
Submitted:
24 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Background: Fungi are ubiquitous microorganisms that are easily dispersed through the air. In healthcare environments, indoor air can favor the spread of healthcare-associated fungal infections, compromising mainly immunocompromised hospitalized individuals. Thus, this study aimed to evaluate the indoor air contamination in healthcare environments, investigating mainly the presence of potentially pathogenic yeasts. Methods: Indoor air samples were collected from twelve healthcare environments (hospital and medical clinics). After the growth, isolation, and purification of the yeast colonies, the isolates were identified by polymerase chain reaction using species-specific primers for yeasts of the genus Candida and sequencing of D1/D2 domains of the large ribosomal subunit (LSU rRNA). Results: Fourteen yeast species were identified, including emerging pathogens. Species of clinical importance such as Candida parapsilosis, Candida orthopsilosis, Candida glabrata, Rhodotorula mucilaginosa, and Trichosporon mucoides were present. C. Parapsilosis was the most prevalent species, followed by Rodothorula mucilaginosa. Conclusions: The present study shows that potentially fungal pathogens were present in air samples from healthcare environments, proving the role of indoor air in spreading infections. Thus, monitoring air quality in healthcare environments is a fundamental approach in developing infection control measures, especially those related to invasive fungal infections.
Keywords:
Healthcare-associated infections
; indoor air quality
; infection control
; Candida
1. Introduction
Healthcare-associated infections (HAI), defined as infections related to the patient’s stay while in the hospital or in any healthcare setting [1], are a global problem and require urgent action to control the spread of pathogens within the hospital environment. Annually, more than one million hospitalized individuals are affected by HAIs, and the associated mortality rate is about 6% [2]. There are many factors involved in HAIs, mainly the impaired immune condition of patients and the various invasive procedures that culminate in creating alternative infection routes [3].
In this context, fungal pathogens have achieved notable prominence in recent years. This fact is mainly because of the increased susceptibility condition experienced by many hospitalized individuals, which is sometimes the result of aggressive therapeutic procedures [4]. For instance, patients who have been submitted to transplants are among the most susceptible to opportunistic fungal infections, especially those caused by Aspergillus sp. and Candida sp. [5]. One of the most frequent pathogens involved in HAI is the yeasts of the genus Candida. Invasive candidiasis is the most significant infection caused by these fungi, occurring mainly in Intensive Care Units (ICU) [6]. In neonatal ICUs, invasive candidiasis is the leading cause of morbidity and mortality in premature and low birth weight newborns [7]. In addition to these risk factors, the prevalence of opportunistic infections caused by Candida sp. can also be associated with newborns who have been submitted to invasive procedures such as the insertion of catheters [8,9].
In recent years, countless evidence has demonstrated the role of hospital indoor air in spreading and transmitting diseases caused by fungi. This observation is crucial when considering that many invasive fungal infections occurs in this environment [10]. Seervi and collaborators [11] evaluated aerial contamination in some hospital areas and verified the presence of Candida spp., including species with antifungal resistance phenotype. Many studies have also reported other potentially pathogenic yeasts in the hospital air, showing that indoor air quality plays a significant risk factor in HAI occurrence [12,13]. In addition, in outbreaks caused by Candida auris, its spread within the hospital environment was related to indoor air contamination [14,15].
Given the above stated, environmental monitoring in healthcare environments should be considered an essential strategy in knowing the factors involved in HAI occurrence, especially those caused by yeasts. Thus, considering the role that air plays in disseminating fungal pathogens, this study aimed to evaluate indoor air contamination in healthcare environments focusing on the presence of potentially pathogenic yeasts. This survey describes a significant diversity of airborne yeasts in healthcare settings, including non-albicans Candida species and other potential opportunistic pathogens.
2. Materials and Methods
2.1. Indoor air sampling
All analyses related to indoor air quality followed the recommendations set out in Resolution No. 09/2003 of Brazil’s National Health Surveillance Agency [16]. Indoor air samples were collected at various locations in 12 healthcare facilities (Medical Clinics and Hospitals), including critical areas, such as operating rooms, intensive care units (ICUs), and hemodialysis. The Andersen® single-stage impactor sampler was used for the collections, with Petri dishes of 90 x 10 mm with Dichloran Rose Bengal Chloramphenicol Agar (DRBC). The impactor was placed in the center of the room and positioned 1.5 m above the floor. The flow rate was 28.3 L/min, and the length of each collection was ten minutes, totaling 283 liters of air for each sampling. Outdoor air sampling was carried out to verify its possible influence on the bioaerosols concentration within healthcare facilities. After the collections, the plates were sealed, identified, and taken to the Laboratory of Climatized Environments of the Federal University of Alagoas for growing, isolation and identification of the microorganisms.
2.2. Isolation and conservation of yeasts
For isolation, selected yeast colonies were seeded on plates with YPDA medium (Yeast extract 1%, Dextrose 2%, Peptone 2%, Agar 2%, and Bromocresol dye) with 50 ppm of chloramphenicol and incubated in a microbiological incubator at 28°C for up to seven days. After growth, the colonies were purified by using the same culture medium. Once the culture purity was confirmed, the colonies were kept in microtubes containing 1 mL of sterile distilled water. 114 yeast isolates were obtained and identified by using molecular biology tools.
2.3. Molecular identification, comparison of sequences and phylogenetic analyses
The DNA extraction of the obtained isolates was performed according to the protocol described by [17]. The polymerase chain reaction (PCR) technique was initially used for molecular identification, using specific primers for members of the genus Candida. PCR reactions were performed in a total volume of 20µL in a 0.2 mL microtube, with the concentrations of reagents and reaction conditions according to Hsu et al. [18]. The primer sequences to identify five species of the genus Candida used in this study are shown in (Table 1).
We also performed the amplification of the D1/D2 domains of the large ribosomal subunit (LSU rRNA) for samples not identified with specific primers. The reactions were carried following the protocol described by Hesham et al. [19]. The primers used were NL1-F (5’-GCATATCAATAAGCGGAGGAAAAG-3’) and NL4-R (5’-GGTCCGTGTTTCAAGACGG-3’), and the expected fragment size was 600 bp. The amplification conditions were: initial denaturation at 94 °C for 5 min, followed by 30 cycles of 45 s at 94 °C for denaturation, 45 s at 55 °C for annealing, extension by 45 s at 72 °C and final extension step at 72 °C for 5 min. After amplification, a 5µL aliquot of the PCR products was applied on a 1.2% agarose gel and submitted to the electrophoresis in TBE buffer (Tris-Boric acid, 0.5M EDTA pH 8.0) a voltage of 85V/cm for one hour and 20 minutes. After electrophoresis, the gel was stained in ethidium bromide for two minutes and photographed using an ultraviolet light transilluminator (312 nm wavelength). The PCR products for the D1/D2 region were sent for sequencing by Macrogen Inc. (Seoul, South Korea).
The obtained sequences were evaluated to verify the degree of reliability of each of the nucleotides based on PHRED values >30, followed by the consensus assembly through the Staden Package software [20]. We initially performed local alignments using the BLAST program (Basic Local Alignment Search Tool) [21] to identify the sequenced products. For the D1/D2 region, identification at species level occurred when a sequence similarity value was above 99%. Paired comparisons were carried out between the sequences of the isolates obtained and the yeast sequences available on GenBank. The sequences were analyzed using the Species Demarcation Tool, v. 1.0 (SDT) software [22].
The nucleotide sequences corresponding to the LSU rRNA gene were aligned using the CLUSTAL W algorithm, implemented in MEGA 6 software (Molecular Evolutionary Genetics Analysis) [23]. Phylogenetic analyses were performed through the Maximum Likelihood (ML) method using the TrN+G nucleotide replacement model. The generated tree’s reliability was obtained by a statistical test of bootstrap support with a value of 1000 random pseudo-replicates. Clavispora opuntiae (accession number AY497691) was used as an outgroup in phylogenetic analyses.
All sequences of the isolates obtained in this study are publicly available on GenBank. The access numbers to the isolated sequences are: MT001237, MT001238, MT001239, MT001240, MT001241, MT001242, MT001243, MT001244, MT001245, MT001246, MT001247, MT001248, MT001249, MT001250, MT001251, MT001252, MT001253, MT001254, MT001255, MT001256, MT001257, MT001258, MT001259, MT001260, MT001261, MT001262, MT001263, MT001264, MT001265, MT001266, MT001267, MT001268, MT001269, MT001270, MT001271, MT001272, MT001273, MT001274, MT001275, MT001276, MT001277, MT001278, MT001279, MT001280, MT001281, MT001282, MT001283, MT001284 and MN966855.
3. Results
We obtained 114 yeast isolates after the collection in healthcare environments. Out of this total, 104 (91.2%) were collected from indoor air, while 10 (8.8%) were from outdoor air samples. Two samples were discarded due to low sequence quality to be correctly identified, and then only 112 isolates were analyzed. Out of this total, 63 (56.2%) were identified by specific primers for Candida genus and 49 (43.8%) by sequencing the D1/D2 region. Only Candida parapsilosis was present in the indoor air samples identified by specific primers (Table 2).
The initial analyses performed using the BLAST algorithm, and paired sequence comparisons showed considerable yeast species diversity. The identified species were Candida orthopsilosis, Candida glabrata, C. parapisilosis, Trichosporon mucoides, Rhodotorula mucilaginosa, Papiliotrema flavescens, Jaminaea lanaiensis, Fereydounia khargensis, Pseudozyma siamensis, Torulaspora delbrueckii, Pseudozyma hubeiensis, and Hortaea werneckii (Table 3). Besides, two samples showed 100% identity with yeasts of the genus Moniliella. We obtained ten isolates from outdoor air collections, and the species identified were C. parapsilosis and Cystobasidium slooffiae.
According to (Figure 1), we observed a more remarkable number of species in the hospital environment than in medical clinics. The species C. glabrata, T. mucoides, J. lanaiensis, P. siamensis, and T. delbruecki were detected only in hospital indoor air samples. In medical clinics, we observed the strict occurrence of P. flavenscens, F. khargensis, and two isolates identified as Moniliella sp. Isolates of R. mucilaginosa and C. parapsilosis were present in the hospital environment and medical clinics, with the most significant detection in hospitals. Except for C. parapsilosis, no other yeast species identified in the indoor air was present in the outdoor air.
Phylogenetic analyses were performed based on the sequencing data of the D1/D2 domain of the LSU rRNA gene, including sequences of isolates from the present study and sequences obtained from GenBank. Our analysis showed that the 49 isolates obtained were separated into three groups, according to (Figure 2). In group I, the most significant number of related species was present, namely: Fereydounia khargensis (access number KJ490644), Jaminaea lanaiensis (access number KY109812), Papiliotrema flavescens (access number EF653918), Trichosporon mucoides (access number KM821090), Cystobasidium slooffiae (access number AB566328), Moniliella sp (access number JQ798180), Pseudozyma hubeiensis (access number AB566327), Pseudozyma siamensis (access number LC053502) and Rhodotorula mucilaginosa (access number KP087899). The species belonging to group II were: Candida glabrata (access number JN032660), Torulaspora delbrueckii (access number KM521824), Candida orthopsilosis (access number KJ817161), and Candida parapisilosis (access number KJ817165). The species Hortaea werneckii (access number AB079587) was the only member of the third group.
4. Discussion
In hospitals and clinic environments, indoor air quality can aggravate infection outbreaks, favored mainly by the presence of immunocompromised or susceptible individuals in these places. In this survey, we reported indoor air contamination in healthcare environments by various yeast species. Also, our results provide evidence about exposure to airborne pathogens in hospital areas, which can determine HAI occurrence. Despite indoor air contamination by filamentous fungi, other airborne fungi, such as yeasts, can also severely threaten human health, especially in health settings.
In this study, we observed more significant indoor air contamination and a greater diversity of airborne fungi in hospital environments than in medical clinics. This observation may be due to the higher number of sick people in hospitals and the performance of specific procedures in these environments, contributing to more aerosolization and dissemination of microorganisms. Compared to other environments, hospitals constitute important reservoirs for yeasts, which can be aerosolized and spread throughout the building’s spaces. Like us, Veysi and co-authors [24] also found a higher average concentration of bioaerosols and other indoor air contaminants in hospitals than in other indoor environments. On the other hand, Guo and colleagues [25] assessed the concentration of airborne fungi in one hospital and other buildings and reported divergent results. They found that the indoor air fungal concentration in the hospital environment was lower than in homes. This discrepancy can be explained by the fact that homes are subjected to a more significant influence of factors that contribute to the increase of indoor air fungal concentration compared to hospitals. Thus, concerning healthcare environments, our finding confirms the importance of hospital settings as reservoirs for a wide range of pathogenic fungi species and their possible involvement in HAIs.
Of all identified yeasts, detecting Candida isolates is noteworthy in the hospitals and medical clinics analyzed. We have two possible explanations for this result. First, species of this genus constitute the microbiota of the human body and may have patients and workers as sources of contamination for indoor air. This assumption has already been observed in the literature, primarily reports of aerosolizing commensal bacteria from the skin and oral mucosa [26,27], which can also occur for yeasts. Second, invasive procedures in critically ill patients may also be responsible for aerosolizing Candida into the air. Mirhoseini et al. [28] also found that dental procedures significantly influence the abundance of airborne opportunistic pathogens in dental clinics. In many of the sites where airborne Candida were reported in our monitoring, there is a low occurrence of invasive procedures and a massive circulation of people (e.g., Doctor’s office and Reception). Thus, these yeasts may have been aerosolized mainly from patients’ or health professionals’ skin and oral cavities.
Investigations of the composition of bioaerosols in indoor air have primarily used a culture-dependent identification approach. However, these methods have significant limitations, sometimes making it challenging to identify microorganisms at the species level and restricting the understanding of the microbial signature of a given environment. Thus, culture-independent methods such as PCR assays and sequencing have been widely used in airborne microbiology today. Our study used a combination of culture-dependent and independent (PCR assay and Sequencing) methods, which allowed us to observe a considerable diversity of yeasts in healthcare settings. In Brazil, Venceslau and co-authors [29] evaluated indoor air contamination in critical and non-critical hospital areas and reported contamination by Candida sp. However, due to a culture-dependent approach, the authors could not identify the isolates obtained at the species level, limiting the knowledge of Candida diversity in the analyzed environments. Similar to us, Pedrosa and colleagues [30] used culture-based methods and the PCR assay to identify yeast isolates found in indoor air in critical areas at a University Hospital and reported contamination by Candida tropicalis, Candida krusei, and C. parapsilosis. Thus, combining culture-dependent and independent methods can be an exciting strategy to understand better the diversity of yeasts composing bioaerosols in healthcare settings.
Candida parapsilosis was the most prevalent species in the analyzed environments. Its detection occurred in hemodialysis and chemotherapy rooms and critical areas such as operating rooms and ICUs. This finding deserves attention since individuals in these places represent the leading risk group for infections by this emergent species. Nosocomial candidemia is a growing hospital problem in several countries, including Brazil. For example, Yamin et al. [31] reported this species as the leading cause of Candidemia in patients in ICUs and oncology wards. Also, an epidemiological surveillance study in 16 hospitals in five Brazilian regions shows that Candida sp. was the 7th most prevalent agent in cases of nosocomial bloodstream infection and that C. parapsilosis specie was the second most prevalent [32]. In agreement with our results, Souza and coauthors [33] also found this species the most frequent among yeasts isolated in air samples from neonatal intensive care units (NICU). In contrast, Sudharsanam and coworkers [34] found these indoor bioaerosols concentrations from a hospital ward and reported Candida krusei as the only yeast species found. This result difference may be due to the limited number of hospital sites analyzed. For example, while we evaluated several sites, the authors performed air sampling only in an orthopedic ward. Thus, hospital air quality assessment can be essential in providing important epidemiological data about the occurrence and spread of Candida sp. in the hospital environment. In addition, it provides data to assist in developing infection control measures.
Surprisingly, we have not detected Candida albicans in the air samples analyzed, which had already been observed in other studies [32,35]. Although C. albicans is considered one of the most important pathogens of the genus Candida, other Candida-non-albicans species have also emerged in the HAI context. We also described the detection of C. orthopsilosis and C. glabrata in the hospital reception and operating room, respectively. In line with us, studies in Brazilian hospitals and other countries have also reported detecting C. glabrata in indoor air samples [35,36]. C. orthopsilosis occurrence in hospital air samples has not yet been demonstrated in the literature until the completion of this study. This species and other Candida may be inferred as significant indoor air contaminants in hospitals. However, due to the use of culture-dependent methods for airborne yeast studies, their detection has not yet been reported. Thus, we highlight the first report on this species as a contaminant of indoor air in healthcare environments.
Here, we also reported Rhodotorula in our indoor air quality microbiological monitoring. Its detection has substantial clinical relevance because it has emerged as a significant opportunistic pathogen in recent years, especially in immunocompromised patients. In our finding, R. mucilaginosa was the second most frequent species encountered in hospitals and medical clinics, mainly in non-critical areas. Although we have not observed its occurrence in critical areas, indoor air can be essential in spreading to these places. Similarly, other studies have reported Rhodotorula sp. as an indoor air contaminant in critical and semi-critical hospital areas [37,38]. Equally, Souza et al. [33] evaluated fungal contamination of indoor air in two neonatal intensive care units and reported R. mucilaginosa. However, unlike us, the authors of this study additionally reported the presence of Rhodotorula minuta. Since Rhodotorula sp. has been recognized as a relevant opportunistic pathogen in various types of infections, studies to evaluate indoor air quality may be helpful to clarify better the role of these yeasts in the occurrence of HAIs.
Studies on fungal bioaerosols as contaminants in hospital indoor air mainly focus on filamentous fungi. Thus, there are few yeast species reported in the literature. In addition to the clinically relevant species already discussed, other yeasts with the potential to cause opportunistic infections were identified in our study. We report the first occurrence of the Trichosporon mucoides, Fereydounia khargensis, and Hortaea werneckii species in indoor air samples collected in healthcare environments. Except for H. werneckii, which is strictly associated with benign superficial infections [39], F. khargensis and T. mucoides have stood out as relevant opportunistic emerging pathogens, especially in transplanted patients, cancer patients, and critical areas [40,41]. Although Candida sp. is the most reported yeast in hospital indoor air quality analysis and the most significant in causing HAI, our results indicate that hospital air can also be an essential factor in the occurrence of invasive fungal infections by emerging or even unknown pathogens.
In order to infer a possible influence of outdoor air on the diversity of yeast species in indoor air, collections were made in open areas close to the evaluated hospitals and clinics. Overall, based on the few isolates obtained in our study, we believe that outdoor air did not influence the concentration of airborne yeast in the analyzed environments. We verified that C. parapsilosis was the most prevalent indoor air sample species detected in outdoor air. This fact may indicate a slight influence in some environments, at least for this species. Some studies have reported the contribution of outdoor air to high indoor concentrations of filamentous fungi, which has been mainly attributed to opening doors and windows [42]. Thus, the diversity of fungal contaminants observed in our study is likely to have been influenced by internal factors that must be better understood. Further studies are essential to identify the key factors influencing the concentration of airborne yeast in the healthcare setting and confirm the role of outdoor air on yeast diversity in healthcare settings.
5. Conclusions
In this study, we report a considerable diversity of yeasts in indoor air samples in healthcare facilities, with hospitals exhibiting a greater diversity of yeasts than medical clinics. Several sites were positive for airborne yeast contamination, including those with a higher probability of infections for exposed patients, such as operating rooms, ICUs, and hemodialysis. Clinically significant species such as C. parapsilosis and R. mucilaginosa were the most prevalent in the evaluated environments, in addition to opportunistic or emerging pathogens.
Our results further reinforce the evidence about the role of indoor air as an essential factor to be considered in the spread of HAI, with a greater risk for immunocompromised individuals. In this way, indoor air quality monitoring consists of a fundamental approach to target the elements involved in the aerial spread of fungal infections and guiding actions to implement effective infection control programs.
Author Contributions
Conceptualization, Eurípedes Alves da Silva Filho and Jean Phellipe Marques do Nascimento.; methodology, Jean Phellipe Marques do Nascimento, Raniele dos Santos, Mirna Samile dos Santos Silva, Mykaella Andrade de Araújo and Daniela Évelin dos Santos.; writing—original draft preparation, Jean Phellipe Marques do Nascimento and Eurípedes Alves da Silva Filho.; writing—review and editing, Eurípedes Alves da Silva Filho and Lucas Anhezini. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dadi, N.C.T.; Radochová, B.; Vargová, J.; Bujdáková, H. Impact of Healthcare-Associated Infections Connected to Medical Devices—An Update. Microorganisms. 2021, 9, 2332. [Google Scholar] [CrossRef]
- Klevens, R.M.; Edwards, J.R.; Richards, C.L.Jr.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef]
- Corrales-Fernández, M.J.; Gea-Velázquez de Castro, M.T.; Limón-Ramírez, R.; Miralles-Bueno, J.J.; Requena-Puche, J.; Aranaz-Andrés, J.M. Factores que contribuyen a la infección relacionada con la asistencia sanitaria: cómo evitarlos. Rev Calid Asis. 2011, 26, 367–375. [Google Scholar] [CrossRef]
- Suleyman, G.; Alangaden, G.J. Nosocomial Fungal Infections. Infect Dis Clin North Am. 2016, 30, 1023–1052. [Google Scholar] [CrossRef]
- Vazquez, J.A.; Miceli, M.H.; Alangaden, G. Invasive fungal infections in transplant recipients. Ther Adv Infect Dis. 2013, 1, 85–105. [Google Scholar] [CrossRef] [PubMed]
- Presente, S.; Bonnal, C.; Normand, A.C.; Gaudonnet, Y.; Fekkar, A.; Timsit, J.F.; Kernéis, S. Hospital Clonal Outbreak of Fluconazole-Resistant Candida Parapsilosis Harboring the Y132F ERG11p Substitution in a French Intensive Care Unit. Antimicrob Agents Chemother. 2023, 16, e0113022. [Google Scholar] [CrossRef]
- Caggiano, G.; Lovero, G.; De Giglio, O.; Barbuti, G.; Montagna, O.; Laforgia, N.; Montagna, M.T. Candidemia in the Neonatal Intensive Care Unit: A Retrospective, Observational Survey and Analysis of Literature Data. Biomed Res Int. 2017, 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lona-Reyes, J.C.; Gómez-Ruiz, L.M.; Cordero-Zamora, A.; Cortés-González, S.I.; Quiles-Corona, M.; Pérez-Ramírez, R.O.; Pinto-Macedo, H. Invasive candidiasis in a neonatal intensive care unit in Lagos, Nigeria. Niger Postgrad Med J. 2017, 24, 150–154. [Google Scholar]
- Ezenwa, B.N.; Oladele, R.O.; Akintan, P.E.; Fajolu, I.B.; Oshun, P.O.; Oduyebo, O.O.; Ezeaka, V.C. Invasive candidiasis in a neonatal intensive care unit in Lagos, Nigeria. Niger Postgrad Med J. 2017, 24, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, J.P.M.; Queijeiro-López, A.M.; Araújo, M.A.; Araujo, L.A.; Silva-Filho, E.A. Airborne Fungi in Indoor Hospital Environments. Int J Curr Microbiol App Sci. 2019, 5, 627–632. [Google Scholar] [CrossRef]
- Seervi, K.L.; Khatri, P.K.; Parihar, R.S.; Kulshrestha, S.; Meena, S.; Bora, A. Emergence of Drug Resistant Fungi in Hospital Air: A Need for Strict Microbiological Surveillance. Int J Curr Microbiol App Sci. 2016, 8, 2749–2772. [Google Scholar] [CrossRef]
- Mohajeri, P.; Soltani, S.; Getso, M.I.; Khatib, M.; Dastranj, M.; Farahani, A. Investigation of bio-air contamination in some hospitals of Kermanshah, Iran. Adv Hum Biol. 2019, 9, 65–70. [Google Scholar]
- valedeyni asl, F.; Arzanlo, M.; Fazlzadeh, M.; Amani, S.; Hazrati, S. Types and concentration of fungal bio-aerosols in hospital indoor air of Imam Khomeini and Alavi hospital in Ardabil city during 2016. IOH. 2017, 14, 103–113. [Google Scholar]
- Brown, C.S.; Guy, R. National Public Health Response to Candida auris in England. J Fungi. 2019, 5, 93. [Google Scholar] [CrossRef] [PubMed]
- Kenters, N.; Kiernan, M.; Chowdhary, A.; Denning, D.W.; Pemán, J.; Saris, K.; Schelenz, S.; Tartari, E.; Widmer, A.; Meis, J.F.; Voss, A. Control of Candida auris in healthcare institutions: Outcome of an International Society for Antimicrobial Chemotherapy expert meeting. Int J Antimicrob Agents. 2019, 54, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Agência Nacional de Vigilância Sanitária. Resolução-RE Nº 09. Ministério da Saúde do Brasil. 2003, 1–14.
- Silva-Filho, E.A.; Santos, S.K.B.; Resende, A.M.; Morais, J.O.F.; Morais, M.A.; Simões, D.A. Yeast population dynamics of industrial fuel-ethanol fermentation process assessed by PCR-fingerprinting. Anton Leeuw Int J G. 2005, 88, 13–23. [Google Scholar] [CrossRef]
- Hsu, M.; Chen, K.; Lo, H.; Chen, Y.; Liao, M.; Lin, Y.; Li, S. Species identification of medically important fungi by use of real-time LightCycler PCR. J Med Microbiol. 2003, 52, 1071–1076. [Google Scholar] [CrossRef]
- Hesham, A.E.; Wambui, V.; Ogola, J.O.H.; Maina, J.M. Phylogenetic analysis of isolated biofuel yeasts based on 5.8S-ITS rDNA and D1/D2 26S rDNA sequences. J Genet Eng Biotechnol. 2014, 12, 37–43. [Google Scholar] [CrossRef]
- Staden, R.; Judge, D.P.; Bonfield, J.K. Analyzing Sequences Using the Staden Package and EMBOSS. In Introduction to Bioinformatics; Krawetz, S.A., Womble, D.D., Eds.; Humana Press: Totowa-NJ, United States, 2003; pp. 393–410. [Google Scholar]
- Altschul, S.F.; Gish, W.; Miller, W.; Myers, E.W.; Lipman, D.J. Basic local alignment search tool. J Mol Biol. 1990, 215, 403–410. [Google Scholar] [CrossRef]
- Muhire, B.; Martin, D.P.; Brown, J.K.; Navas-Castillo, J.; Moriones, E.; Zerbini, F.M.; Rivera-Bustamante, R.; Malathi, V.G.; Briddon, R.W.; Varsani, A. A genome-wide pairwise-identity-based proposal for the classification of viruses in the genus Mastrevirus (family Geminiviridae). Arch Virol. 2013, 158, 1411–1424. [Google Scholar] [CrossRef]
- Tamura, K.; Peterson, D.; Peterson, N.; Stecher, G.; Nei, M.; Kumar, S. MEGA5: Molecular Evolutionary Genetics Analysis Using Maximum Likelihood, Evolutionary Distance, and Maximum Parsimony Methods. Mol Biol Evol. 2018, 183, 591–596. [Google Scholar] [CrossRef]
- Veysi, R.; Heibati, B.; Jahangiri, M.; Kumar, P.; Latif, M.T.; Karimi, A. Indoor air quality-induced respiratory symptoms of a hospital staff in Iran. Environ. Monit. Assess. 2019, 191, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guo, K.; Qian, H.; Ye, J.; Sun, F.; Zhuge, Y.; Wang, S.; Liu, C.; Cao, G.; Zheng, X. Assessment of airborne bacteria and fungi in different-type buildings in Nanjing, a hot summer and cold winter moist Chinese city. Build Environ. 2021, 205, 108258. [Google Scholar] [CrossRef]
- Adams, R.I.; Bhangar, S.; Pasut, W.; Arens, E.A.; Taylor, J.W.; Lindow, S.E.; Nazaroff, W.W.; Bruns, T.D. Chamber bioaerosol study: outdoor air and human occupants as sources of indoor airborne microbes. PLoS One. 2015, 10, e0128022. [Google Scholar] [CrossRef] [PubMed]
- Zemouri, C.; Volgenant, C.M.C.; Buijs, M.J.; Crielaard, W.; Rosema, N.A.M.; Brandt, B.W.; Laheij, A.M.G.A.; De Soet, J. J. Dental aerosols: microbial composition and spatial distribution. J. Oral Microbiol. 2020, 12, 1762040. [Google Scholar] [CrossRef]
- Mirhoseini, S.H.; Koolivand, A.; Bayani, M.; Sarlak, H.; Moradzadeh, R.; Ghamari, F.; Sheykhan, A. Quantitative and qualitative assessment of microbial aerosols in different indoor environments of a dental school clinic. Aerobiologia (Bologna). 2021, 37, 1–8. [Google Scholar] [CrossRef]
- Venceslau, E.M.; Martins, R.P.P.; Oliveira, I.D. Frequency of airborne fungus in critical areas at hospital unit of Aracaju, Sergipe, Brazil. RBAC. 2012, 44, 26–30. [Google Scholar]
- Pedrosa, K.P.; do Nascimento, J.P.M.; Araújo, M.A.; Silva, M.S.S.; Santos, D.E.; Silva-Filho, E.A. Airborne Fungi in a Neonatal Intensive Care Unit and Operating Theater in a University Hospital. International Journal for Innovation Education and Research. 2022, 10, 41–55. [Google Scholar] [CrossRef]
- Yamin, D. 1.; Husin, A.; Harun, A. Distribution of candidemia in Malaysian tertiary care hospital revealed predominance of Candida parapsilosis. Trop. Biomed. 2020, 37, 903–910. [Google Scholar] [PubMed]
- Doi, A.M.; Pignatari, A.C.C.; Edmond, M.B.; Marra, A.R.; Camargo, L.F.A.; Siqueira, R.A.; Mota, V.P.; Colombo, A.L. Epidemiology and microbiologic characterization of nosocomial candidemia from a Brazilian national surveillance program. PLoS One. 2016, 11, e0146909. [Google Scholar] [CrossRef]
- Souza, A.K.P.; Nascimento, J.P.M.; Araújo, M.A.S.; Pedrosa, K.P.S.; Tenorio, B.M.; Pires, L.L.S.; Lima, G.B.C.; Barboza, R.I.S.; Silva-Filho, E.A. Airborne Fungi in Neonatal Intensive Care Unit of a Public Hospital in Brazil. Int J Curr Microbiol App Sci. 2019, 8, 1210–1219. [Google Scholar] [CrossRef]
- Sudharsanam, S.; Swaminathan, S.; Ramalingam, A.; Thangavel, G.; Annamalai, R.; Steinberg, R.; Balakrishnan, K.; Srikanth, P. Characterization of indoor bioaerosols from a hospital ward in a tropical setting. Afr. Health Sci. 2012, 12, 217–225. [Google Scholar] [CrossRef]
- Diba, K.; Rhaimirad, M.; Makhdoomi, K.; Khorshidvand, Z.A. Identification of Candida species isolated from hospital acquired infections cases and hospital indoor environments. Afr. J. Microbiol. Res. 2012, 6, 4164–4168. [Google Scholar] [CrossRef]
- Kumar, M.R.; Prasad, S.R.; Urhekar, A.D. Incidence of Candida in Air from the Hospital Environment. Int J Adv Microbiol Health Res. 2017, 1, 29–33. [Google Scholar]
- Cordeiro, R.A.; Brilhante, R.S.N.; Pantoja, L.D.M.; Moreira-Filho, R.E.; Vieira, P.R.N.; Rocha, M.F.G.; Monteiro, A.J.; Sidrim, J.J.C. Isolation of pathogenic yeasts in the air from hospital environments in the city of Fortaleza, northeast Brazil. Braz J Infect Dis. 2010, 14, 30–34. [Google Scholar] [CrossRef]
- Sanna, C.; Marras, L.; Desogus, A.; Marras, B.; Montero, N.; Bertolino, G.; Schintu, M.; Coroneo, V. Evaluation of Rhodotorula spp. contamination in hospital environments. World J Pediatr Congenit Heart Surg. 2021, 193, 152. [Google Scholar] [CrossRef]
- Nogueira, N.; Júnior, E. Tinea Nigra na cidade de Campos dos Goytacazes, Rio de Janeiro. Revista Cienfica da FMC. 2012, 7, 20–24. [Google Scholar] [CrossRef]
- Tap, R.M.; Ramli, N.Y.; Sabaratnam, P.; Hashim, R.; Bakri, A.R.A.; Bee, L.B.; Ginsapu, S.J.; Ahmad, R.; Razak, M.F.A.; Ahmad, N. First Two Cases of Fungal Infections Associated with Multi-drug Resistant Yeast, Fereydounia khargensis. Mycopathologia. 2016, 181, 531–537. [Google Scholar] [CrossRef]
- Hunninghake, J.; Schuety, C.; Calvano, T.; Ferraro, D. Disseminated Trichosporon infection. Crit Care Med. 2019, 47, 270. [Google Scholar] [CrossRef]
- Rostami, N.; Alidadi, H.; Zarrinfar, H.; Salehi, P. Assessment of indoor and outdoor airborne fungi in an Educational, Research and Treatment Center. Ital. J. Med. 2017, 11, 52–56. [Google Scholar] [CrossRef]
Figure 1.
Prevalence of yeasts in healthcare environments and outdoor air. The circos plot displays the relative abundance of yeast species in indoor and outdoor air samples. Plots were generated from a table with the isolates obtained from D1/D2 domain sequencing from the LSU rRNA gene. The abundance of each isolate is directly proportional to the width of each ribbon connecting yeast species to its respective environment in which air samples were obtained. The outer ring represents the cumulative percent of isolates assigned to a given yeast species from each indoor environment or outdoor air sample. The inner circle represents the number of isolates assigned to a given species in a given sample (indoor or outdoor air).
Figure 1.
Prevalence of yeasts in healthcare environments and outdoor air. The circos plot displays the relative abundance of yeast species in indoor and outdoor air samples. Plots were generated from a table with the isolates obtained from D1/D2 domain sequencing from the LSU rRNA gene. The abundance of each isolate is directly proportional to the width of each ribbon connecting yeast species to its respective environment in which air samples were obtained. The outer ring represents the cumulative percent of isolates assigned to a given yeast species from each indoor environment or outdoor air sample. The inner circle represents the number of isolates assigned to a given species in a given sample (indoor or outdoor air).
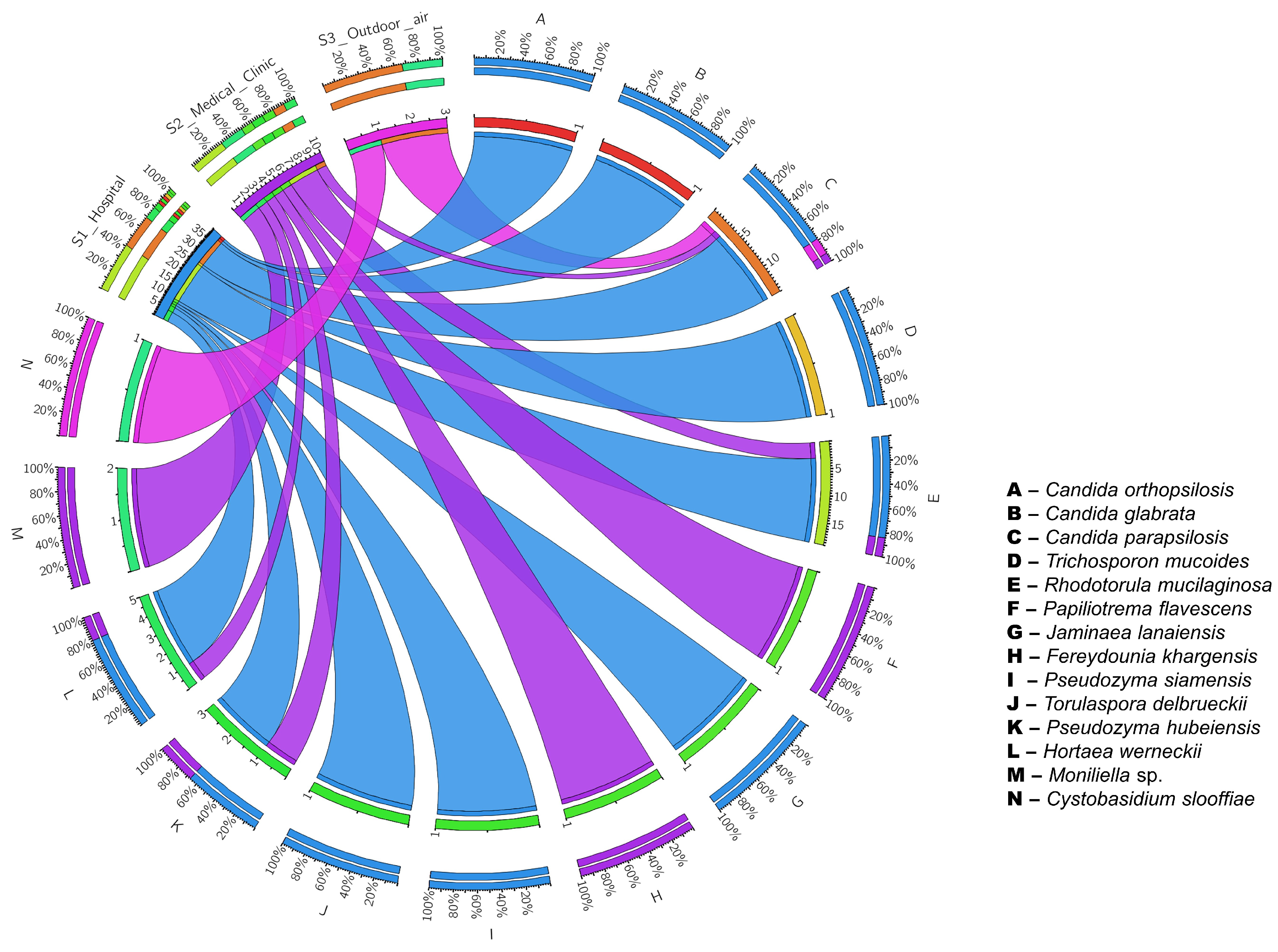
Figure 2.
Phylogenetic tree of maximum-likelihood generated by the PhyML software built based on the multiple alignments of partial sequences of the yeast LSU rRNA gene. The nucleotide replacement model used was TrN+G, provided by the jModeltest software. Node numbers indicate percentage bootstrap values (1000 bootstraps). Clavispora opuntiae was used as an outgroup.
Figure 2.
Phylogenetic tree of maximum-likelihood generated by the PhyML software built based on the multiple alignments of partial sequences of the yeast LSU rRNA gene. The nucleotide replacement model used was TrN+G, provided by the jModeltest software. Node numbers indicate percentage bootstrap values (1000 bootstraps). Clavispora opuntiae was used as an outgroup.
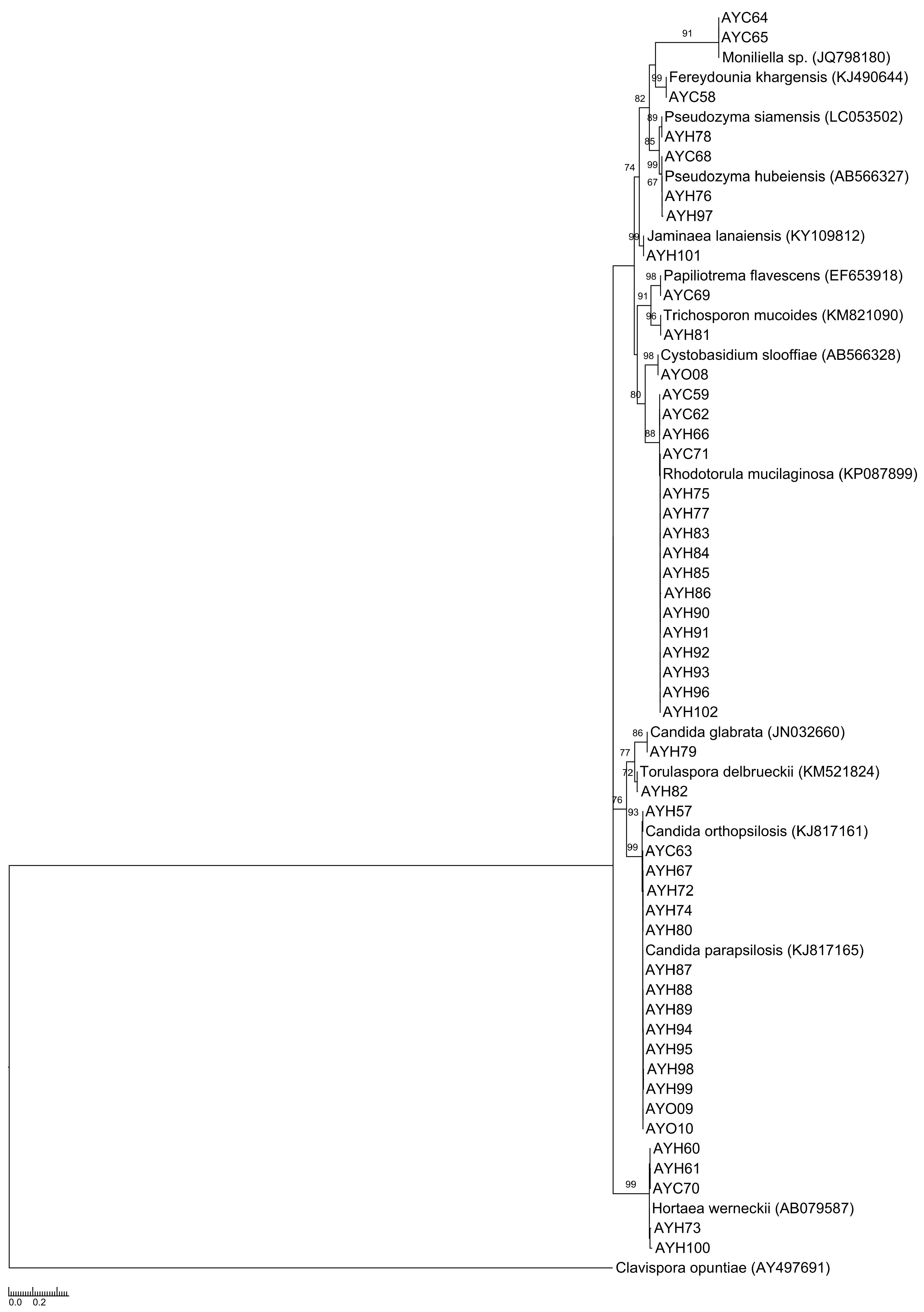

Table 1.
Oligonucleotides sequence used for the molecular identification of species of the genus Candida.
Table 1.
Oligonucleotides sequence used for the molecular identification of species of the genus Candida.
| Species | Sequences (5’-3’)* | Size (pb) |
|---|---|---|
| Candida krusei | CKRU1:GCATCGATGAAGAACGCAGC CKRU2:AAAAGTCTAGTTCGCTCGGGCC | 258 |
| Candida albicans | CALB1:TTTATCAACTTGTCACACCAGA CALB2:ATCCCGCCTTACCACTACCG | 273 |
| Candida parapsilosis | CPA1:GCCAGAGATTAAACTCAACCAA CPA2:CCTATCCATTAGTTTATACTCCGC | 300 |
| Candida tropicalis | CTR1:CAATCCTACCGCCAGAGGTTAT CTR2:TGGCCACTAGCAAAATAAGCGT | 372 |
| Candida glabrata | CGL1:TTATCACACGACTCGACACT CGL2:CCCACATACTGATATGGCCTACAA | 423 |
* All sequences were obtained from the study conducted by Hsu et al. 2003.
Table 2.
Molecular identification of airborne yeasts identified in hospital (AYH code)/medical clinics (AYC code) environments and outdoor air (AYO code) by species-specific oligonucleotides.
Table 2.
Molecular identification of airborne yeasts identified in hospital (AYH code)/medical clinics (AYC code) environments and outdoor air (AYO code) by species-specific oligonucleotides.
| Sample | Environment/Collection site | Species |
|---|---|---|
| AYH01 | Hospital/Operating room | Candida parapsilosis |
| AYC02 | Medical Clinic/Doctor’s office | Candida parapsilosis |
| AYH03 | Medical Clinic/Doctor’s office | Candida parapsilosis |
| AYH04 | Hospital/Examination room | Candida parapsilosis |
| AYH05 | Hospital/Examination room | Candida parapsilosis |
| AYH06 | Hospital/Post-anesthesic care unit | Candida parapsilosis |
| AYC07 | Medical Clinic/Serology | Candida parapsilosis |
| AYC08 | Medical Clinic/Serology | Candida parapsilosis |
| AYC09 | Medical Clinic/Biochemistry laboratory | Candida parapsilosis |
| AYC10 | Medical Clinic/Collection room | Candida parapsilosis |
| AYH11 | Hospital/Urgency and Emergency | Candida parapsilosis |
| AYH12 | Hospital/Reception | Candida parapsilosis |
| AYH13 | Hospital/Reception | Candida parapsilosis |
| AYH14 | Hospital/Reception | Candida parapsilosis |
| AYH15 | Hospital/Waiting room | Candida parapsilosis |
| AYH16 | Hospital/Waiting room | Candida parapsilosis |
| AYH17 | Hospital/Waiting room | Candida parapsilosis |
| AYH18 | Hospital/Waiting room | Candida parapsilosis |
| AYH19 | Hospital/Ultrasound | Candida parapsilosis |
| AYH20 | Hospital/ICU | Candida parapsilosis |
| AYH21 | Hospital/Examination room | Candida parapsilosis |
| AYH22 | Hospital/Examination room | Candida parapsilosis |
| AYH23 | Hospital/Examination room | Candida parapsilosis |
| AYH24 | Hospital/Apartment | Candida parapsilosis |
| AYH25 | Hospital/Observation room | Candida parapsilosis |
| AYH26 | Hospital/Operating room reception | Candida parapsilosis |
| AYH27 | Hospital/Operating room reception | Candida parapsilosis |
| AYH28 | Hospital/Reception | Candida parapsilosis |
| AYH29 | Hospital/Diagnostic Center | Candida parapsilosis |
| AYH30 | Hospital/Diagnostic Center | Candida parapsilosis |
| AYH32 | Hospital/Operating room | Candida parapsilosis |
| AYH33 | Hospital/Operating room | Candida parapsilosis |
| AYH34 | Hospital/Hemodialysis | Candida parapsilosis |
| AYH35 | Hospital/Hemodialysis | Candida parapsilosis |
| AYH36 | Hospital/Hemodialysis | Candida parapsilosis |
| AYH37 | Hospital/Hemodialysis | Candida parapsilosis |
| AYH38 | Hospital/Chemotherapy | Candida parapsilosis |
| AYH39 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH40 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH41 | Hospital/Social assistance | Candida parapsilosis |
| AYH42 | Hospital/Application room | Candida parapsilosis |
| AYH43 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH44 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH45 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH46 | Hospital/Waiting room | Candida parapsilosis |
| AYH47 | Hospital/Clinical screening | Candida parapsilosis |
| AYH48 | Hospital/Occupational therapy | Candida parapsilosis |
| AYH49 | Hospital/Operating room | Candida parapsilosis |
| AYH50 | Hospital/Operating room | Candida parapsilosis |
| AYH51 | Hospital/Sterilization room | Candida parapsilosis |
| AYH52 | Hospital/Doctor’s office | Candida parapsilosis |
| AYH53 | Hospital/Application room | Candida parapsilosis |
| AYH54 | Medical Clinic/Quality control | Candida parapsilosis |
| AYH55 | Medical Clinic/Quality control | Candida parapsilosis |
| AYH56 | Medical Clinic/Recption | Candida parapsilosis |
| AYO01 | Outdoor air | Candida parapsilosis |
| AYO02 | Outdoor air | Candida parapsilosis |
| AYO03 | Outdoor air | Candida parapsilosis |
| AYO04 | Outdoor air | Candida parapsilosis |
| AYO05 | Outdoor air | Candida parapsilosis |
| AYO06 | Outdoor air | Candida parapsilosis |
| AYO07 | Outdoor air | Candida parapsilosis |
Table 3.
Molecular identification of airborne yeasts identified by sequencing the D1/D2 domains of the LSU rRNA gene in hospital (AYH code)/medical clinics (AYC code) environments and outdoor air (AYO code).
Table 3.
Molecular identification of airborne yeasts identified by sequencing the D1/D2 domains of the LSU rRNA gene in hospital (AYH code)/medical clinics (AYC code) environments and outdoor air (AYO code).
| Sample | Environment/Collection site | Species | Accession number |
|---|---|---|---|
| AYH57 | Hospital/Reception | Candida orthopsilosis | GenBank: MT001254 |
| AYC58 | Medical Clinic/Doctor’s office | Fereydounia khargensis | GenBank: MT001262 |
| AYC59 | Medical Clinic/Doctor’s office | Rhodotorula mucilaginosa | GenBank: MT001268 |
| AYH60 | Hospital/Operating room | Hortaea werneckii | GenBank: MT001237 |
| AYH61 | Hospital/Operating room | Hortaea werneckii | GenBank: MT001242 |
| AYC62 | Medical Clinic/Operating room | Rhodotorula mucilaginosa | GenBank: MT001269 |
| AYC63 | Medical Clinic/Doctor’s office | Candida parapsilosis | GenBank: MT001241 |
| AYC64 | Medical Clinic/Doctor’s office | Moniliella sp. | GenBank: MT001260 |
| AYC65 | Medical Clinic/Doctor’s office | Moniliella sp. | GenBank: MT001263 |
| AYH66 | Hospital/Procedures room | Rhodotorula mucilaginosa | GenBank: MT001270 |
| AYH67 | Hospital/Hemodialysis | Candida parapsilosis | GenBank: MT001243 |
| AYC68 | Medical Clinic/Reception | Pseudozyma hubeinsis | GenBank: MT001240 |
| AYC69 | Medical Clinic/Storage room | Papiliotrema flavescens | GenBank: MT001249 |
| AYC70 | Medical Clinic/Fractionation room | Hortaea werneckii | GenBank: MT001253 |
| AYC71 | Medical Clinic/Microbiology laboratory | Rhodotorula mucilaginosa | GenBank: MT001271 |
| AYH72 | Hospital/Observation room | Candida parapsilosis | GenBank: MT001244 |
| AYH73 | Hospital/Observation room | Hortaea werneckii | GenBank: MT001258 |
| AYH74 | Hospital/Observation room | Candida parapsilosis | GenBank: MT001245 |
| AYH75 | Hospital/Urgency and Emergency | Rhodotorula mucilaginosa | GenBank: MT001272 |
| AYH76 | Hospital/Neonatal ICU | Pseudozyma hubeiensis | GenBank: MT001247 |
| AYH77 | Hospital/Apartment | Rhodotorula mucilaginosa | GenBank: MT001273 |
| AYH78 | Hospital/Hemodialysis | Pseudozyma siamensis | GenBank: MT001251 |
| AYH79 | Hospital/Operating room | Candida glabrata | GenBank: MN966855 |
| AYH80 | Hospital/Post-anesthesia care unit | Candida parapsilosis | GenBank: MT001246 |
| AYH81 | Hospital/Storage room | Trichosporon mucoides | GenBank: MT001239 |
| AYH82 | Hospital/Audit | Torulaspora delbrueckii | GenBank: MT001238 |
| AYH83 | Hospital/Hemodialysis | Rhodotorula mucilaginosa | GenBank: MT001274 |
| AYH84 | Hospital/Observation room | Rhodotorula mucilaginosa | GenBank: MT001275 |
| AYH85 | Hospital/Waiting room | Rhodotorula mucilaginosa | GenBank: MT001276 |
| AYH86 | Hospital/Nurses station | Rhodotorula mucilaginosa | GenBank: MT001277 |
| AYH87 | Hospital/Pharmacy | Candida parapsilosis | GenBank: MT001248 |
| AYH88 | Hospital/Examination room | Candida parapsilosis | GenBank: MT001250 |
| AYH89 | Hospital/Social assistance | Candida parapsilosis | GenBank: MT001252 |
| AYH90 | Hospital/Macroscopy | Rhodotorula mucilaginosa | GenBank: MT001278 |
| AYH91 | Hospital/Macroscopy | Rhodotorula mucilaginosa | GenBank: MT001279 |
| AYH92 | Hospital/Clinical screening | Rhodotorula mucilaginosa | GenBank: MT001280 |
| AYH93 | Hospital/Occupational therapy | Rhodotorula mucilaginosa | GenBank: MT001281 |
| AYH94 | Hospital/Observation room | Candida parapsilosis | GenBank: MT001255 |
| AYH95 | Hospital/Doctor’s office | Candida parapsilosis | GenBank: MT001256 |
| AYH96 | Hospital/Administrative | Rhodotorula mucilaginosa | GenBank: MT001282 |
| AYH97 | Hospital/Application room | Pseudozyma hubeiensis | GenBank: MT001267 |
| AYH98 | Hospital/Application room | Candida parapsilosis | GenBank: MT001257 |
| AYH99 | Hospital/Telephone exchange | Candida parapsilosis | GenBank: MT001261 |
| AYH100 | Hospital/Coordination | Hortaea werneckii | GenBank: MT001259 |
| AYH101 | Hospital/Information technology | Jaminaea lanaiensis | GenBank: MT001264 |
| AYH102 | Hospital/Observation room | Rhodotorula mucilaginosa | GenBank: MT001283 |
| AYO08 | Outdoor air | Cystobasidium slooffiae | GenBank:MT001284 |
| AYO09 | Outdoor air | Candida parapsilosis | GenBank:MT001265 |
| AYO10 | Outdoor air | Candida parapsilosis | GenBank:MT001266 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



