Submitted:
30 June 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
Background: The 2021 “Universal Definition of Heart Failure (HF)” Proposed the following left ventricle ejection (LVEF) phenotype classification: ≤40%; HF with intermediate LVEF: between 41-49% and HF with preserved LVEF: ≥50%. LVEF represents the percentage of left ventricular ejected volume in each cardiac cycle and Cut-points considered statistically normal are: ≥52% in men and ≥54% in women. The prevalence HFpEF is of 35-60% among the HF phenotypes, with a facing to increase rates in relation to HFrEF and is associated with mortality rates similar to those of HFrEF. The pathophysiology of HFpEF is based on vascular and metabolic dysfunction, therefore, there is less neurohumoral stimulation compared to HFrEF. Methodology: A systematic review was performed to report of information related to Sacubitril-valsartan and the treatment of HFrEF. Terms related to “treatment” and “brazil” were used in the databases PubMed (MEDLINE) and Scientific Electronic Library Online (SCIELO). Results: Clinical trials testing drugs that modulate the neurohumoral system in patients with HFpEF failed to demonstrate benefit in the combined endpoint of reduced mortality/hospitalization due to HF compared to placebo to date. Sacubitril-valsartan is a drug with a mechanism of action surrogate the pathophysiological concept of HFpEF, it is safe and decreased endpoints of natriuretic peptides and left atrial structure in a phase II clinical study. Conclusions: The PARAGON-HF trial demonstrated that sacubitril-valsartan reduced the primary endpoint of the study when assessed the pre-specified subgroup of LVEF≤57% and improved the secondary endpoints of performance status and renal function in the population.
Keywords:
Sacubitril-valsartan
; heart failure
; ejection fraction and cardiovascular disease
1. Introduction
Heart failure (HF) is a syndrome that, from an injury of physical, chemical and metabolic factors, determines cardiovascular remodeling and dysfunction, which can result in symptoms of dyspnea and/or decreased physical performance status. According to the 2021 Universal Definition of HF, heart failure when: 1) a set of current or previous HF symptoms and/or signs caused by a structural and/or functional cardiac abnormality; and 2) supported by an increase in natriuretic peptides or by an objective evidence of cardiogenic or systemic pulmonary congestion1. Systematic search strategies were performed of literature was performed, to answer the main question was ‘How is the effect of Sacubitril-valsartan concerning the pathophysiological concept of HFpEF and the continuum of left ventricle ejection fraction”. This study also ratified the classification according to left ventricular ejection fraction (LVEF) phenotypes with slight modifications as HF with reduced LVEF ≤40% or HFrEF, HF with mildly reduced LVEF between 41- 49% or HFmrEF and HF with preserved LVEF ≥50% or HFpEF HF with improved LVEF≤40% at baseline and increases >10% on a second measure of >40%. It is important to point out that the LVEF parameters mentioned above to define the cutoff for HFpEF and HFmrEF are arbitrary and by definition based on the Gaussian distribution of this variable. LVEF is considered normal when ≥52% in men and ≥54% in women2.
2. Methods
Systematic search strategies were performed of literature was performed, to answer the main question was ‘How is the effect of Sacubitril-valsartan concerning the pathophysiological concept of HFpEF and the continuum of left ventricle ejection fraction?. Alternative or auxiliary literature searches were conducted combining global results with those from Brazil. To improve the research process, we used the PICO framework (Patients–Intervention–Comparison–Outcomes). PICO is a framework that addresses themes by developing clinical research questions prior to starting the research. According to the PICO system, the main search frame was as follows: “Patients/Population/Problem: Heart Failure”, “Intervention: Sacubitril-valsartan treatment”, “Comparison: Treatments approved/used in Brazil”, “Outcomes: Review on effectiveness and safety”.
Research questions
The main PICO question evaluated the role of Sacubitril-valsartan treating HF patients. Epidemiology and demographics of HF and the effectiveness and safety of Sacubitril-valsartan were the focus of the review.
Databases
Public and open access databases were selected for this bibliographic search. Latin American databases were included to also retrieve Brazilian papers, using ‘Brazil’ as term or ‘Portuguese’ as language limit. The query that retrieved the greater number of items was selected for each database. The searched databases were PubMed (MEDLINE) and Scientific Electronic Library Online (SCIELO)
Search process
Initially, a highly sensitive search was performed in order to retrieve as many relevant references as possible from each database. The framework query strategy was conducted with various combinations of key themes (treatment, epidemiology, demographics, effectiveness, safety, statements, guidelines, Brazil). Filters and limits were applied in order to retrieve the most recent and relevant results. All databases were searched up to 21/January/2022.Articles electronically published ahead of print were also included.
3. Results
3.1. Fundamental pathophysiological aspects in HFrEF and HFpEF
The pathophysiological context of patients with HFrEF and HFmrEF is directly related to an initial injury to the cardiac myocyte by infectious agents, toxic agents or, more frequently, by ischemia. The result is an increased oxidative stress leading to apoptosis, autophagy or cell necrosis. In this context, in the necrotic segments there is an important systolic dysfunction, fibroblasts deposit intense amounts of collagen and the sympathetic system, renin-angiotensin-aldosterone, initiate an over stimulation to keep the hemodynamic status (Figure 1).
In patients with HFpEF, the tissue injury begins with the harmful effect of multiple associated comorbidities, mainly obesity, diabetes, hypertension, but also chronic obstructive pulmonary disease (COPD) and chronic kidney disease. This metabolic milieu determines a chronic pro-inflammatory state by endothelium-cardiomyocyte signaling and coronary microvascular endothelial cells initiate the production of reactive oxygen species, decreasing the bioavailability of nitric oxide. It reduces protein kinase G activity in cardiomyocytes. The low activity of protein kinase G causes hypophosphorylation of titin, a contractile protein of the cytoskeleton, causing an increase in the passive tension of the cardiomyocyte, inducing its stiffness and hypertrophy. Simultaneously, endothelial cells also produce vascular cell adhesion molecules and E-selectin, promoting the migration of monocytes into the intima vessel. Monocytes will stimulate the conversion of fibroblasts into myofibroblasts that deposit collagen in the interstitial space, further increasing myocardial stiffness3. Therefore, in this process without myocyte death, contractility and LVEF, is preserved or slightly reduced (Figure 1). In the HFpEF generation mechanism, sympathetic stimulation and the upregulation of the renin-angiotensin-aldosterone system is much less pronounced than in HFrEF.
cGMP, cyclic guanosine monophosphate; COPD, chronic obstructive pulmonary disease; F-passive, tension at rest; IL-6, interleukin 6; NO, nitric oxide; ONOO-, peroxynitrite; GPK, G protein kinase; sGC, soluble guanylate cyclase; sST2, soluble ST2; TNF, tumor necrosis factor; VCAM, cell adhesion molecule; OS, oxidative stress. Adapted from Paulus et al2.
The result of these two distinct phenomena mentioned above is cardiac remodeling and alteration in pump function, which in HFrEF progresses with prominent systolic dysfunction and some diastolic dysfunction, and in HFpEF with diastolic dysfunction and minimal or no systolic dysfunction. From a clinical point of view, the two phenotypes share varying degrees of pulmonary and systemic congestion, determining dyspnea and pulmonary and venous edema, as well as a decrease in systemic perfusion, causing fatigue and exercise intolerance.
3.2. HFpEF and HFmrEF epidemiology in relation to HFrEF
Prevalence rates of HFpEF vary according to the origin of the population investigated, the defined LVEF cutoff, and how specialized the clinic from which the population comes. However, most studies show that at least half of patients with HF have HFpEF4.
A Brazilian registry5 allocated 633 participants from primary care in Brazil, aged ≥ 45 years, with the aim of verifying the prevalence of HF in stages A, B, C and D. Stage 0 was considered when patients did not present any risk factors and were asymptomatic. In addition, LVEF-related phenotypes were also registered. The prevalence of symptomatic HF was 9.3% (stage C) and the rate of HFpEF was 59% of this population (Figure 2). Regarding sex, HFpEF was more frequent in females and HFrEF in males.
In more selected patients from a University Hospital in southern Brazil, the prevalence of HFpEF and HFmrEF found were 51.6% and 17%, respectively, and there was no significant difference in total mortality rates between groups with different phenotypes of LVEF (Figure 3 and Figure 4). However, in relation to cardiovascular mortality, the population with HFpEF had a slightly lower rate of this endpoint when compared to the others6.
In short, regarding prevalence and endpoint rates, in Brazil and worldwide there is a large percentage of patients with HFpEF and HFmrEF with similar rates of outcomes, which therefore represent a problem with an economic impact on public health system.
4. Discussion
4.1. Contemporary pharmacological management of HF and unmet needs
The current treatment for chronic HFrEF is well established7 and is based on facing the pathophysiological damages already described in this text, that is, the relief of congestion with diuretics, control of sympathetic overstimulation with beta-blocking agents and of the renin-angiotensin-aldosterone system upregulation with angiotensin converting enzyme inhibitors, angiotensin II receptor blockers (ARB), mineralocorticoid antagonists (MCA). The angiotensin receptor antagonist/neprilysin inhibitors (ARANIs) complement the process, releasing more natriuretic peptide while blocking angiotensin II. Added to this group of drugs are sodium-glucose-transporter inhibitors (SGLT2i), a metabolic optimizer with a variety of effects not yet totally identified. All these drug classes, except diuretics, are associated with a decrease in mortality and hospitalization for heart failure and gain indication class I (Figure 5), as they act appropriate pathophysiological disorders in clinical trials.
The drug management of HFpEF is more complex. Although there is evidence that circulatory decongestion with diuretics improves quality of life, no randomized clinical trial has reduced classic hard primary endpoints such as mortality and/or hospitalization for heart failure. When secondary endpoints related to instability and need for hospitalization due to HF are analyzed, only two drug classes showed results: ARBs and MCAs. Therefore, apart from diuretics, ARB and MCA to reduce symptoms, no drug has a recommendation to reduce mortality, according to the Brazilian Guidelines on HF8 (Table 2). Among the potential rationales for this unmet need in the drug management of HFpEF is the fact that large studies have tested drugs that act by regulating the unbalanced expression of the sympathetic systems, renin-angiotensin-aldosterone, which are exacerbated metabolic responses in the classic HFrEF model, as mentioned above. Altered metabolic milieu, generating oxidative stress and endothelial dysfunction, low production of nitric oxide and its vasodilatory response, myocardial cell remodeling with resulting stiffness is the central phenomenon in HFpEF and, to a lesser degree, in HFmrEF.

Table 2.
Recommendations for HFpEF pharmacological treatment. Adapted from the Brazilian Guidelines on Heart Failure 20188,.
Table 2.
Recommendations for HFpEF pharmacological treatment. Adapted from the Brazilian Guidelines on Heart Failure 20188,.
| Recommendations | Class | Level of evidence |
|---|---|---|
| Loop diuretics or thiazides to decrease congestive symptoms | I | B |
| Treatments for comorbidities such as myocardial ischemia, AF and hypertension, according to current guidelines, to reduce symptoms or disease progression | I | C |
| Spironolactone to reduce hospitalizations | IIA | B |
| ARBs to reduce hospitalizations | IIB | B |
AF: atrial fibrillation, ARBs: angiotensin II receptor blockers.
4.2. Sacubitril-valsartan for the treatment of HFpEF and HFmrEF: pharmacological principles
The molecule initially named LCZ696 (sacubitril-valsartan) is an angiotensin II and neprilysin receptor inhibitor that comprises the molecular portions of the neprilysin inhibitory prodrug (neutral endopeptidase) AHU377 and the ARB valsartan in a single compound. The AHU377 is metabolized by enzymatic cleavage to LBQ657, the active neprilysin inhibitor. Neprilysin degrades biologically active natriuretic peptides, including atrial natriuretic peptide (ANP), B-type natriuretic peptide (BNP), and C-type natriuretic peptide, but not biologically inert NT-proBNP, which is not a substrate for this enzyme. By increasing active natriuretic peptides, inhibition of neprilysin increases the generation of guanosine 3′5′ cyclic myocardial monophosphate, which improves myocardial relaxation and reduces hypertrophy.
Natriuretic peptides also stimulate diuresis, natriuresis, vasodilation, and may have additional anti-fibrotic and anti-sympathetic effects. However, neprilysin also contributes to the degradation of angiotensin, which is the rationale for dual-action compounds that inhibit this enzyme and block the action or generation of angiotensin9.
Therefore, the functions performed by this molecule affect the classic pathophysiological component of HFpEF more forcefully, determining vasodilation, natriuresis and improvement in myocardial relaxation, as well as the HFmrEF model, determining angiotensin blockade, anti-sympathetic and anti-fibrotic effect.
4.3. Sacubitril-valsartan for the treatment of HFpEF and HFmrEF: clinical studies
The first large clinical trial with sacubitril-valsartan was first published in 20129. PARAMOUNT was a multicenter, phase 2, randomized, parallel-group, double-blind trial in patients with New York Heart Association (NYHA) functional class II – III HF, left ventricular ejection fraction of 45% or greater, and NT-proBNP greater than 400 pg/ml. Participants were randomly assigned (1:1) to receive LCZ696 titrated to up to 200 mg twice daily or valsartan titrated to up to 160 mg twice daily for 36 weeks. Investigators and participants were blinded to treatment assignment. The primary endpoint was change in NT-proBNP, a marker of left ventricular wall stress, from baseline to week12.
A total of 149 patients randomly assigned to sacubitril-valsartan and 152 to valsartan were included. For the analysis of the primary endpoint, 134 in the sacubitril-valsartan group and 132 in the valsartan group. NT-proBNP was significantly reduced at 12 weeks (Figure 6) and no difference in adverse symptom rates was observed (Table 2).
The authors concluded that sacubitril-valsartan significantly reduced NT-proBNP relative to valsartan at 12 weeks and that it was well tolerated. With these results, they generated a hypothesis that the clinical efficacy should be tested in a phase III study.
Table 2.
Serious adverse events and laboratory abnormalities.
| LCZ696 (n = 149) | Valsartan (n = 152) | P value | |
|---|---|---|---|
| Any serious adverse event Deaths Heart failure Acute Coronary Syndrome Arrhythmia Renal Any adverse event Symptomatic hypotension Kidney dysfunction Hyperkalemia Discontinuation due to AE Laboratory abnormalities Potassium >5.5 mmol/l Potassium ≥6.0 mmol/l ≥50% decrease in GFR |
22 (15%) 1 (1%) 4 (3%) 4 (3%) 2 (1%) 2 (1%) 96 (64%) 28 (19%) 3 (2%) 12 (8%) 15 (10%) 24 (16%) 5 (3%) 5 (3%) |
30 (20%) 2 (1%) 6 (4%) 4 (3%) 2 (1%) 3 (2%) 111 (73%) 27 (18%) 7 (5%) 9 (6%) 17 (11%) 16 (11%) 6 (4%) 4 (3%) |
0.32 0.99 0.77 0.74 0.63 0.98 0.14 0.88 0.34 0.50 0.90 0.21 0.97 0.98 |
Five years after the publication of the disruptive PARADIGM-HF10 study, which showed that sacubitril-valsartan caused a lower rate of hospitalization for heart failure or death from cardiovascular causes than enalapril among patients with HFrEF, the PARAGON-HF11 study was published. A total of 4822 patients with NYHA class II to IV heart failure, ejection fraction of 45% or greater, elevated levels of natriuretic peptides, and structural heart disease received sacubitril-valsartan (target dose of 97 mg sacubitril with 103 mg of valsartan two times daily) or valsartan (target dose, 160 mg twice daily).
The primary endpoint was a composite of the total number of hospitalizations for heart failure and death from cardiovascular causes. Secondary endpoints were: NYHA class change; worsening of renal function and change in the Kansas City Cardiomyopathy Questionnaire (KCCQ) for symptoms and physical limitations. Safety was also investigated.
Inclusion criteria were: age of 50 years; signs and symptoms of HF NYHA class II to IV, an LVEF of 45% or more within the last 6 months, elevated natriuretic peptide level (with different cutoffs depending on the occurrence of recent hospitalization for heart failure and the presence of atrial fibrillation or flutter), evidence of structural heart disease and diuretic therapy. Exclusion criteria were: history of LVEF <40%; myocardial infarction, coronary artery bypass graft surgery, or any event within 6 months prior to screening that could have reduced LVEF (unless confirmed LVEF of 45%); acute decompensated HF requiring therapy; treatment with two or more of the following required: ACE inhibitors, ARB or renin inhibitor; SBP <110 mmHg OR SBP>180 mmHg at screening; serum potassium >5.2 mmol/l at screening or >5.4 mmol/l at the end of each run-in period; GFR<30 ml/min/1.73m2 at screening or end of each run-in period GFR <25 ml/min/1.73m2 or reduction in GFR >35% compared to that at screening.
In the study design, a screening period called run-in, in which all patients received valsartan for the first time at half the target dose, followed by sacubitril-valsartan at half the target dose. Participants who had no unacceptable side effects in both run-in phases and whose laboratory values remained within pre-specified safety criteria were randomly assigned in a 1:1 ratio to receive double-blind treatment with sacubitril-valsartan (target dose of 97 mg sacubitril with 103 mg valsartan twice daily) or valsartan (target dose 160 mg twice daily). Patients were evaluated at trial visits every 4 to 16 weeks. Renin-angiotensin system inhibitors other than mineralocorticoid receptor antagonists were discontinued prior to the run-in period, but all other background drugs were continued. The dose of test drugs could be adjusted downward if the target dose led to unacceptable side effects (Figure 7).
For sample size calculation, it was determined that 1847 primary events would be able to provide the test with 95% power to detect an overall 22% lower rate in the sacubitril-valsartan group (corresponding to a 30% lower risk of hospitalization for heart failure and a 10% lower risk of death from cardiovascular causes) and at least 80% power to detect an overall 19% lower rate (corresponding to a 25% lower risk of hospitalization for heart failure and a 10% lower risk of death from cardiovascular causes). A total of 4600 participants was estimated to be required over a 29-month period with a minimum follow-up of 26 months, based on an anticipated “time to first primary event” rate of 9 events per 100 patient-years. Analyses of primary and secondary endpoints were conducted according to the intention-to-treat principle.
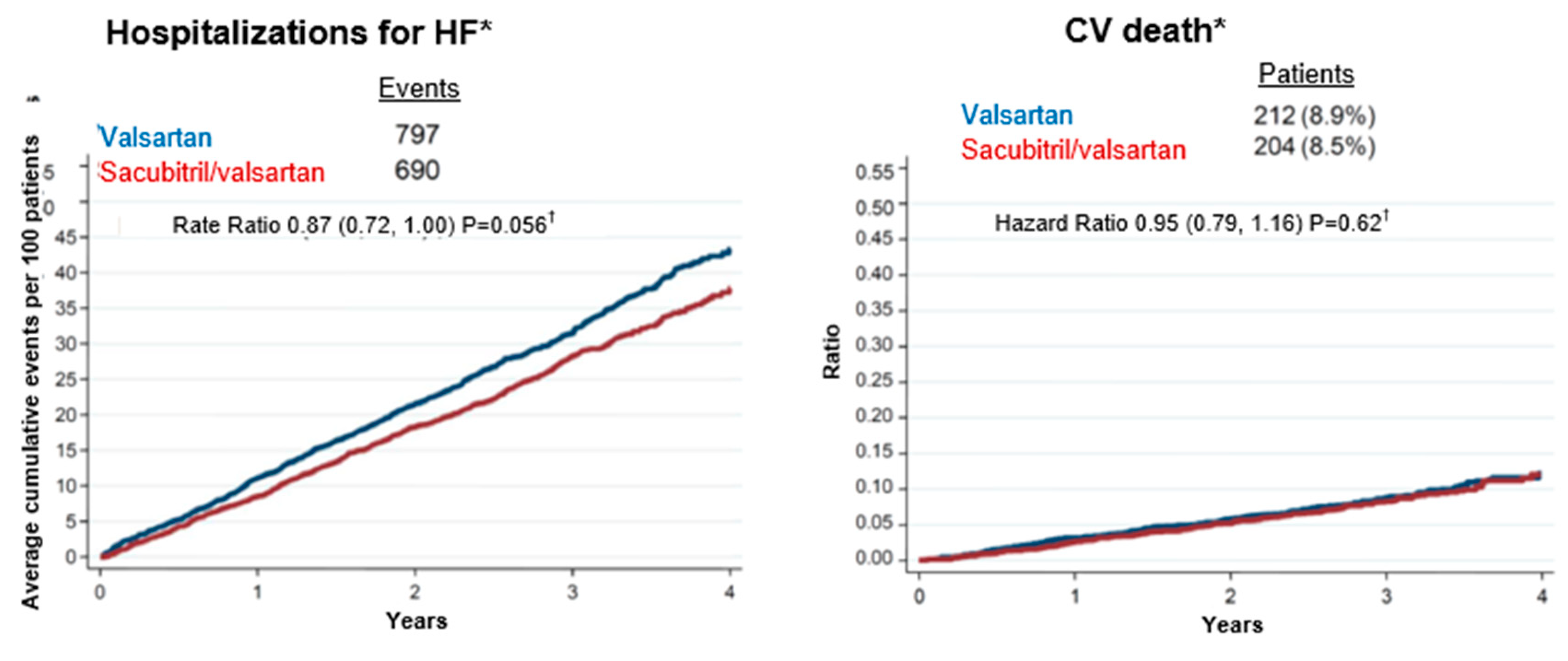
As a result, a total of 894 primary events were found in 526 patients in the sacubitril-valsartan group and 1009 primary events in 557 patients in the valsartan group (rate ratio, 0.87; 95% confidence interval [CI], 0.75 to 1.01; P = 0.06) (Figure 8). The incidence of death from cardiovascular causes was 8.5% in the sacubitril-valsartan group and 8.9% in the valsartan group (hazard ratio, 0.95; 95% CI, 0.79 to 1.16) (Figure 9); a total of 690 and 797 hospitalizations occurred due to heart failure, respectively (frequency ratio, 0.85; 95% CI, 0.72 to 1.00) (Figure 10).
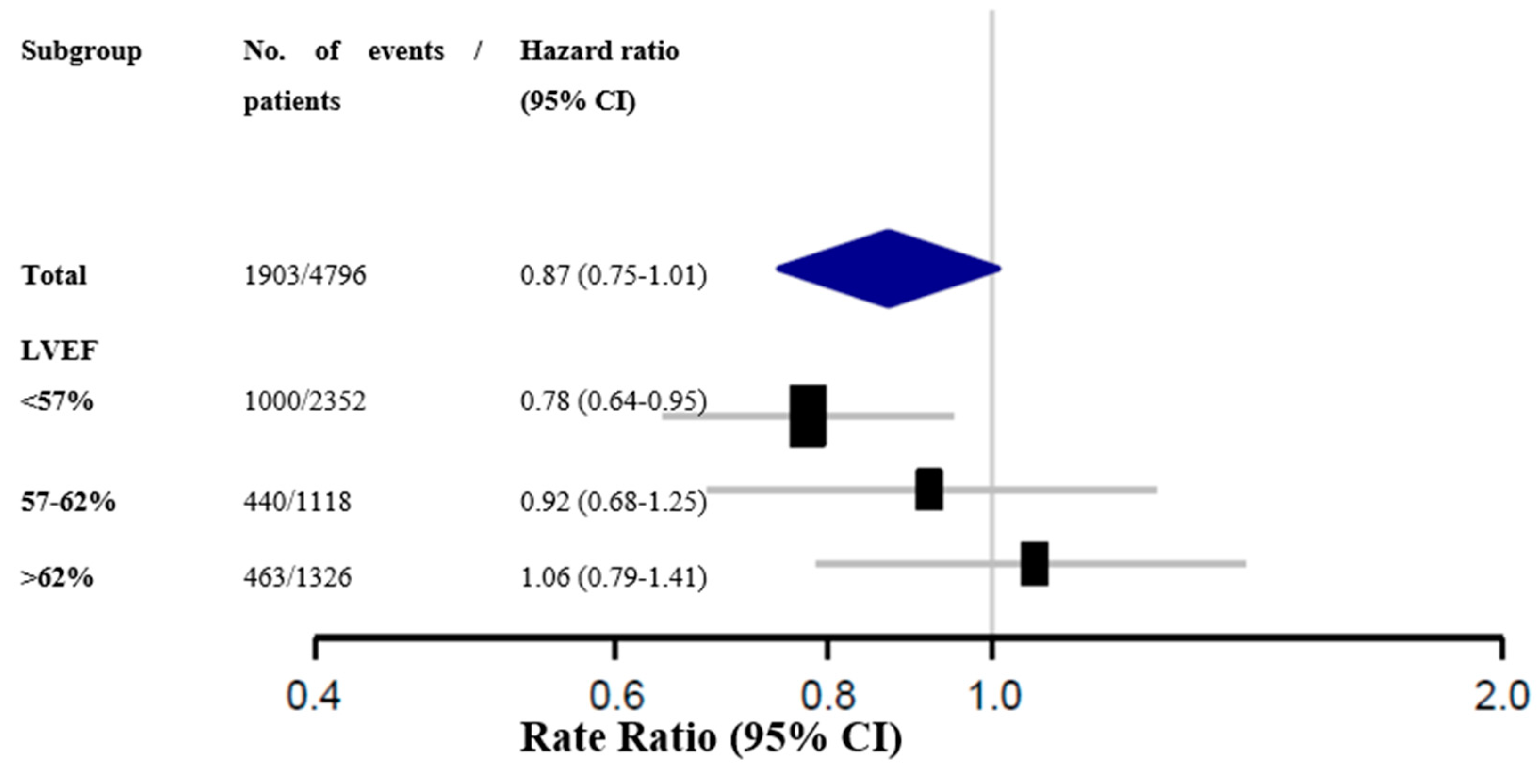
Regarding secondary endpoints (Figure 11), NYHA class improved in 15.0% of patients in the sacubitril-valsartan group and in 12.6% of those in the valsartan group (hazard ratio, 1.45; 95% CI, 1.13-1.86); renal function worsened by 1.4% and 2.7%, respectively (hazard ratio, 0.50; 95% CI, 0.33 to 0.77). Among 12 pre-specified subgroups, there was a suggestion of heterogeneity with possible benefit with sacubitril-valsartan in patients with lower ejection fraction and in females (Figure 12).
Of the 12 pre-specified subgroups, 2 showed possible heterogeneity in treatment effect, with a strong suggestion of benefit in patients with ejection fraction in the lower range (45 to 57%) (Figure 10) and in women, who represent a high proportion of patients with HFpEF and who were well represented in this study. The potential benefit of sacubitril-valsartan in patients with LVEF equal to or below the median has biological plausibility. Several post hoc analyses of previous trials12,13 have shown that other treatments that have been effective in patients with heart failure and low LVEF may also benefit patients with left ventricular ejection fraction ranging from 40 to 55%, populations that have subtle systolic dysfunction, with pathophysiological mechanisms also in populations that have preserved LVEF and are at increased risk of hospitalization for heart failure.
Figure 9.
Secondary endpoints. NYHA: New York Heart Association; KCCQ – Kansas City quality of life score. Adapted from Solomon S et al11.
Figure 9.
Secondary endpoints. NYHA: New York Heart Association; KCCQ – Kansas City quality of life score. Adapted from Solomon S et al11.
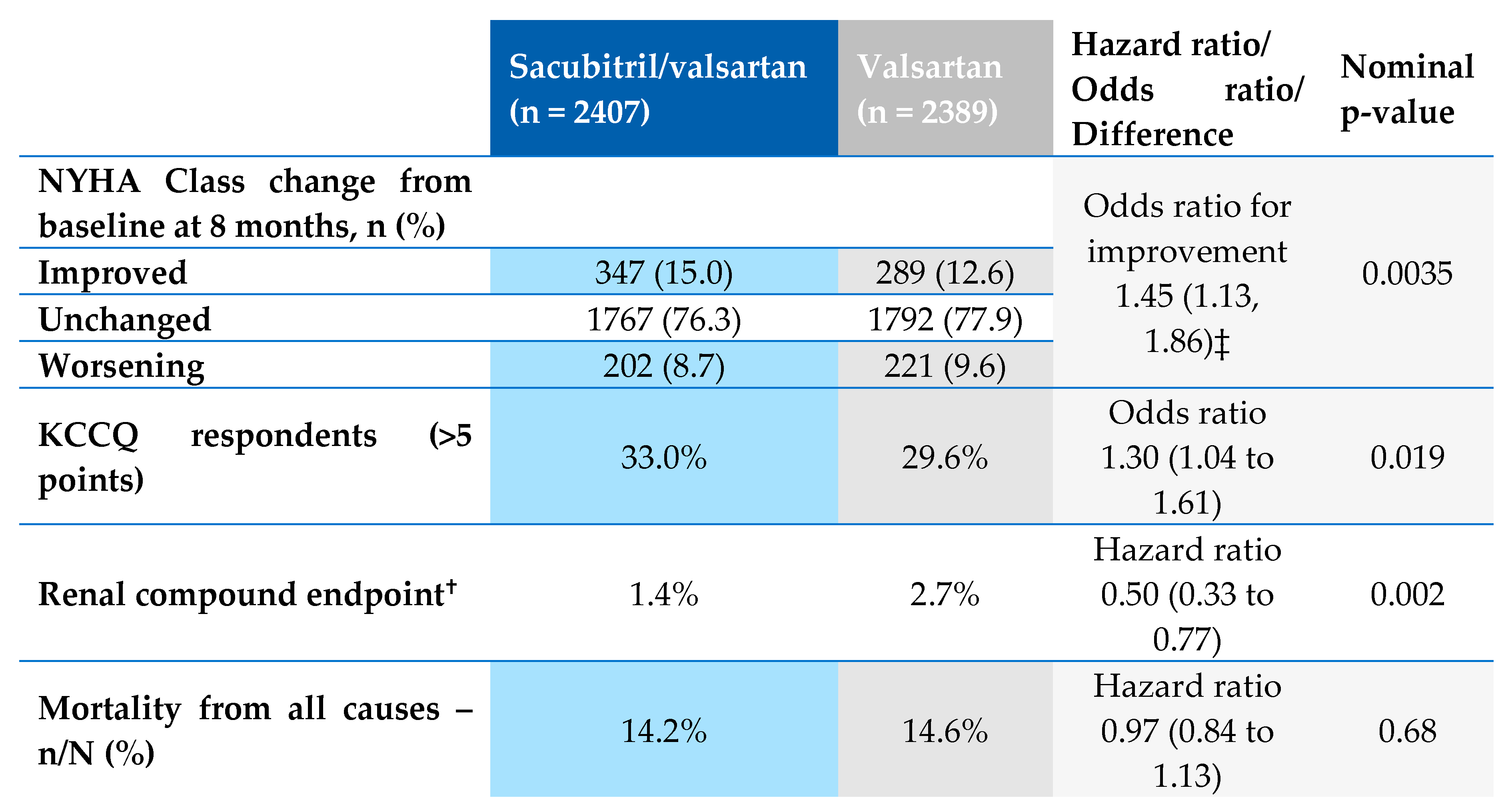
Figure 10.
Primary endpoint by pre-specified ejection fraction subgroups. LVEF: left ventricular ejection fraction. Adapted from Solomon S et al1.
Figure 10.
Primary endpoint by pre-specified ejection fraction subgroups. LVEF: left ventricular ejection fraction. Adapted from Solomon S et al1.
5. Conclusion
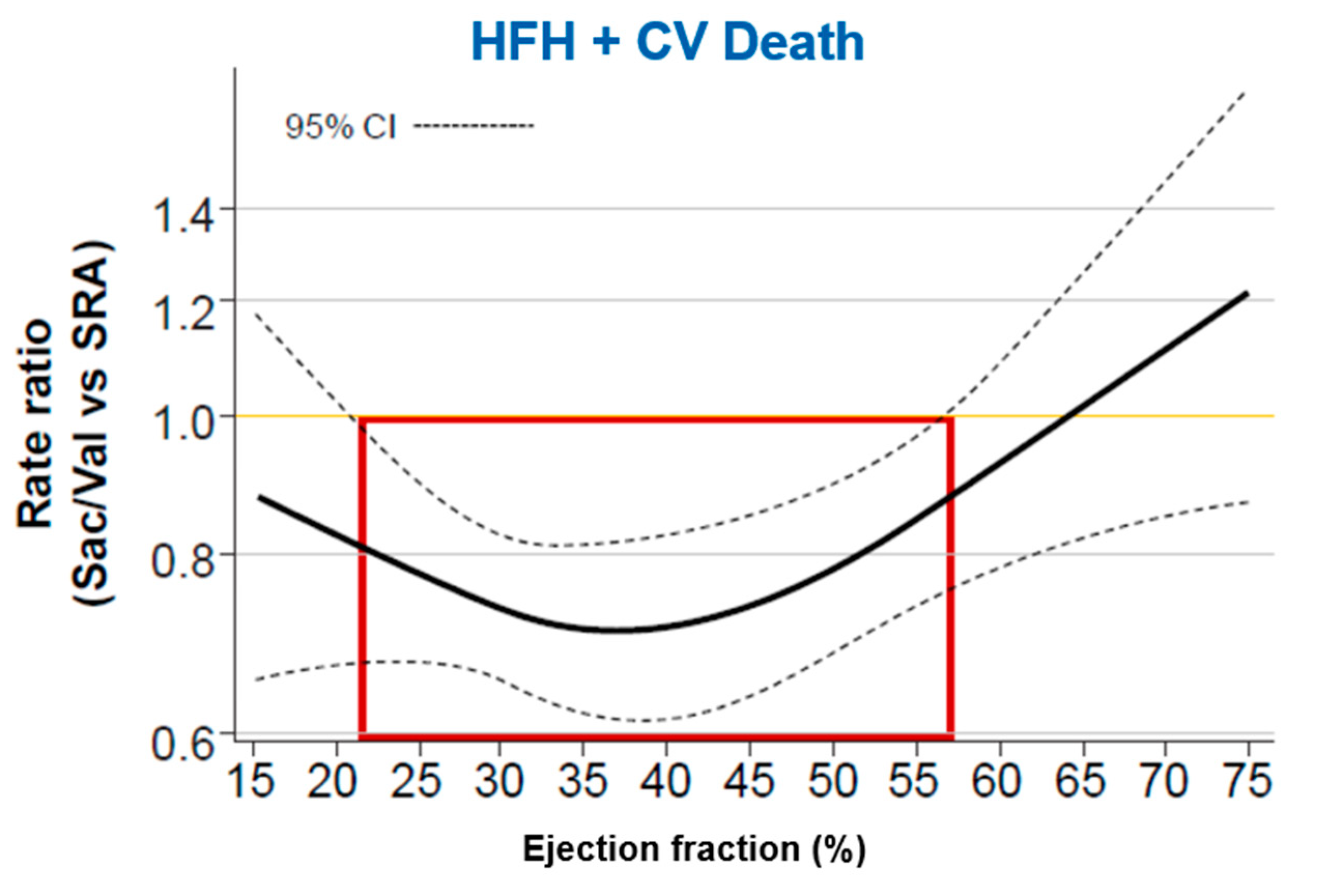
Therefore, results of the PARAGON-HF study point to a benefit in primary endpoints with mechanistic plausibility, that is, within a continuum of LVEF, from the favorable results in populations with lower rates of this index, already well proven in the PARADIGM-HF10 study, up to a cutoff point that can be considered LVEF below normal, whose contemporary classification1 defines as HFmrEF and HFpEF with LVEF≤57% (Figure 11)14
Figure 11.
Primary endpoints by pre-specified ejection fraction subgroups. Sac/Val: sacubitril-valsartan; SRA: valsartan; HFH: Heart failure hospitalizations. Adapted from Solomon S, et al 11,14.
Figure 11.
Primary endpoints by pre-specified ejection fraction subgroups. Sac/Val: sacubitril-valsartan; SRA: valsartan; HFH: Heart failure hospitalizations. Adapted from Solomon S, et al 11,14.
Considerations on the analysis of subgroups of the PARAGON HF study
The analysis of subgroups of the PARAGON-HF study includes several epidemiological and biostatistical characteristics necessary for an adequate interpretation of the data: 1) The analysis was pre-specified (not post hoc); 2) It included a large number of participants and events; 3) It used an interaction test adjusted for multiplicity (a multivariate analysis); 4) It evaluated the architecture of the total data and adjacent subgroups (internal consistency); 5. Results were interpreted in the context of similar data from other clinical trials (external validation); 6. It presents biological coherence and plausibility.
Final conclusions about Sacubitril-valsartan for HF treatment with below normal LVEF
Considering the following arguments:
- -
- HFpEF and HFmrEF are highly prevalent syndromes, causing disabling symptoms and frequent hospitalizations in the elderly, many of whom are females, and for whom there is no approved treatment;A well-designed study with the largest number of participants to date published for this population showed statistically significant results in reducing renal endpoints, improvement of performance status and it was safe;
- -
- In a pre-specified subgroup analysis of the PARAGON-HF study, sacubitril-valsartan showed benefit in the combined primary endpoint in patients with LVEF equal to or less than the 57% median;
- -
- Additional data shows that other drugs act on neurohumoral pathways also seem to be beneficial in patients with HF and lower rates of LVEF in the HFpEF setting, i.e, below the normal;
- -
- The update of the Brazilian Guidelines on HF 2021 already recommends the use of sacubitril-valsartan for patients with HFmrEF;
- -
- The US Food and Drug Administration (FDA) has recently approved sacubitril-valsartan as below normal ejection fraction HF treatment;
Therefore, it is coherent to consider sacubitril-valsartan as an effective, safe and available pharmacological treatment for the treatment of HFmrEF and HFpEF with a range of LVEF≤57%.
Declaration of interest
The authors declare no conflicts of interest. LCD is employed of Universidade Luterana do Brasil and declare no conflicts of interest. NT is employees of Novartis declare no conflicts of interest. FJF and RFC were employees of Novartis during the writing of manuscript and declare no conflicts of interest.
References
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail 2021, 23, 352–380. [Google Scholar] [PubMed]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; et al. 2016–2018 EACVI Scientific Documents Committee. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2017, 18, 1301–1310. [Google Scholar] [PubMed]
- Paulus, W.J.; Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Jorge, A.L.; Rosa, M.L.; Martins, W.A.; Correia, D.M.; Fernandes, L.C.; Costa, J.A.; Moscavitch, S.D.; Jorge, B.A.; Mesquita, E.T. The Prevalence of Stages of Heart Failure in Primary Care: A Population-Based Study. J Card Fail. 2016, 22, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Petersen, L.C.; Danzmann, L.C.; Bartholomay, E.; Bodanese, L.C.; Donay, B.G.; Magedanz, E.H.; Azevedo, A.V.; Porciuncula, G.F.; Miglioranza, M.H. Survival of Patients with Acute Heart Failure and Mid-range Ejection Fraction in a Developing Country - A Cohort Study in South Brazil. Arq Bras Cardiol. 2021, 116, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Marcondes-Braga, F.G.; Moura, L.A.Z.; Issa, V.S.; et al. Emerging Topics Update of the Brazilian Heart Failure Guideline - 2021. Arq Bras Cardiol. 2021, 116, 1174–1212. [Google Scholar] [PubMed]
- Diretriz Brasileira da Insuficiência Cardíaca Crônica e Aguda. Arq Bras Cardiol. 2018;Arquivos Brasileiros de Cardiologia. 2018, 111, 436–539.
- Solomon, S.D.; Zile, M.; Pieske, B.; et al. Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion (PARAMOUNT) Investigators. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: A phase 2 double-blind randomised controlled trial. Lancet. 2012, 380, 1387–1395. [Google Scholar] [PubMed]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl JMed 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; et al. PARAGON-HF Investigators and Committees. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N Engl J Med. 2019, 381, 1609–1620. [Google Scholar] [PubMed]
- Solomon, S.D.; Claggett, B.; Lewis, E.F.; et al. Influence of ejection fraction on outcomes and efficacy of spironolactone in patients with heart failure with preserved ejection fraction. Eur Heart J 2016, 37, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Claggett, B.; Liu, J.; et al. Heart failure with mid-range ejection fraction in CHARM: Characteristics, outcomes and effect of candesartan across the entire ejection fraction spectrum. Eur J Heart Fail 2018, 20, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Vaduganathan, M.; LClaggett, B.; Packer, M.; Zile, M.; Swedberg, K.; Rouleau, J.; APfeffer, M.; Desai, A.; Lund, L.H.; Kober, L.; Anand, I.; Sweitzer, N.; Linssen, G.; Merkely, B.; Luis Arango, J.; Vinereanu, D.; Chen, C.H.; Senni, M.; Sibulo, A.; Boytsov, S.; Shi, V.; Rizkala, A.; Lefkowitz, M.; McMurray, J.J.V. Sacubitril/Valsartan Across the Spectrum of Ejection Fraction in Heart Failure. Circulation. 2020, 141, 352–361. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pathophysiology of heart failure according to left ventricular ejection fraction.
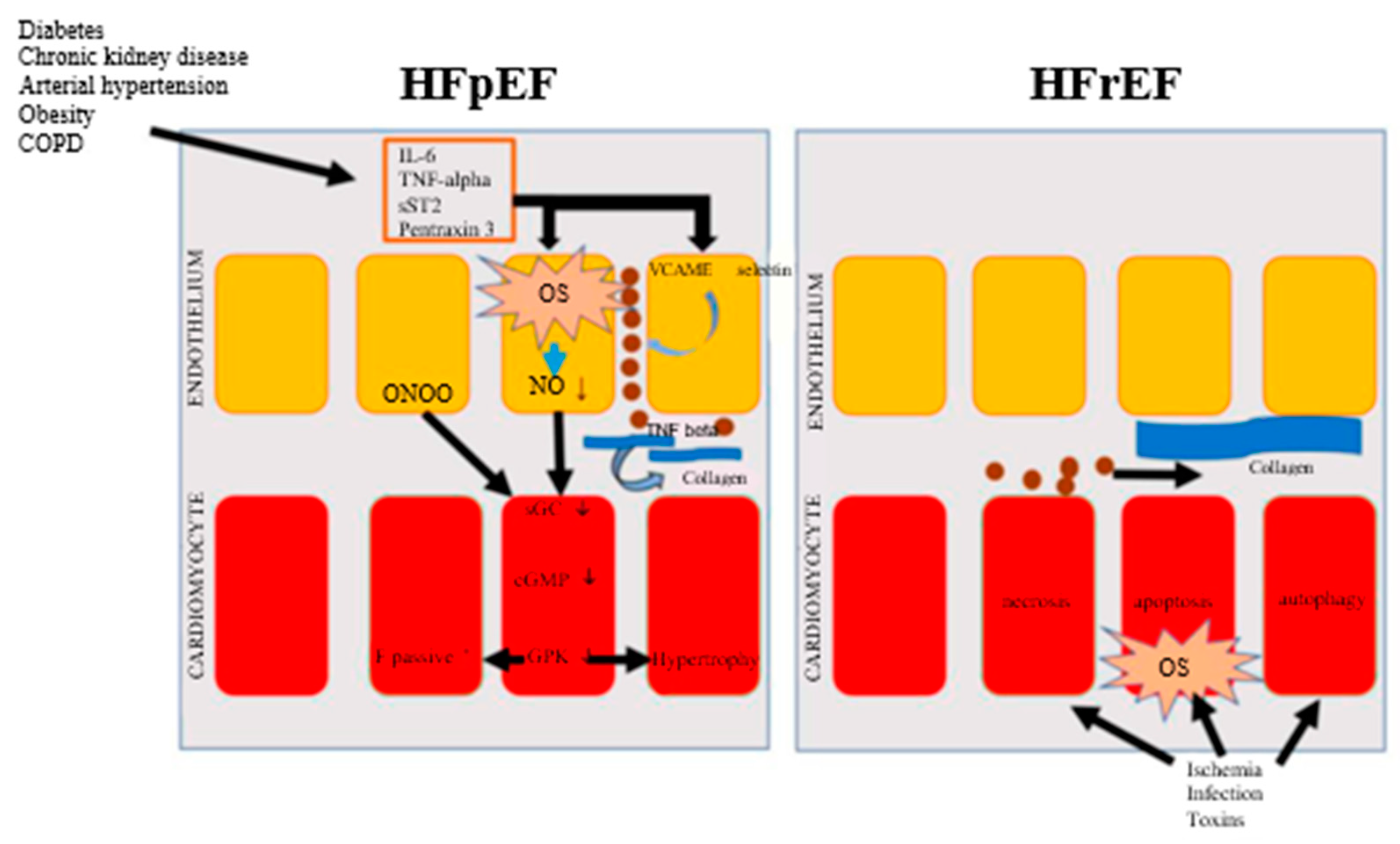
Figure 2.
Prevalence of HF stages and its phenotypes at primary care in the city of Niteroi-RJ. Adapted from Jorge AL et al4.
Figure 2.
Prevalence of HF stages and its phenotypes at primary care in the city of Niteroi-RJ. Adapted from Jorge AL et al4.
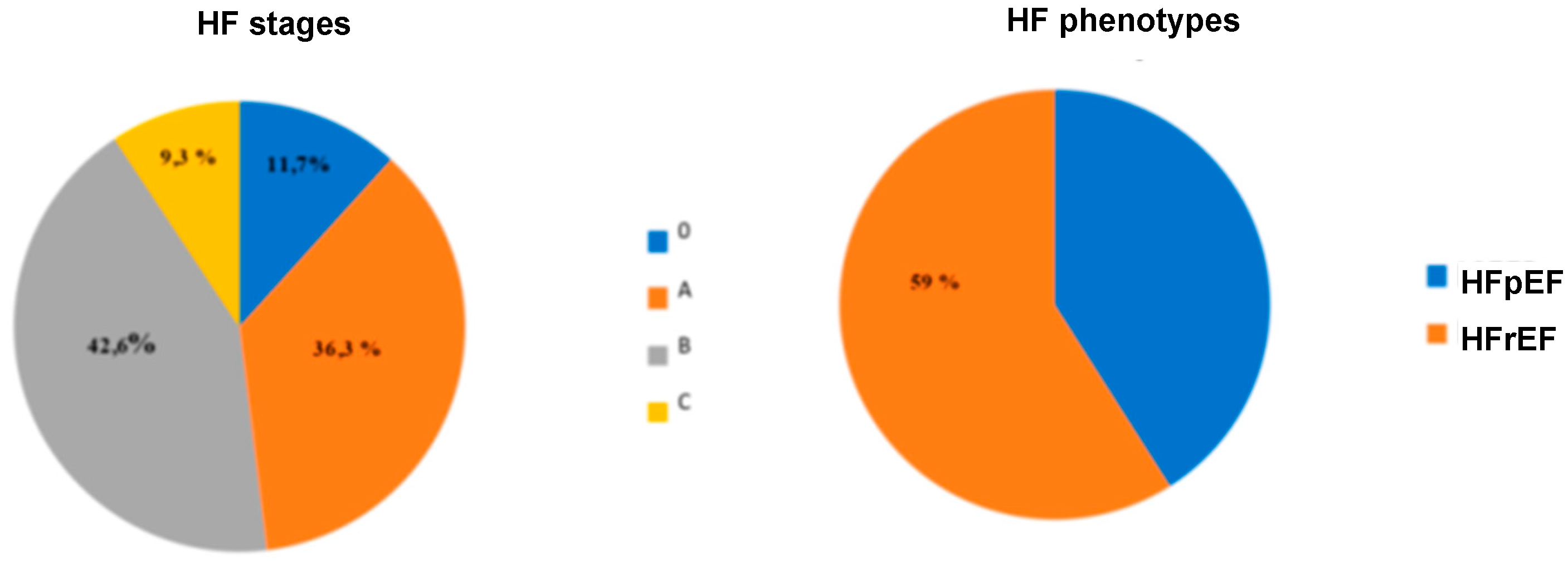
Figure 3.
Overall survival curve. HFrEF: heart failure with reduced ejection fraction; HFiEF: heart failure with intermediate ejection fraction; HFpEF: heart failure with preserved ejection fraction.
Figure 3.
Overall survival curve. HFrEF: heart failure with reduced ejection fraction; HFiEF: heart failure with intermediate ejection fraction; HFpEF: heart failure with preserved ejection fraction.
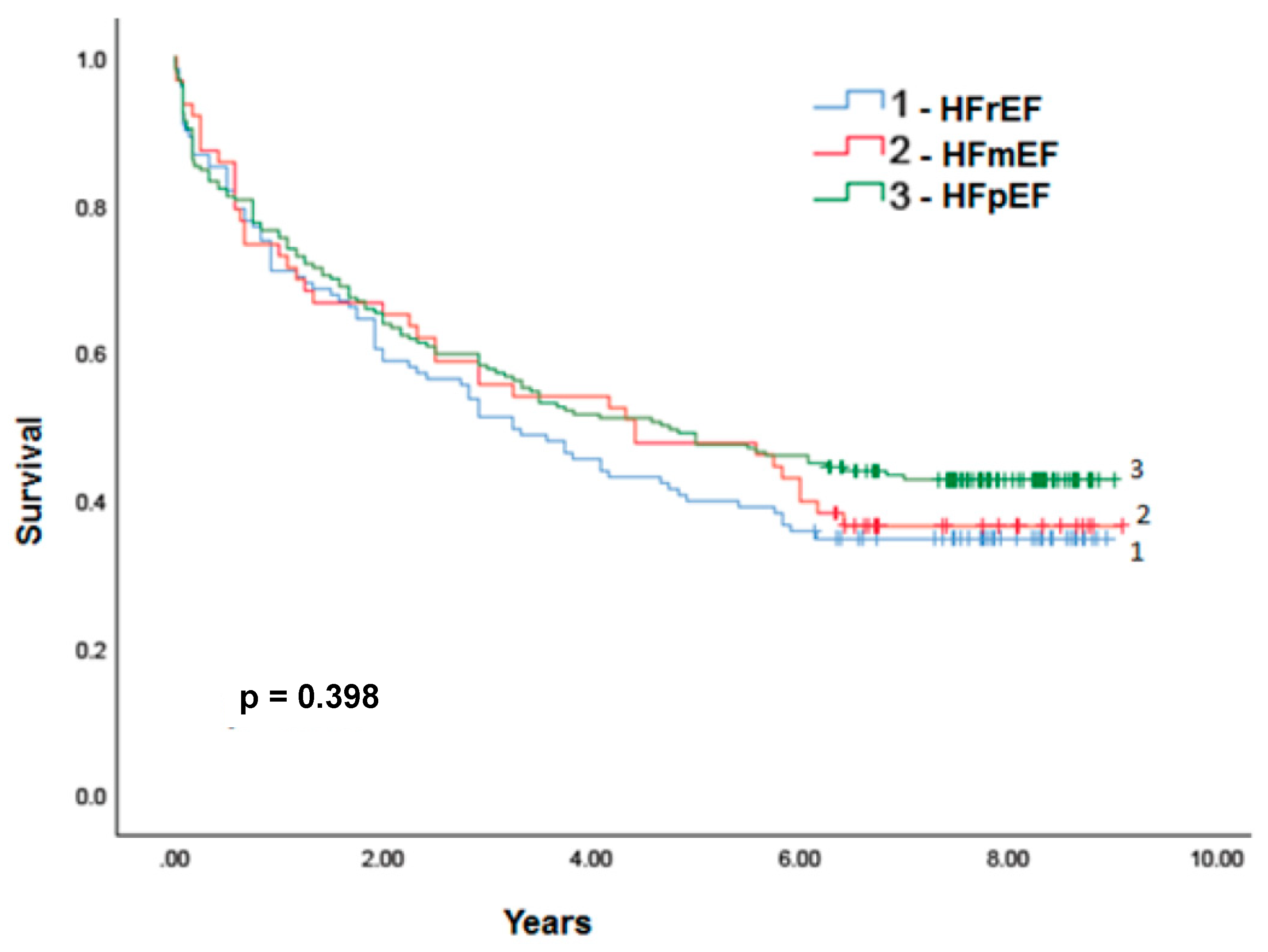
Figure 4.
Survival curve for cardiovascular diseases, HFrEF: heart failure with reduced ejection fraction; HFiEF: heart failure with intermediate ejection fraction; HFpEF: heart failure with preserved ejection fraction.
Figure 4.
Survival curve for cardiovascular diseases, HFrEF: heart failure with reduced ejection fraction; HFiEF: heart failure with intermediate ejection fraction; HFpEF: heart failure with preserved ejection fraction.
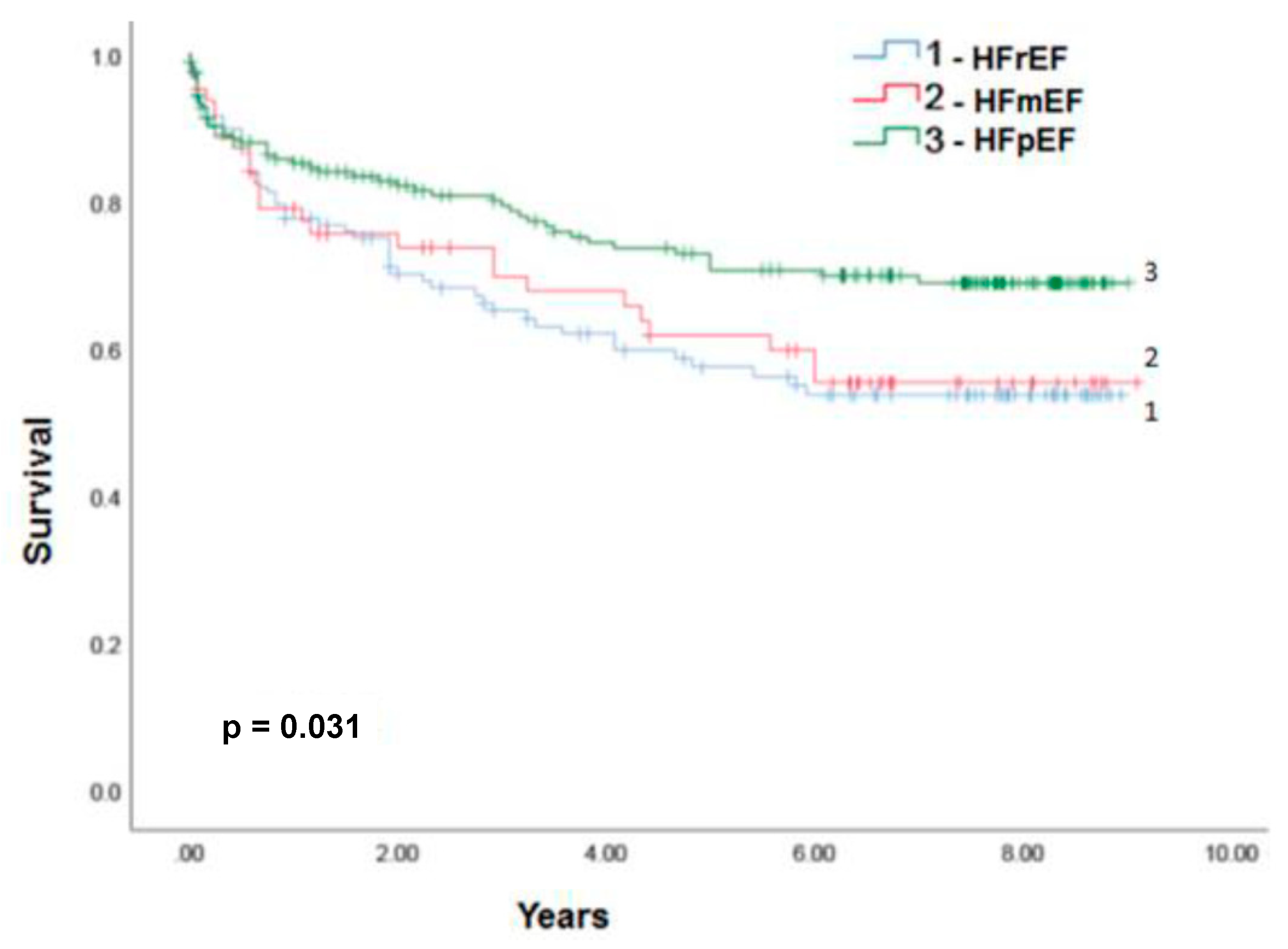
Figure 5.
Reduced ejection fraction heart failure treatment algorithm ARB: angiotensin II receptor blockers; LBB: left bundle branch block; ICD: implantable cardioverter defibrillator; LVEF: left ventricular ejection fraction; H-N: combination of hydralazine and nitrate; HF: heart failure; ACEi: angiotensin converting enzyme inhibitors; ARNi: angiotensin receptor neprilysin inhibitor; SGLT2i: sodium and glucose cotransporter inhibitors 2; NYHA: New York Heart Association; CRT: cardiac resynchronization therapy. Adapted from Marcondes-Braga et al.
Figure 5.
Reduced ejection fraction heart failure treatment algorithm ARB: angiotensin II receptor blockers; LBB: left bundle branch block; ICD: implantable cardioverter defibrillator; LVEF: left ventricular ejection fraction; H-N: combination of hydralazine and nitrate; HF: heart failure; ACEi: angiotensin converting enzyme inhibitors; ARNi: angiotensin receptor neprilysin inhibitor; SGLT2i: sodium and glucose cotransporter inhibitors 2; NYHA: New York Heart Association; CRT: cardiac resynchronization therapy. Adapted from Marcondes-Braga et al.
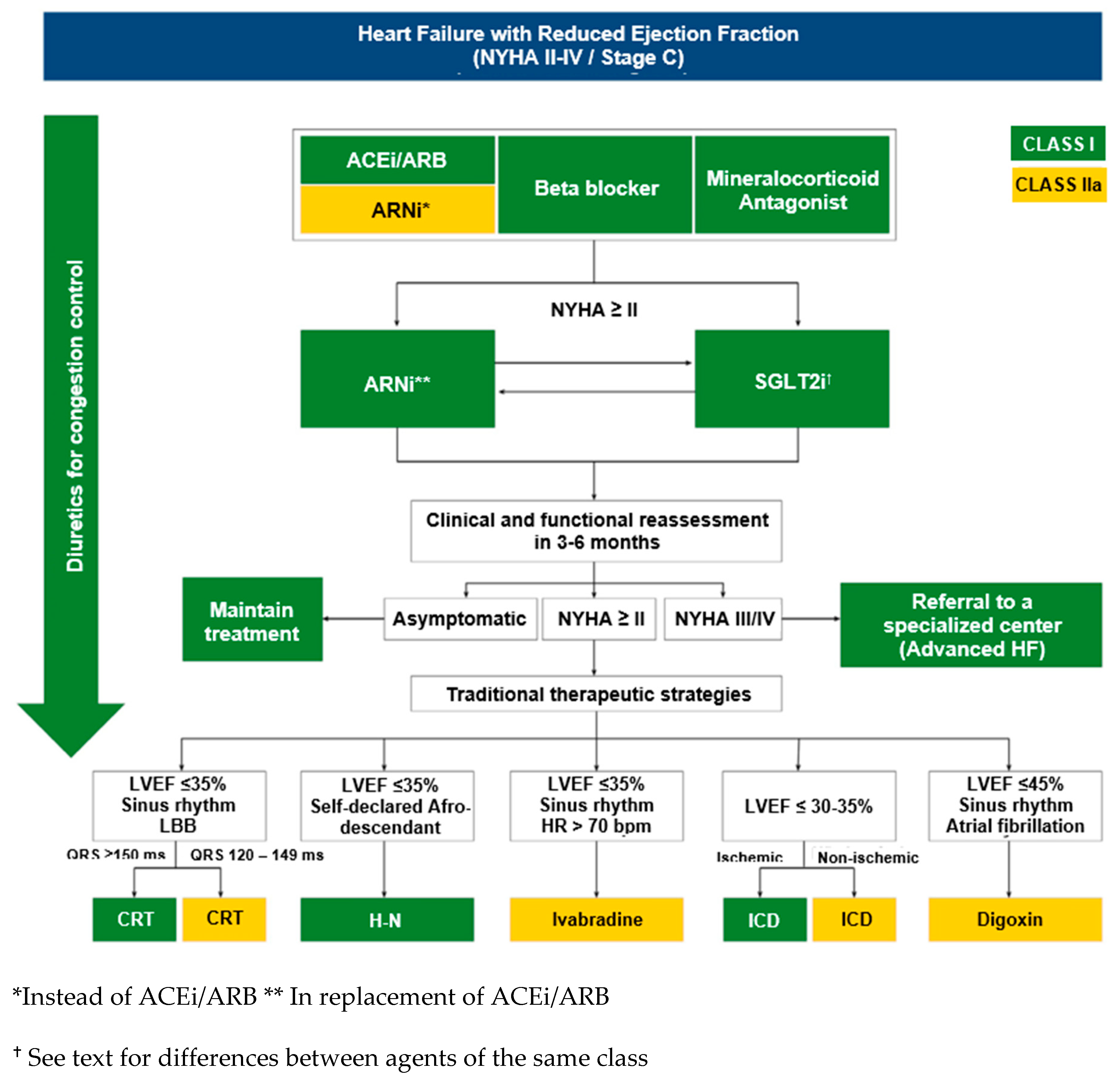
Figure 6.
NT-proBNP in 4, 12 and 36 weeks in the LCZ696 and Valsartan groups.
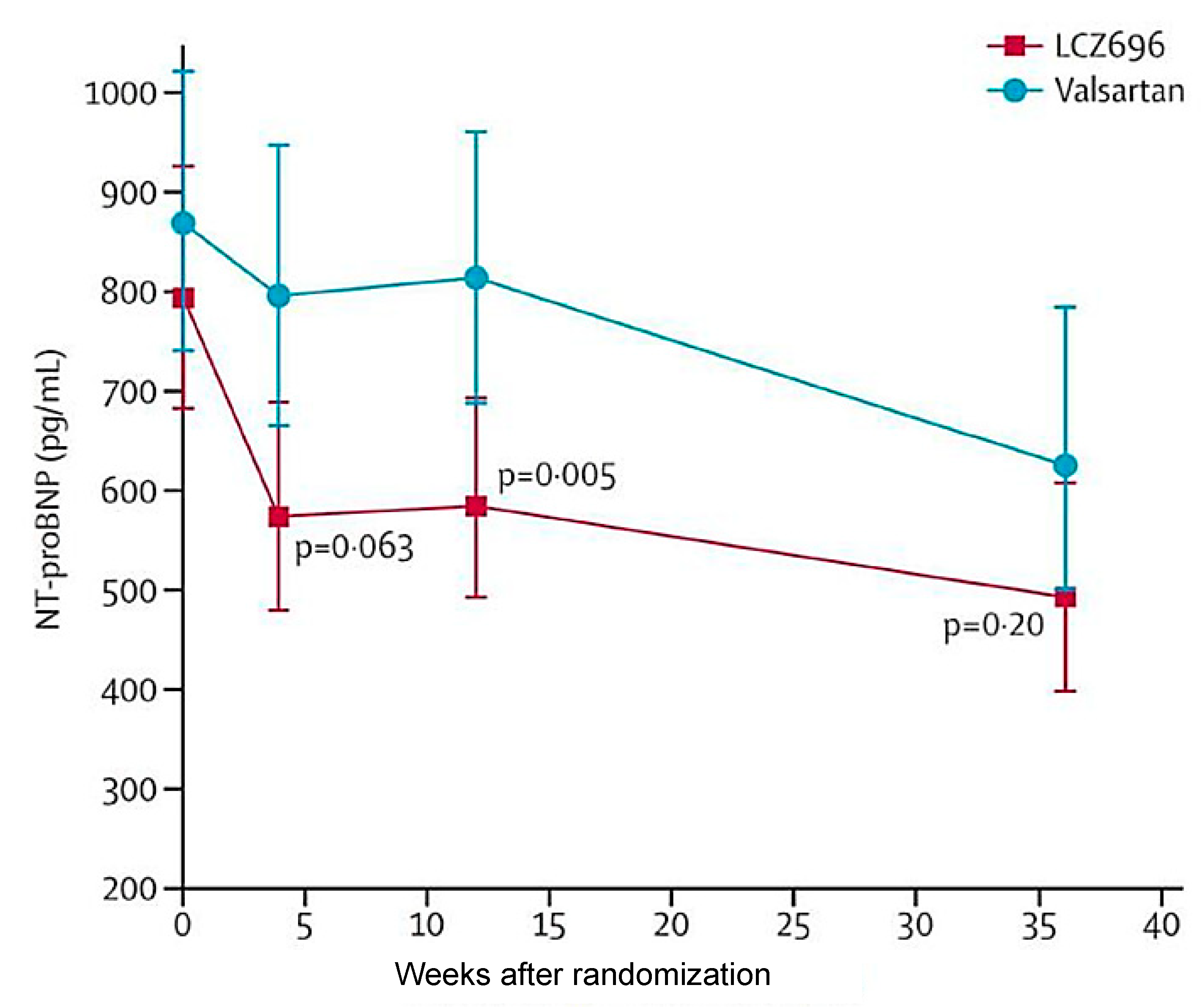
Figure 7.
PARAGON HF study design. BID: twice daily, run-in: initial enrollment; Sac-val: sacubitril-valsartan. Adapted from Solomon S et al11.
Figure 7.
PARAGON HF study design. BID: twice daily, run-in: initial enrollment; Sac-val: sacubitril-valsartan. Adapted from Solomon S et al11.
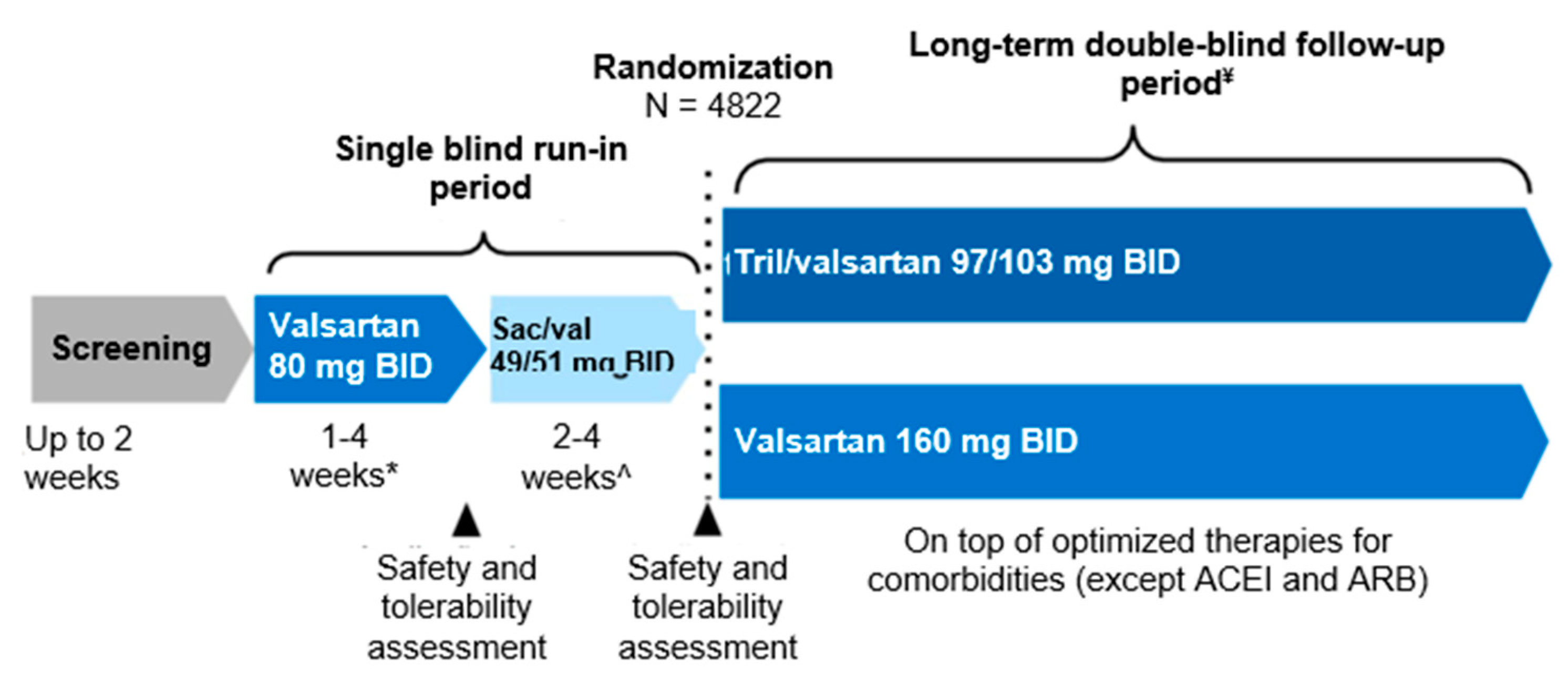
Figure 8.
Primary endpoint of cardiovascular mortality/hospitalizations. Adapted from Solomon S et al11.
Figure 8.
Primary endpoint of cardiovascular mortality/hospitalizations. Adapted from Solomon S et al11.
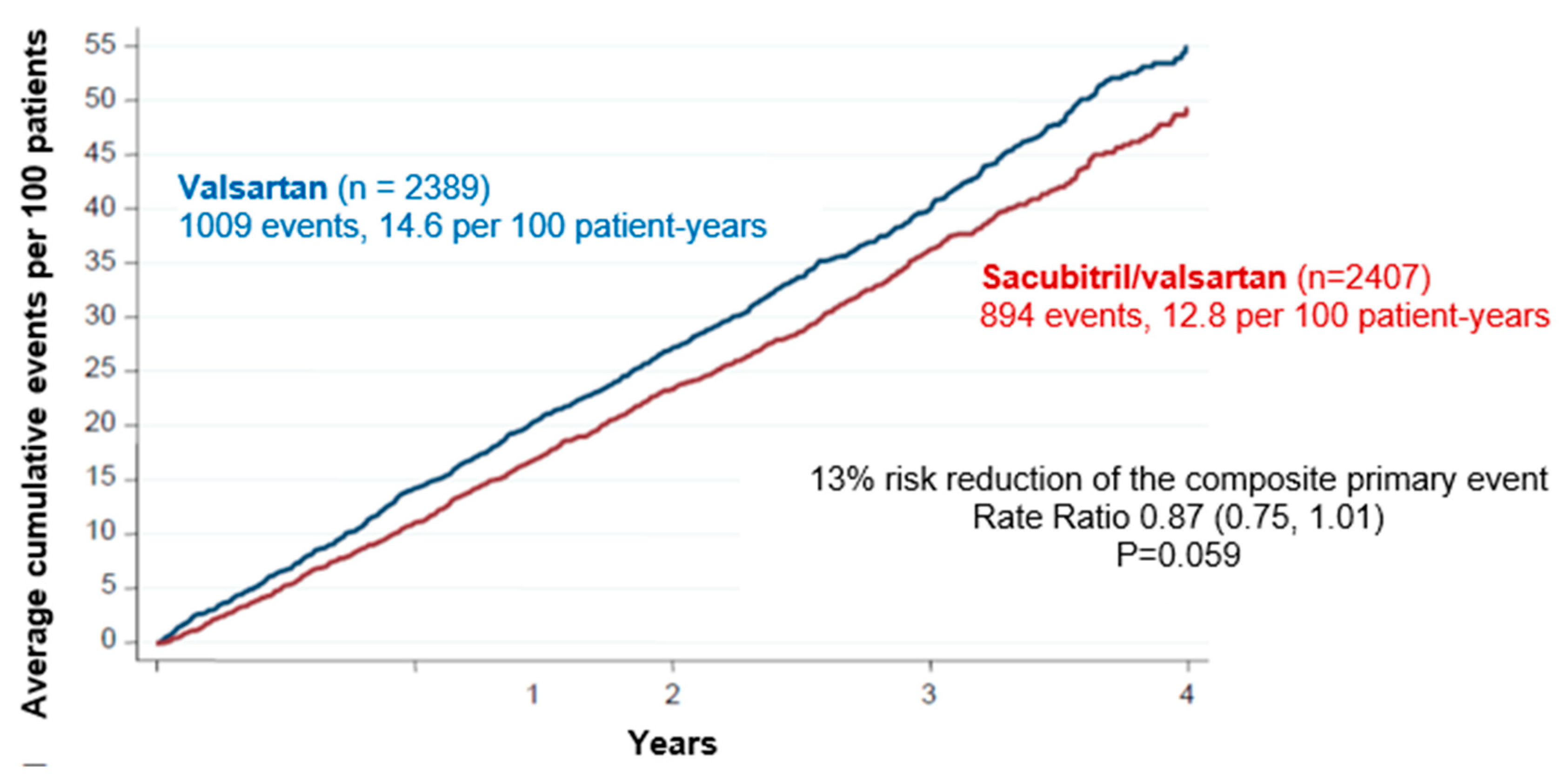
Figure 9.
Primary endpoint divided into cardiovascular mortality and hospitalizations. HF: heart failure; CV: cardiovascular. Adapted from Solomon S et al11.
Figure 9.
Primary endpoint divided into cardiovascular mortality and hospitalizations. HF: heart failure; CV: cardiovascular. Adapted from Solomon S et al11.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



