| Farhangnia et al., 2020 | 48 | 24 | 8.0 (0.7) | 17 M; 7 F | 24 | 8.1 (0.6) | 17 M; 7 F | n.s | n.s | n.s | PHAT; Copy task and dictation task |
| Flapper et al., 2006 | 24 | 12 | 9.8 (1.7) | 11 M; 1 F | 12 | 9.7 (1.2) | 11 M; 1 F | Inclusion criteria: formal diagnosis of ADHD+DCD; Exclusion criteria: learning, neurological or psychiatric disorders, IQ score < 70 | 6 ADHD/I; 4 ADHD/C; 2 ADHD/HI | Off-state for the first assessment; On-state for 4 to 5 weeks for the second assessment | BHK; Copy task |
| Frings et al., 2010 | 21 | 10 | 12.3 (1.3) | 10 M | 11 | 12.1 (1.8) | 9 M; 2 F | Inclusion criteria: formal diagnosis of ADHD | 10 ADHD/C | On-state | Copy task |
| Hung & Chang, 2022 | 60 | 30 | 7.1 (0.5) | 16 M; 14 F | 30 | 7.2 (0.5) | 16 M; 14 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: ASD, seizure disorder, IQ < 80, mental retardation, mood disorders, anxiety or psychotic disorders | 9 ADHD/I; 18 ADHD/C; 3 ADHD/HI | n.s | BCBL; Copy task and dictation task |
| Johnson et al., 2013 | 35 | 14 | 11.0 (1.95) | 14 M | 21 | 11.0 (2.1) | 21 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic or neurodevelopmental disorders, intellectual disability | 14 ADHD/C | Off-state at least 24 to 72 hrs before the experiment | HPT; Copy task |
| Langmaid et al., 2014 | 28 | 14 | 10.9 (2.0) | 14 M | 14 | 10.6 (2.3) | 14 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic or neurodevelopmental disorders, intellectual disability | 14 ADHD/C | Off-state at least 24 to 72 hrs before the experiment | Cursive letters production on a digitizing tablet |
| Langmaid et al., 2016 | 28 | 14 | 10.8 (2.0) | 14 M | 14 | 10.5 (2.2) | 14 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: medical, sensory, genetic, neurodevelopmental disorders, intellectual disability | 14 ADHD/C | Off-state at least 24 to 72 hrs before the experiment | Cursive letters production at 10 mm and 40 mm on a digitizing tablet |
| Laniel et al., 2020 | 25 | 12 | 9.5 (1.1) | 8 M; 4 F | 12 | 9.9 (1.3) | 6 M; 6 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: intellectual disability; One child had ODD and anxiety disorder, another had dyspraxia | n.s | On-state | BHK; Copy task; Pen-stroke test on a digitizing tablet |
| Lofty et al., 2011 | 40 | 20 | 7.8 (1.2) | n.s | 20 | 7.8 (1.2) | 20 M | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: sensory or psychiatric disorders; 60 % of included children met criteria for dyslexia | n.s | n.s | DDS; Copy task |
| Okuda et al., 2011 | 22 | 11 | 8.6 to 11.6 | 11 M | 11 | n.s | n.s | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: sensory or psychiatric disorders | n.s | On-state | Scale of Dysgraphia |
| Rosenblum et al., 2008 | 24 | 12 | 8 to 10 | 10 M; 2 F | 12 | 8 to 10 | 10 M; 2 F | Inclusion criteria: formal diagnosis of ADHD; Exclusion criteria: other medical diagnosis | n.s | On-state | HHE on a digitizing tablet; Copy task |
| Shen et al., 2012 | 42 | 21 | 8.5 (1.2) | 17 M; 4 F | 21 | 8.5 (1.0) | 17 M; 4 F | Inclusion criteria: formal diagnosis of ADHD, with possible ODD and CD in the ADHD group; Exclusion criteria: epilepsy, severe anxiety, psychotic disorder, DCD (score < 15th centile on M-ABC 2) | 6 ADHD/I; 10 ADHD/C; 5 ADHD/HI | Off-state at least 24 hrs before the experiment | THPS; BRWT; Copy task and dictation task on a digitizing tablet |
| Tucha & Lange, 2001 | 42 | 21 | 10.7 (0.4) | 21 M | 21 | 10.5 (0.4) | 21 M | Inclusion criteria: formal diagnosis of ADHD, with medication; Exclusion criteria: concurrent psychotropic medications, ADHD/I and ADHD/HI, reading disability or spelling disorder; Four children had mathematics disability | 21 ADHD/C | Off-state at least 10 hrs before experiment and on-state 1 hr after the administration | Copy task and dictation task on a digitizing tablet |
| Tucha & Lange, 2004 | 20 | 10 | 9.9 (n.s) | 5 M; 5 F | 10 | 9.9 (n.s) | 5 M; 5 F | Inclusion criteria: formal diagnosis of ADHD, with possible ODD and CD in the ADHD group; Exclusion criteria: neurological and psychiatric disorders | n.s | On-state | Sentences production on a digitizing tablet |
| Yoshimasu et al., 2011 | 5699 | 379 | 10.4 (4.6) | 284 M; 95 F | 5320 | n.s | 2666 M; 2654 F | Inclusion criteria: retrospective cohort-based study which has sought formal diagnosis of ADHD (based on DSM criteria); Exclusion criteria: IQ score < 50, written language disorder with or without reading disability | n.s | Possible medication | Information retrieved from individualized education program goals for written language and/or specific writing subtest scores ≤ 90; Legibility and/or writing subtest scores |
Abbreviations: ADHD: Attention Deficit Hyperactivity Disorder; ADHD/C: Combined Presentation; ADHD/I: Inattentive Presentation; ADHD/HI: Hyperactive-Impulsive Presentation; ASD: Autism Spectrum Disorders; BCBL: Battery of Chinese Basic Literacy; BHK: Concise Assessment Scale for Children’s Handwriting; BRWT: Basic Reading and Writing Comprehensive Test; BVSCO-2: Batteria di Valutazione della Scrittura e della Competenza Ortografica 2; CD: Conduct Disorder; DCD: Developmental Coordination Disorder; DDS: Dysgraphia Disability Scale; DSM: Diagnostic and Statistical Manual; F: Female; FTF: Five to Fifteen Questionnaire; HHE: Hebrew Handwriting Evaluation; HPT: Handwriting Performance Test; IIV: Intra-Individual Variability; IQ: Intelligence Quotient; M: Male; MHA: Minnesota Handwriting Assessment; MPH Methylphenidate; n.s: Not Specified; ODD: Oppositional Defiant Disorder; PHAT: Persian Handwriting Assessment Tool; THPS: Tseng Handwriting Problem Checklist; WM: Working Memory.
Table 4.
Main results of included studies.
| Study | Main Results |
|---|---|
| Adi-Japha et al., 2007 | ADHD children made more errors regarding letter insertions, substitutions, transpositions and omissions, produced confused shaped letters and replaced end-of-word letter with its simpler and more common middle-of-the-word version; Speed of handwriting did not differ between groups; No difference considering spatial features; ADHD children displayed poor time utilization, produced inconsistent and disproportionate writing accompanied by high levels of pressure and multiple corrections; Handwriting problems were associated with attentional problems and reflected an impairment in the graphemic buffer and in kinematic motor production |
| Åsberg Johnels et al., 2014 | ADHD children obtained lower scores on parental ratings of handwriting |
| Borella et al., 2011 | ADHD children produced fewer writing sequences than control groups; ADHD children showed greater IIV than control groups |
| Capodieci et al., 2018 | No difference between groups considering handwriting speed; In condition without WM interference, ADHD children produced about 10 % fewer graphemes than control groups; In spatial condition, difference between groups was slightly greater (- 20 %), though not statistically significant; In verbal condition, ADHD children wrote significantly more slowly (- 38 %) than control groups; Handwriting of ADHD children was generally less legible than control groups, especially in verbal and spatial condition; ADHD group had a higher IIV in verbal condition than control groups; High IIV influenced the reduced speed in the case of the verbal condition for both groups |
| Capodieci et al., 2019 | ADHD children made more spelling mistakes than control groups in all conditions; ADHD children who better coped with a concurrent verbal WM load had better spelling performance; ADHD children obtained lower scores for handwriting quality than control groups; No difference between groups in terms of writing speed |
| Dirlokov et al., 2017 | ADHD children showed worse letter-form scores compared to control groups across conditions (copy, trace, fast trace); No difference in letter-spacing errors between groups; ADHD children made fewer speed inflections across conditions compared to control groups; Both groups showed a significant correlation between letter form and WM performance in the copy condition only |
| Farhangnia et al., 2020 | In the copy task, ADHD children had lower global legibility scores compared to control groups; No significant difference between the two groups for space, alignment, size of letters and slant components of writing as well as for speed of writing; In the dictation task, ADHD children had lower legibility score compared to control groups while there was no difference between the groups in terms of space, alignment and slant components and size of letters |
| Flapper et al., 2006 | ADHD+DCD children showed lower scores on quality of handwriting but there was no difference in speed of handwriting between groups; When on-state, of the 11 children with ADHD+DCD who could be assessed a second time, 6 improved their handwriting quality on the BHK, 4 did not improve and one child deteriorated; When assessed off-state, ADHD+DCD children did not improve their handwriting speed |
| Frings et al., 2010 | Mean letter height did not differ between groups; Letter height increased during repeated writing of the same sentence in the ADHD group only |
| Hung & Chang, 2022 | ADHD children had poorer writing performance than the control groups in both character dictation and character copying; ADHD children wrote less fluently and correctly compared to the control groups; Inattention was the stronger predictor of character dictation in ADHD children; Manual dexterity was significantly correlated with character copying in the ADHD group |
| Johnson et al., 2013 | ADHD children made more total handwriting errors than control groups (i.e. correction and formation errors); No difference between groups in average height or width; No difference in the coefficient of variability of phrase height and width; No difference in average word spacing; ADHD children included additional strokes more often than control groups; There was a trend towards significant difference between the groups in terms of speed of handwriting, yet not significant; In the ADHD group, more corrections were associated with slower handwriting speed and maturational processes contributed to handwriting performance |
| Langmaid et al., 2014 | ADHD children were more variable in terms of stroke length and showed inconsistent stroke height when compared to the control groups; No difference in the other kinematic variables; Symptom severity scores were correlated to variability of stroke height (vertical size); Higher scores on the inattentive and total ADHD subtests were significantly correlated with more variable writing size; Stroke duration was significantly related to hyperactive behavior such that a more hyperactive child had strokes of shorter duration (faster writing); Ballisticity was significantly associated with hyperactive behavior (more ballistic movement when symptoms of hyperactivity increased) |
| Langmaid et al., 2016 | Despite both groups being significantly more inaccurate on the 40 mm task compared to 10 mm, ADHD children were unable to maintain the size of their cursive letter at the 40 mm size contrary to control groups; Groups were comparable on the 10 mm task; ADHD children had more ballistic movements on both tasks; Only pen pressure was positively correlated with inattention scores during the 10 mm task |
| Laniel et al., 2020 | ADHD children showed poorer performance on quality scores (BHK), lower writing speed and higher writing size than control groups; On the Pen-stroke test, ADHD children displayed poorer motor planning and execution and greater variability in motor control than the control groups; In the ADHD group only, motor planning on the handwriting task correlated with speed of handwriting on BHK (the faster a child wrote, the shorter the motor production delay); ADHD children showed greater amplitude of movement on the Pen-stroke test which was associated with faster motor speed; No relationship between inattention and hyperactivity symptoms with motor control skills was measured on the Pen-stroke test |
| Lofty et al., 2011 | 10 % of ADHD children had normal handwriting with no disability, 40% had excellent handwriting with a minimum of disability and 50% of ADHD children showed mild to moderate handwriting disability; ADHD children had poorer performance in respecting lines, spacing between words, letter direction, spelling a sentence and punctuation (item of the DDS); No difference between males and females in the ADHD group only on DDS scores; No correlation between DDS scores and age in the ADHD group only |
| Okuda et al., 2011 | ADHD children manifested poorer performance regarding flowing lines, descending lines, retouched letters, curvatures and angles of "m", "n" and "u" letters; They produced more collisions and adherences, sudden movements, irregular size and incorrect form of letters |
| Rosenblum et al., 2008 | Poorer performance of ADHD children when off-state versus on-state on most handwriting process and product measures; When off-medication, ADHD children showed more total time and more in-air time than when on-medication and compared to control groups; No difference in handwriting speed when compared on-state and off-state while on-state and off-state ADHD children wrote faster than control groups; No difference in product handwriting between on-state and off-state but ADHD children regardless of on or off-state differed in comparison to control groups |
| Shen et al., 2012 | ADHD children scored lower on THSPC and on BSRWT; Despite speed of writing per se being no different between the two groups, ADHD children spent more on-paper time on the copy task and hence needed more time to end a copy task |
| Tucha & Lange, 2001 | When off-state, the quality of handwriting specimens of hyperactive boys was poorer than on-state but more fluent; When off-state, ADHD children did not differ from control groups in handwriting movements; Hyperactive behavior improvement through MPH was associated with increased legibility and greater accuracy of handwriting |
| Tucha & Lange, 2004 | When on-state, ADHD children displayed significantly more inversions in the direction of their velocity profiles than control groups; When off-state, there was no difference between the groups; The medication resulted in increased dysfluency during handwriting |
| Yoshimasu et al., 2011 | ADHD girls tended to have a single specific writing difficulty whereas ADHD boys were more likely to have multiple writing difficulties (e.g. legibility + poor paragraph organization) |
Table 5.
Recommendations for Future Research aimed at investigating handwriting skills in ADHD populations.
Table 5.
Recommendations for Future Research aimed at investigating handwriting skills in ADHD populations.
| Recommendations | Level |
|---|---|
| Eligible Population | |
| Ensure a reasonable sample size necessary to conduct the study | high |
| Verify the diagnosis of ADHD by formal diagnosis following DSM-5 indications and use of gold standard tools | high |
| Verify the diagnosis of HD by standardized, valid and reliable tools | high |
| Harmonize the comparator group(s) with previous studies to facilitate comparison | |
| ADHD only | high |
| HD only | high |
| Typical | high |
| Harmonize the reference group with previous studies to facilitate comparison | |
| ADHD+HD | high |
| Ensure children acceptability (motivation to study participation) | low |
| Subgroup Analysis | |
| Consider demographic characteristics | |
| age | high |
| gender | high |
| handless | low |
| IQ | high |
| socioeconomic factor | low |
| ethnicity | low |
| cultural background | low |
| Including documentation of ADHD subtypes | high |
| Screen for comorbid emotional or behavioral conditions (eg, anxiety depression, sleep disturbance) | high |
| Screen for comorbid neurodevelopmental conditions (eg, learning and language disorders, autism spectrum disorders) | high |
| Screen for comorbid physical conditions (eg, tics). | low |
| Treatment and Care | |
| Considered ADHD specific treatment | |
| methylphenidate | high |
| other medication | low |
| behavioral interventions as treatment of ADHD or comorbidities | high |
| motor behavioral interventions (psychomotricity) | high |
| Expert Panel | |
| Harmonize measurement of key handwriting elements to facilitate pooling and comparison between study findings | high |
| Use common outcome measures to facilitate pooling and comparison between study findings | high |
| Supervise the experimental handwriting testing without knowing the child group (blind test) | low |
| Assess the handwriting performance without knowing the child group (blind evaluation) | high |
| Assess the handwriting performance by an expert panel of experiment judges (two or more) | high |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



