Submitted:
14 June 2023
Posted:
14 June 2023
You are already at the latest version
Abstract
Acute vertigo and dizziness are frequent presenting symptoms in patients on the emergency department. With a broad differential diagnosis and symptoms/signs often subtle and transient, the diagnostic approach to the dizzy patient remains challenging. Previous work emphasized the value of combining structured history-taking and a targeted examination focusing on subtle oculomotor signs. Here I review different bedside algorithms proposed for the acutely dizzy patient. Comparing area-under-the-curve ROC-characteristics and sensitivity/specificity, highest diagnostic accuracy was observed for algorithms focusing on subtle oculomotor signs. Both the HINTS+ bedside-exam and the STANDING algorithm have demonstrated higher diagnostic accuracy for identifying strokes than early (<24-48h after symptom-onset) MRI-DWI. Importantly, HINTS and STANDING require moderate training to allow reliable application. Thus, for physicians lacking dedicated training, other approaches are needed. Various scores that rely on vascular risk-factors, clinical symptoms and focal neurologic findings have been proposed (e.g., ABCD2-score, PCI-score, TriAGe+-score). While these scores are more readily applicable for frontline providers, they provide intermediate diagnostic accuracy at best and often lack external validation, thus are an insufficient substitute for algorithms assessing subtle oculomotor findings. Providing dedicated training in HINTS+ or STANDING techniques will be key to improve the diagnostic accuracy and to avoid unnecessary brain imaging.
Keywords:
Vertigo
; dizziness
; bedside testing
; HINTS
; STANDING
; truncal ataxia
1. Introduction
A chief complaint of acute vertigo or dizziness is related to about 2.1 to 7.1% of all emergency department (ED) consultations [1,2,3,4], with an increase of the number of ED-visits with a chief-complaint of dizziness between 1995 and 2009 by 90% [5]. This results in about 4.3 million consults in the USA per year as estimated in 2012 [6,7]. With the differential diagnosis of patients presenting with acute or episodic vertigo / dizziness being very broad and cutting across all specialties, frontline providers and specialists may be overwhelmed with this leading symptom. In patients presenting to the ED with vestibular symptoms, life-threatening conditions have been identified in a single study in 23.8% of visits, with 12.5% of all visits related to cerebrovascular events [2]. This emphasizes the need to distinguish between dangerous central and benign, self-limited peripheral vestibular disorders to avoid misdiagnosis. Overall, roughly 9% of cerebrovascular events are missed at the initial ED presentation and risk of misdiagnosis is much greater when presenting neurologic complaints are mild, nonspecific, or transient (range 24%–60%) [8]. For posterior circulation strokes presenting with dizziness frontline misdiagnosis appears common, occurring in roughly 35% of cases [9]. In patients presenting with acute prolonged vertigo or dizziness meeting diagnostic criteria for an acute vestibular syndrome or AVS (i.e., a clinical syndrome of acute-onset, continuous vertigo, dizziness, or unsteadiness lasting days to weeks, generally including features suggestive of new, ongoing vestibular system dysfunction [e.g., vomiting, nystagmus, severe postural instability] [10]), about 25% ± 15% will eventually receive a diagnosis of an underlying vertebrobasilar ischemic stroke [11]. This may trigger unnecessary diagnostic testing including brain imaging (computed tomography (CT) and magnetic resonance imaging including diffusion-weighted imaging (MRI-DWI)), laboratory workup or electrocardiography. Not surprisingly, annual costs in the USA related to the diagnosis and treatment of dizzy patients in the ED have been estimated to exceed 4 billion USD in 2013 and are expected to rise further [6,7]. One of the main reasons for growing costs identified is the increasing use of imaging and further diagnostic testing [7]. Specifically, the utilization of CT and MRI increased by 169% from 1995 to 2004, which was more than any other test [1]. Large fractions of acutely dizzy patients received CT-scans (17% (1995 – 2004) [12] and 48% (2008-2011) [13]), a clinically significant pathology leading to a CNS diagnosis (6%) [12] or even requiring an intervention (0.74%) [13], however, was the exception. Thus, the predictive value for significant pathology of CT brain / head in acutely dizzy patients was low [13], and visits with a CT scan were associated with an increased ED length of stay compared to visits without a CT scan [12]. Even MRI including DWI in AVS has limited sensitivity, missing about 1 out of 5 vertebrobasilar strokes when obtained within the first 24-48 hours after symptom onset [14]. This false-negative rate may rise to up to 50% for small lacunar brainstem strokes [15].
At the same time, the evidence base for effective bedside differentiation of inner ear diseases from stroke in patients with acute dizziness and vertigo has grown substantially over time [16,17], as emphasized recently [14]. Noteworthy, relying on any obvious focal neurologic signs has a sensitivity of 44% for detecting a central cause of AVS only, i.e., more than 50% of strokes will be missed when relying on this approach solely [14]. Thus, different clinical signs pointing to a central cause in AVS patients have been proposed, emphasizing the combined use of targeted neuro-otologic bedside examination techniques, such as the HINTS (Head Impulse, Nystagmus, Test of Skew) [18], HINTS+ (which adds a bedside test of hearing) [19], STANDING [20] or assessing for gait/truncal instability [21]. This critical review provides an overview of diagnostic algorithms previously proposed for the differential diagnosis in the AVS patient, discussing advantages and limitations of specific tests.
2. Bedside Examination Tools in AVS
For the bedside examination of the patient meeting the diagnostic criteria for an AVS, a broad range of clinical scores has been proposed. These scores take into account a combination of different features including the patient’s history (e.g., symptom presentation, cardiovascular risk factors), findings from the clinical neurologic examination, findings from a dedicated oculomotor examination and biomarkers. The ABCD2 score, for example, relies on patient history and neurologic examination only [19,22,23], whereas the HINTS [18] and the STANDING [20] score focus on findings retrieved from a dedicated oculomotor examination. Yet other scores combine the patient history, neurologic and oculomotor examination, as e.g. the TriAGe+ score [24]. In the following, I will review various scores (see Table 1), critically discussing their validity and value in the diagnostic approach to the acutely dizzy patient.
2.1. HINTS/HINTS Plus
A targeted bedside examination using three subtle oculomotor findings has been found to identify central causes (mostly ischemic strokes) in AVS patients [18]. Specifically, presence of one (or more) central signs in the HINTS (Head-impulse, nystagmus, test of skew) testing battery, which consisted of a bedside assessment of the horizontal angular vestibulo-ocular reflex (aVOR) by applying the head-impulse test (HIT) [25], evaluating ocular stability at eccentric gaze (looking for a gaze-evoked nystagmus) and testing for a vertical divergence in the alternating cover test was associated with a 100% sensitivity and 96% specificity for detecting a stroke. Central signs pointing to an INFARCT were defined as a normal head-impulse test, presence of gaze-evoked nystagmus on lateral gaze or presence of a skew deviation [18]. Importantly, presence of one out of these three signs was sufficient to suspect a central cause. The HINTS paradigm became increasingly popular since its introduction in 2009 and is now considered the standard bedside examination technique in AVS patients on the ED, as summarized in the very recent GRACE3-guideline on acute vertigo and dizziness in the ED [26]. In a recent systematic review of the literature (1980 - 2022) focusing on high-quality (level of evidence 1 to 3) studies reporting on the diagnostic accuracy of bedside eye movement testing in acutely dizzy patients, ten studies investigating the diagnostic accuracy of bedside HINTS were included (representing data from 422 patients with a central AVS and 378 patients with a peripheral AVS). In this meta-analysis, a high sensitivity (95.3% [95% confidence interval (CI) = 92.5 - 98.1%]) and specificity (92.6% [88.6 - 96.5%]) for the HINTS bedside exam was found [14]. When adding a fourth sign (unilateral, new onset hearing loss) to the HINTS battery (called HINTS-plus [19]), sensitivity increased further (97.2% [94.0 – 100.0%]) compared to the HINTS (by 1.9%). However, the sample size of patients was smaller for the HINTS+ battery (central AVS=276, peripheral AVS=252). Importantly, both subspecialists (i.e., neuro-otologists / neuro-ophthalmologists) and non-subspecialists (i.e., general neurologists, neurology residents, emergency physicians) demonstrated a high accuracy when using either the HINTS or the HINTS+ exam. Noteworthy, the sensitivity of the HINTS exam was comparable amongst these two groups (94.3% vs 95.0%, p = 0.55), although specificity of the HINTS exam was higher in the subspecialist group than in the non-subspecialist group (97.6% vs 89.1%, p = 0.007), indicating potential differences in the interpretation of test results [14]. Another study, which fell outside of the inclusion criteria for this recent meta-analysis also suggested that trained ED clinicians can accurately perform and interpret the horizontal HIT and nystagmus testing [27].
2.2. Standing
The STANDING algorithm (i.e., a four-step algorithm including 1) the discrimination between SponTaneous and positional nystagmus, (2) the evaluation of the Nystagmus Direction, (3) the head Impulse test, and (4) the evaluation of equilibrium (staNdinG)) was designed to be more inclusive. Specifically, it allows to diagnose patients with positional nystagmus as well (by applying provocation maneuver for the posterior and lateral canals), and examined truncal ataxia also [20,27]. However, this algorithm was more selective in applying single bedside tests based on initial findings (e.g., a head-impulse test was applied only in patients with unilateral spontaneous nystagmus). Likewise, the grading of truncal ataxia was less granular than proposed by others [21]. Specifically, an inability to stand or walk was considered indicative for a central origin (approximately reflecting grade 2 or grade 3 truncal instability (for details see dedicated section on gait and truncal instability further below).
Three prospective studies with relatively unselected patient cohorts have been published. When first proposed, the inventors of the STANDING algorithm reported a high overall diagnostic accuracy (sensitivity=95% [83 – 99%]; specificity=87% [85 – 87%] in a cohort of 352 patients with acute vertigo/unsteadiness [27]. In a more recent, prospective study with 300 patients with isolated vertigo and unsteadiness, the specificity of the STANDING algorithm was lower (75% vs. 87%), whereas the sensitivity (94% vs. 95%) was similar compared with the prior validation study [23]. In a follow-up prospective study, the same group investigated the diagnostic accuracy of the STANDING algorithm performed by ED physicians (both interns and senior emergency physicians) that had received 4 hours of training (lectures and practical demonstrations) [28]. Specifically, the STANDING algorithm demonstrated sensitivities of 84.8% (75.6 – 93.9%) and 89.8% (82.1 – 97.5%) in the interns and the senior emergency physicians, respectively. Likewise, the specificity reached 88.9% (85.1 – 92.8%) and 91.3% (87.8 – 94.8%) in both groups.
Overall, these prospective studies confirm that the STANDING algorithm is very valuable in the ED setting, with a diagnostic accuracy similar than when using the HINTS, but applicable to a larger proportion of dizzy patients (including cases with positional or episodic symptoms only). A potential limitation is the relatively small number of studies published, with two of the three studies available coming from the same laboratory.
2.3. TriAGe+ Score and PCI-Score
For the TriAGe+ score, information retrieved by taking the patient’s history (asking for triggers and the type of dizziness), by assessing the presence / absence of vascular risk factors and from the bedside by a clinical examination including performing the alternating cover test and testing of stance / gait are combined. This score (range=0-17 points) was first proposed by Kuroda and co-workers in 2017 and was compared to the ABCD2-score [24]. In a single-center observational (retrospective) study 498 patients presenting to the ED with vertigo or dizziness were included [24]. Based on the area under the curve (AUC), diagnostic accuracy of the TriAGe+ score was maximal when selecting a cutoff value of 10 points, resulting in a sensitivity of the score of 77.5% and a specificity of 72.1%. Compared to the ABCD2 score, the TriAGe+ score had a significantly larger AUC for the occurrence of stroke (p < 0.001), however, was clearly below diagnostic accuracy values reported for the HINTS(+) or STANDING algorithms. Furthermore, there are no prospective validation studies published for the TriAGe+ score and findings published by Kuroda and colleagues have not been replicated by others. Noteworthy, the HIT and the nystagmus on lateral-gaze test are not part of the TriAGe+ score and more detailed information on how truncal instability was rated is missing. Thus, the value of the TriAGe+ score currently remains unclear and better validated scores such as HINTS+ or STANDING should be considered instead.
Likewise, the PCI-score combines nine items, addressing reported symptoms (type of dizziness), vascular risk factors and focal neurologic findings such as limb or gait ataxia [29]. Importantly, the PCI-score does not include any subtle oculomotor signs. As for the TriAGe+ score the AUC was significantly larger than for the ABCD2 score (0.82 vs. 0.69), resulting in a sensitivity of 94.1% and a specificity of 41.4%. Importantly, this score was retrieved from a retrospective data set and was not prospectively validated, thus limiting its clinical applicability substantially.
2.4. ABCD2 Score
The ABCD2 score (0-7 points) was originally developed to predict the stroke risk in patients that have suffered a transient-ischemic attack (TIA) [30]. In a retrospective study by Navi and colleagues, it has been suggested that such a risk stratification approach based on the ABCD2 score might help identify strokes acutely in ED patients presenting with dizziness [31]. Being based on five items readily assessable in the ED setting, it can be reliably and quickly calculated in the ED setting. Navi and colleagues identified a cut-off value of 4 points or more as indicate of a central (ischemic) cause. Thus, the diagnostic accuracy of the ABCD2-score has been compared to other algorithms proposed for distinguishing peripheral from central causes in acutely dizzy patients, including the TriAGe+ score, the PCI-score, the HINTS+ bedside exam and the STANDING algorithm.
In a prospective, cross-sectional study including high-risk patients with AVS (n=190), using brain MRI including DWI as gold standard in all patients, the area under the receiver operating characteristic [ROC] curve was significantly smaller for the ABCD2 score (0.613, [0.531 - 0.695] than for the HINTS (0.995 [0.985 - 1.000]) [19]. Thus, HINTS (stroke sensitivity=96.5%, specificity=84.4%) substantially outperformed the ABCD2 score (cutoff value= sensitivity=61.1%, specificity=62.3%) for stroke diagnosis in ED patients with AVS. More recently, Gerlier and colleagues compared the HINTS, STANDING and ABCD2 score in a prospective, single center diagnostic cohort study among patients with isolated vertigo and unsteadiness presenting to the ED [23]. While the HINTS and the STANDING algorithm reached high sensitivities of 97% and 94% and negative predictive values (NVP) of 99% and 98%, respectively, the ABCD2 score failed to predict half of central vertigo cases and had a sensitivity of 55% and a NPV of 87% [23]. Likewise, the ABCD2 score was inferior to the TriAGe+ score [24] and the PCI-score [29] as described in detail in the previous paragraph. In a prospective, single-center cross-sectional study including patients with acute dizziness presenting to the ED, the diagnostic accuracy of the ABCD2-score and the HINTS were compared [22]. All patients received a brain MRI including DWI at least 48 hours after symptom onset. Whereas the sensitivity of ABCD2 score for stroke was 71.4% for a score of ≥4, these authors reported 100% sensitivity for the HINTS exam. Noteworthy, when using a combination of a “central pattern of nystagmus”, defined as the presence of a bidirectional gaze-evoked nystagmus, an isolated torsional nystagmus or a vertical nystagmus in any position, and an ABCD2-score of ≥4, a sensitivity for detecting central causes of 100% was achieved as well.
2.5. Gait and Truncal Instability (GTI) Rating
In the hands of neuro-otologists and trained ED physicians, HINTS(+) have been very successfully applied [14]. Less experienced and not appropriately trained ED physicians, however, may be overwhelmed by HINTS(+) or similar algorithms [32,33]. Thus, the search for other, less demanding bedside tests with high diagnostic accuracy in AVS patients is ongoing. Assessing the patient’s ability to walk and stand is part of the established neurological exam in the ED setting, thus emergency physicians are likely more familiar with performing and interpreting these tests than with the HINTS or STANDING algorithm. Therefore, assessing for gait and truncal instability (GTI) has been proposed as a substitute for the HINTS exam for ED physicians that had not received any training in performing the HINTS [21]. In an attempt to provide a graded truncal instability rating, different clinical findings have been linked to grade 1, 2 and 3 truncal instability. For grade 1, either «mild to moderate imbalance with walking independently» [34] or being «unable to stand on tandem Romberg with the eyes open at least for 3 seconds» [35] was considered characteristic. Grade 2 GTI is defined as «severe imbalance with standing, but cannot walk without support» [34] or being «unable to stand on Romberg with the eyes open at least for 3 seconds» [35]. Patients presenting with grade 3 GTI have an “inability to stand upright” (i.e., falling at upright posture) [34,35] or an “inability to sit upright” [35] unassisted.
In a recently published meta-analysis including ten studies reporting on GTI in acutely dizzy patients, pooled estimated sensitivity reached 69.7% (43.3 – 87.9%) and specificity was at 83.7% (52.1 – 96.0%) when considering GTI ratings of 2 or 3 as indicative of a central cause [36]. When comparing performance of ED physicians and neurologists, a low correlation (Spearman’s correlation r2=0.17 was reported in a single study [37].

Table 1.
Overview of proposed scores / algorithms for the assessment of the acutely dizzy patient.
| Score / algorithm | Domains tested | Features | evaluated application | AUC (95% CI) | Sensitivity / specificity (95% CI)* | Comments |
|---|---|---|---|---|---|---|
| HINTS [18] | Subtle oculomotor signs | Horizontal head-impulse test, horizontal gaze-evoked nystagmus, test of skew | AVS with nystagmus | 0.995 (0.985 - 1.000 [19] | 95.3% (92.5 – 98.1%) / 92.6% (88.6 – 96.5%) [14] | Largest number of studies available. Moderate training needed (4-6 hours [23,28]) for successful application. Only patients with at least one vascular risk factor included. |
| HINTS+ [19] | Subtle oculomotor signs | Horizontal head-impulse test, horizontal gaze-evoked nystagmus, test of skew, finger rub | AVS with nystagmus | NA | 97.2% (94.0 – 100.0%) / 92.4% (86.9 – 97.9%) [14] | Only patients with at least one vascular risk factor included. |
| STANDING [20,27] | obvious focal neurologic signs and subtle oculomotor signs | Horizontal head-impulse test, horizontal gaze-evoked nystagmus, truncal ataxia, provocation maneuvers (Hallpike Dix, Pagnini-McClure) | Acute vertigo or dizziness | NA | 93.4% - 100% / 71.8% - 94.3% [36] | Internal and external validation available. More inclusive than HINTS(+) covering positional vertigo (BPPV) also. Moderate training needed (4-6 hours [23,28]) for successful application. |
| ABCD2 score [31] | Presenting sx, vascular risk factors, obvious focal neurologic signs | age, blood pressure, clinical features (unilateral weakness, speech disturbance), duration of symptoms, diabetes | acute vertigo or dizziness (some studies meeting criteria for AVS) | range: 0.613 to 0.79 (0.61 (0.53 - 0.70) [19]; 0.69 (0.63 - 0.75) [29]; 0.73 (0.68-0.78) [24]; 0.79 (0.73– 0.85) [31]) | for a cut-off value of ≥4: 55.7% (43.3 – 67.5%) / 81.8% (76.4 – 86.2%) [23]; 61.1% (52 – 70%) / 62.3% (51 – 72%) [19] | low diagnostic accuracy in acutely dizzy patients |
| TriAGe+ score [24] | Presenting sx, vascular risk factors, obvious focal neurologic signs, subtle oculomotor signs | triggers, atrial fibrillation, male gender, blood pressure ≥ 140 / 90mm Hg, brainstem or cerebellar dysfunction (incl. skew deviation, truncal ataxia), focal weakness or speech impairment, dizziness, no history of vertigo / dizziness, labyrinth / vestibular disease | acute vertigo or dizziness | 0.82 (0.78-0.86) | for a cut-off value of 10 points: 77.5% (72.8 - 81.8%) / 72.1% (64.1 - 79.2%), | Single center, retrospective study, no prospective validation studies available |
| PCI score [29] | Past history, presenting sx, vascular risk factors, obvious focal neurologic signs | high blood pressure, diabetes mellitus, ischemic stroke, rotating and rocking, difficulty in speech, tinnitus, limb and sensory deficit, gait ataxia, and limb ataxia. | acute vertigo or dizziness | 0.82 (0.77 to 0.87) | for a cut-off value of 0 points: 94.1% (NA) / 41.4% (NA) | Single center, retrospective study, no prospective validation studies available |
| GTI rating [21,34,35] | obvious focal neurologic signs | gait and truncal instability (graded rating) | acute vertigo, dizziness or gait imbalance | NA | for a cut-off value of grade 2: 69.7% (43.3 – 87.9% / 83.7% (52.1 – 96.0%) [36] | Lower sensitivity than HINTS(+) or STANDING, but applicable also in patients with isolated truncal instability (without nystagmus) |
Abbreviations: AUC=area under curve values in receiver operating characteristics (ROC) curve; AVS=acute vestibular syndrome; BPPV=benign paroxysmal positional vertigo; CI=confidence interval; NA= not available; HINTS (Head impulse, nystagmus, test of skew); GTI=gait and truncal instability; PCI=posterior circulation infarct; STANDING=sponTaneous and positional nystagmus, the evaluation of the nystagmus Direction, the head impulse test, and the evaluation of equilibrium (standing); sx=symptoms. * Whenever available, data from systematic reviews and meta-analyses were reported.
Focusing on grade 3 GTI, another recent meta-analysis found a sensitivity of 35.8% (5.2 – 66.5%) and a specificity of 99.2% (97.8 – 100.0%), emphasizing that the presence of grade 3 GTI is highly suggestive of a central cause [14], whereas absence of grade 3 GTI does not exclude presence of a central cause of AVS (missing 2/3 of all vertebrobasilar strokes with this cut-off value. Furthermore, in patients presenting with acute truncal ataxia without (spontaneous or gaze-evoked) nystagmus, HINTS may not be applicable. Considering the graded GTI rating instead may therefore provide useful, as recently demonstrated by Carmona and colleagues [38].
Importantly, several limitating factors in GTI analysis need to be considered. First, timing of GTI testing varied amongst studies. Whereas some studies applied truncal instability testing early in the clinical examination, others performed testing only after having the patient to rest for at least 5-10min. Second, severe nausea or motion intolerance may prevent from testing for truncal ataxia, thus no combined GTI grade 2&3 rating can be retrieved [39]. However, assessing the ability to sit freely in bed can be considered a “minimal version“ of the GTI assessment, allowing to detect those patients with severe (i.e., grade 3) gait and truncal instability and thus having very likely a central cause of their AVS.
3. Discussion
For the bedside clinical assessment of acutely dizzy patients meeting diagnostic criteria of an acute vestibular syndrome, looking for subtle oculomotor signs is key to increase diagnostic accuracy. This approach has been initiated by the introduction of the HINTS examination in 2009, with growing popularity both amongst specialists and ED physicians over the years. With more than ten high level of evidence studies reporting on unselected patient populations, the utility of the HINTS has been underlined. Thus, it is not surprisingly, that performing the HINTS at the bedside is strongly recommended in the current GRACE-3 guideline on the management of the acutely dizzy patient in the ED [26]. Both the HINTS(+) exam and the STANDING algorithm are very good exclusion tests in the hands of trained emergency physicians, non sub-specialists and neuro-otology / neuro-ophthalmology subspecialists [14]. In the study by Gerlier and colleagues as little as six hours of training by an otologist was sufficient to reliably perform and interpret both HINTS and STANDING algorithms [23]. Thus, both the HINTS and the STANDING algorithm can be considered as gatekeepers, with the initiation of further diagnostic testing (especially brain imaging) only in cases where bedside testing points to a central cause of AVS. Ideally, HINTS+ are combined with a graded GTI rating or the STANDING algorithm is used instead. Stand-alone use of the GTI rating will result in inferior diagnostic accuracy compared to HINTS+ and STANDING, thus should only be considered if testing for subtle oculomotor signs is not applicable or feasible (e.g., due to lack of training). Other scores or grading systems reviewed here have substantially lower diagnostic accuracy and lack high-quality, prospective validation studies. This is true both for the ABCD2-score, the TriAGe+ score and the PCI-score. Thus, application of these scoring systems in AVS patients cannot be recommended at this time.
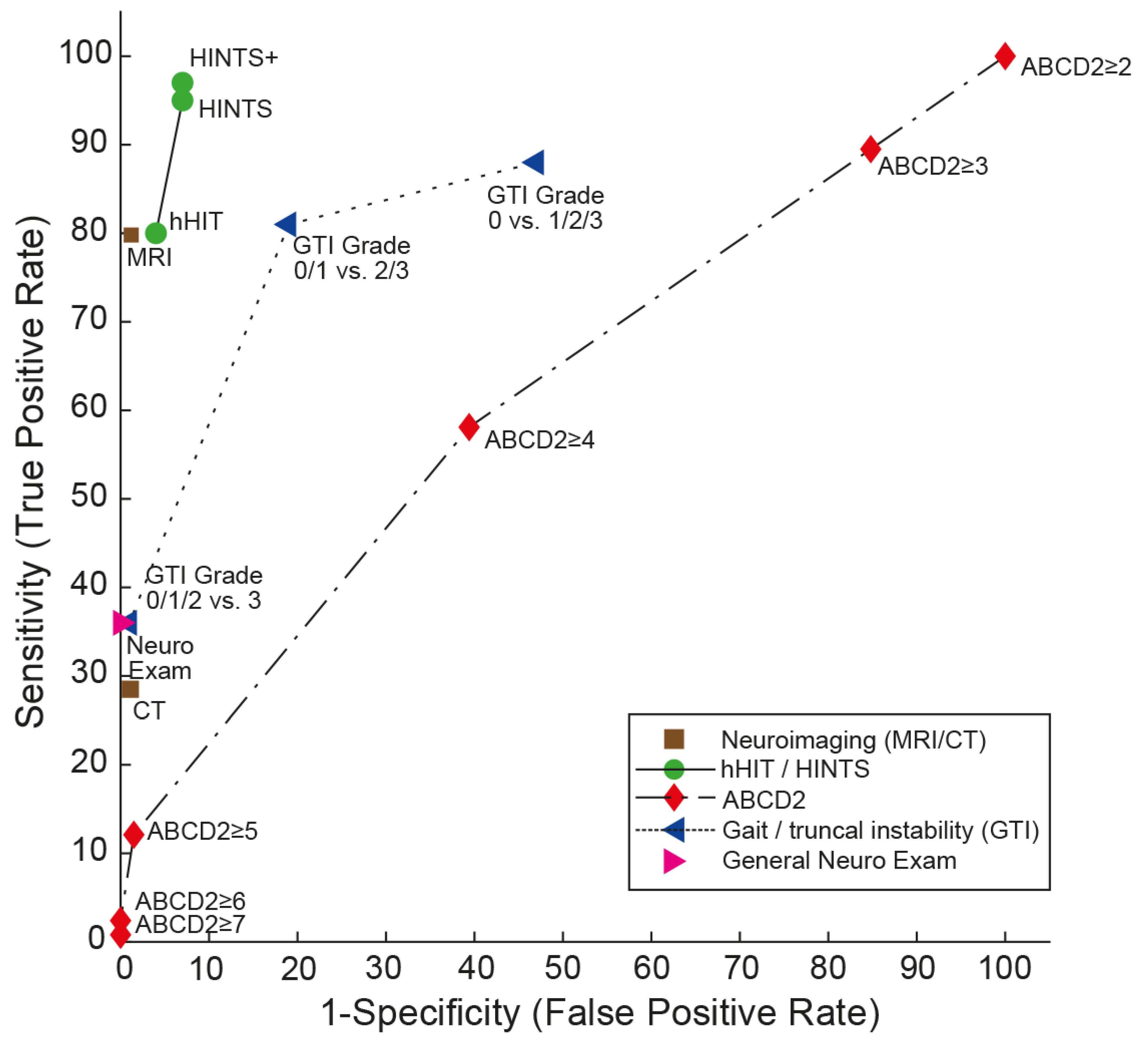
Importantly, both HINTS(+) [14] and STANDING outperformed early (i.e., within first 24-48h) MRI-DWI, which has a sensitivity of 81.1 (73.3 – 88.8) and a specificity of 99.9 (99.6 – 100.0) (based on a systematic review from [40]), as shown in Figure 1. Likewise, the GTI rating outperformed brain CT [14]. For small brainstem strokes (with a diameter of , the sensitivity of early MRI-DWI may be as low as 47% [15]. This underlines the importance of bedside testing in the acutely dizzy patient for treatment decisions and further referral of patients to e.g. a stroke unit.
4. Future Directions
The diagnostic work-up of the acutely dizzy patient remains challenging due to the broad differential diagnosis, spreading over many different specialties and the urgence to distinguish dangerous, potentially life-threating central causes from self-limited peripheral causes. Lacking training in performing and interpreting subtle oculomotor findings such as nystagmus patterns, aVOR-responses on head-impulse testing and gait patterns constitute important limitations especially in frontline providers. Most ED physicians are not yet familiar with a structured approach to the dizzy patient as e.g. outlined in the TiTrATE approach and HINTS(+) or similar bedside algorithms [17,26]. While the introduction of quantitative HINTS to the ED seems promising, increasing the diagnostic accuracy beyond that of neuro-otology experts [41,42], this concept is far from being implemented broadly in EDs in the world. Lacking expertise in applying and interpreting these testing 24/7 and expensive equipment constitute potential obstacles for a more wide-spread use in the near future.
Figure 1.
Summary receiver operating characteristic (SROC) curve analysis for the “HINTS (Head Impulse, Nystagmus, Test of Skew) family” compared with neuroimaging (computed tomography [CT] or magnetic resonance imaging with diffusion-weighted sequences [MRI-DWI], values used as published by Shah and colleagues [40]), graded gait/truncal instability (GTI) ratings, general neurologic exam and vascular risk stratification by ABCD2 (age, blood pressure, clinical features, duration of symptoms, diabetes) score (data from a single study [19]) for detecting stroke in patients presenting the acute vestibular syndrome (modified after [43]). SROC curves are shown for five different diagnostic approaches to diagnosing stroke in the acute vestibular syndrome. A perfect test or decision rule has threshold cutoffs in the upper left corner (100% sensitivity, 100% specificity) and an area under the curve (AUC) of 1.0. Note that the gait/truncal instability ratings outperform the ABCD2 score and the general neurologic exam but are clearly inferior compared to the HINTS family of eye movement tests. Both HINTS and HINTS plus (HINTS plus new hearing loss detected by finger rubbing or similar) demonstrate a higher diagnostic accuracy for ruling out stroke than MRI including DWI. Reused with permission from John Wiley and Sons. Abbreviations: hHIT=horizontal head-impulse test.
Figure 1.
Summary receiver operating characteristic (SROC) curve analysis for the “HINTS (Head Impulse, Nystagmus, Test of Skew) family” compared with neuroimaging (computed tomography [CT] or magnetic resonance imaging with diffusion-weighted sequences [MRI-DWI], values used as published by Shah and colleagues [40]), graded gait/truncal instability (GTI) ratings, general neurologic exam and vascular risk stratification by ABCD2 (age, blood pressure, clinical features, duration of symptoms, diabetes) score (data from a single study [19]) for detecting stroke in patients presenting the acute vestibular syndrome (modified after [43]). SROC curves are shown for five different diagnostic approaches to diagnosing stroke in the acute vestibular syndrome. A perfect test or decision rule has threshold cutoffs in the upper left corner (100% sensitivity, 100% specificity) and an area under the curve (AUC) of 1.0. Note that the gait/truncal instability ratings outperform the ABCD2 score and the general neurologic exam but are clearly inferior compared to the HINTS family of eye movement tests. Both HINTS and HINTS plus (HINTS plus new hearing loss detected by finger rubbing or similar) demonstrate a higher diagnostic accuracy for ruling out stroke than MRI including DWI. Reused with permission from John Wiley and Sons. Abbreviations: hHIT=horizontal head-impulse test.
Thus, disseminating the knowledge about management of the acutely dizzy patient to the frontline providers and providing dedicated training in HINTS+ or STANDING techniques will remain key to improve the diagnostic accuracy and to avoid unnecessary brain imaging.
Author Contributions
AAT was responsible for all contents of this manuscript, including conceptualization of the critical review, reviewing identified manuscripts, drafting and editing the manuscript. AAT has approved the final version of the manuscript.
Funding
None.
Acknowledgments
None.
Conflicts of Interest
The author (AAT) declares no conflict of interest.
References
- Kerber, K.A.; Meurer, W.J.; West, B.T.; Fendrick, A.M. Dizziness presentations in U.S. emergency departments, 1995-2004. Acad Emerg Med 2008, 15, 744–750. [Google Scholar] [CrossRef]
- Goeldlin, M.; Gaschen, J.; Kammer, C.; Comolli, L.; Bernasconi, C.A.; Spiegel, R.; Bassetti, C.L.; Exadaktylos, A.K.; Lehmann, B.; Mantokoudis, G.; et al. Frequency, aetiology, and impact of vestibular symptoms in the emergency department: a neglected red flag. J Neurol 2019, 266, 3076–3086. [Google Scholar] [CrossRef] [PubMed]
- Newman-Toker, D.E.; Hsieh, Y.H.; Camargo, C.A., Jr.; Pelletier, A.J.; Butchy, G.T.; Edlow, J.A. Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample. Mayo Clin Proc 2008, 83, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Ljunggren, M.; Persson, J.; Salzer, J. Dizziness and the Acute Vestibular Syndrome at the Emergency Department: A Population-Based Descriptive Study. Eur Neurol 2018, 79, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Newman-Toker, D.E.; Camargo, C.A., Jr.; Hsieh, Y.H.; Pelletier, A.J.; Edlow, J.A. Disconnect between charted vestibular diagnoses and emergency department management decisions: a cross-sectional analysis from a nationally representative sample. Acad Emerg Med 2009, 16, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Newman-Toker, D.E.; McDonald, K.M.; Meltzer, D.O. How much diagnostic safety can we afford, and how should we decide? A health economics perspective. BMJ Qual Saf 2013, 22 Suppl 2, ii11–ii20. [Google Scholar] [CrossRef]
- Saber Tehrani, A.S.; Coughlan, D.; Hsieh, Y.H.; Mantokoudis, G.; Korley, F.K.; Kerber, K.A.; Frick, K.D.; Newman-Toker, D.E. Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med 2013, 20, 689–696. [Google Scholar] [CrossRef]
- Tarnutzer, A.A.; Lee, S.H.; Robinson, K.A.; Wang, Z.; Edlow, J.A.; Newman-Toker, D.E. ED misdiagnosis of cerebrovascular events in the era of modern neuroimaging: A meta-analysis. Neurology 2017, 88, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Kerber, K.A.; Brown, D.L.; Lisabeth, L.D.; Smith, M.A.; Morgenstern, L.B. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke 2006, 37, 2484–2487. [Google Scholar] [CrossRef]
- ICD-11 (Mortality and Morbidity Statistics). Available online: https://icd.who.int/dev11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1462112221 (accessed on October 18th 2018).
- Tarnutzer, A.A.; Berkowitz, A.L.; Robinson, K.A.; Hsieh, Y.H.; Newman-Toker, D.E. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ 2011, 183, E571–592. [Google Scholar] [CrossRef]
- Kerber, K.A.; Schweigler, L.; West, B.T.; Fendrick, A.M.; Morgenstern, L.B. Value of computed tomography scans in ED dizziness visits: analysis from a nationally representative sample. Am J Emerg Med 2010, 28, 1030–1036. [Google Scholar] [CrossRef]
- Ahsan, S.F.; Syamal, M.N.; Yaremchuk, K.; Peterson, E.; Seidman, M. The costs and utility of imaging in evaluating dizzy patients in the emergency room. Laryngoscope 2013, 123, 2250–2253. [Google Scholar] [CrossRef] [PubMed]
- Tarnutzer, A.A.; Gold, D.; Wang, Z.; Robinson, K.A.; Kattah, J.C.; Mantokoudis, G.; Saber Tehrani, A.S.; Zee, D.S.; Edlow, J.A.; Newman-Toker, D.E. Impact of Clinician Training Background and Stroke Location on Bedside Diagnostic Accuracy in the Acute Vestibular Syndrome - A Meta-Analysis. Ann Neurol 2023. [Google Scholar] [CrossRef]
- Saber Tehrani, A.S.; Kattah, J.C.; Mantokoudis, G.; Pula, J.H.; Nair, D.; Blitz, A.; Ying, S.; Hanley, D.F.; Zee, D.S.; Newman-Toker, D.E. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology 2014, 83, 169–173. [Google Scholar] [CrossRef]
- Saber Tehrani, A.S.; Kattah, J.C.; Kerber, K.A.; Gold, D.R.; Zee, D.S.; Urrutia, V.C.; Newman-Toker, D.E. Diagnosing Stroke in Acute Dizziness and Vertigo: Pitfalls and Pearls. Stroke 2018, 49, 788–795. [Google Scholar] [CrossRef]
- Newman-Toker, D.E.; Edlow, J.A. TiTrATE: A Novel, Evidence-Based Approach to Diagnosing Acute Dizziness and Vertigo. Neurol Clin 2015, 33, 577–599. [Google Scholar] [CrossRef]
- Kattah, J.C.; Talkad, A.V.; Wang, D.Z.; Hsieh, Y.H.; Newman-Toker, D.E. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke 2009, 40, 3504–3510. [Google Scholar] [CrossRef] [PubMed]
- Newman-Toker, D.E.; Kerber, K.A.; Hsieh, Y.H.; Pula, J.H.; Omron, R.; Saber Tehrani, A.S.; Mantokoudis, G.; Hanley, D.F.; Zee, D.S.; Kattah, J.C. HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness. Acad Emerg Med 2013, 20, 986–996. [Google Scholar] [CrossRef] [PubMed]
- Vanni, S.; Nazerian, P.; Casati, C.; Moroni, F.; Risso, M.; Ottaviani, M.; Pecci, R.; Pepe, G.; Vannucchi, P.; Grifoni, S. Can emergency physicians accurately and reliably assess acute vertigo in the emergency department? Emerg Med Australas 2015, 27, 126–131. [Google Scholar] [CrossRef]
- Carmona, S.; Martinez, C.; Zalazar, G.; Moro, M.; Batuecas-Caletrio, A.; Luis, L.; Gordon, C. The Diagnostic Accuracy of Truncal Ataxia and HINTS as Cardinal Signs for Acute Vestibular Syndrome. Front Neurol 2016, 7, 125. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, Y.; Pan, Q.; Liu, J.; Zhu, Y.; Tan, G.; Zhan, Q.; Zhou, J. Central nystagmus plus ABCD(2) identifying stroke in acute dizziness presentations. Acad Emerg Med 2021, 28, 1118–1123. [Google Scholar] [CrossRef]
- Gerlier, C.; Hoarau, M.; Fels, A.; Vitaux, H.; Mousset, C.; Farhat, W.; Firmin, M.; Pouyet, V.; Paoli, A.; Chatellier, G.; et al. Differentiating central from peripheral causes of acute vertigo in an emergency setting with the HINTS, STANDING, and ABCD2 tests: A diagnostic cohort study. Acad Emerg Med 2021, 28, 1368–1378. [Google Scholar] [CrossRef]
- Kuroda, R.; Nakada, T.; Ojima, T.; Serizawa, M.; Imai, N.; Yagi, N.; Tasaki, A.; Aoki, M.; Oiwa, T.; Ogane, T.; et al. The TriAGe+ Score for Vertigo or Dizziness: A Diagnostic Model for Stroke in the Emergency Department. J Stroke Cerebrovasc Dis 2017, 26, 1144–1153. [Google Scholar] [CrossRef]
- Halmagyi, G.M.; Curthoys, I.S. A clinical sign of canal paresis. Arch Neurol 1988, 45, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Edlow, J.A.; Carpenter, C.; Akhter, M.; Khoujah, D.; Marcolini, E.; Meurer, W.J.; Morrill, D.; Naples, J.G.; Ohle, R.; Omron, R.; et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): Acute dizziness and vertigo in the emergency department. Acad Emerg Med 2023, 30, 442–486. [Google Scholar] [CrossRef] [PubMed]
- Vanni, S.; Pecci, R.; Edlow, J.A.; Nazerian, P.; Santimone, R.; Pepe, G.; Moretti, M.; Pavellini, A.; Caviglioli, C.; Casula, C.; et al. Differential Diagnosis of Vertigo in the Emergency Department: A Prospective Validation Study of the STANDING Algorithm. Front Neurol 2017, 8, 590. [Google Scholar] [CrossRef] [PubMed]
- Gerlier, C.; Fels, A.; Vitaux, H.; Mousset, C.; Perugini, A.; Chatellier, G.; Ganansia, O. Effectiveness and reliability of the four-step STANDING algorithm performed by interns and senior emergency physicians for predicting central causes of vertigo. Acad Emerg Med 2023, 30, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Su, R.; Deng, M.; Liu, J.; Hu, Q.; Song, Z. A Posterior Circulation Ischemia Risk Score System to Assist the Diagnosis of Dizziness. J Stroke Cerebrovasc Dis 2018, 27, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Rothwell, P.M.; Nguyen-Huynh, M.N.; Giles, M.F.; Elkins, J.S.; Bernstein, A.L.; Sidney, S. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet 2007, 369, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Kamel, H.; Shah, M.P.; Grossman, A.W.; Wong, C.; Poisson, S.N.; Whetstone, W.D.; Josephson, S.A.; Johnston, S.C.; Kim, A.S. Application of the ABCD2 score to identify cerebrovascular causes of dizziness in the emergency department. Stroke 2012, 43, 1484–1489. [Google Scholar] [CrossRef]
- Ohle, R.; Montpellier, R.A.; Marchadier, V.; Wharton, A.; McIsaac, S.; Anderson, M.; Savage, D. Can Emergency Physicians Accurately Rule Out a Central Cause of Vertigo Using the HINTS Examination? A Systematic Review and Meta-analysis. Acad Emerg Med 2020, 27, 887–896. [Google Scholar] [CrossRef]
- Dmitriew, C.; Regis, A.; Bodunde, O.; Lepage, R.; Turgeon, Z.; McIsaac, S.; Ohle, R. Diagnostic Accuracy of the HINTS Exam in an Emergency Department: A Retrospective Chart Review. Acad Emerg Med 2021, 28, 387–393. [Google Scholar] [CrossRef]
- Lee, H.; Sohn, S.I.; Cho, Y.W.; Lee, S.R.; Ahn, B.H.; Park, B.R.; Baloh, R.W. Cerebellar infarction presenting isolated vertigo: frequency and vascular topographical patterns. Neurology 2006, 67, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Moon, I.S.; Kim, J.S.; Choi, K.D.; Kim, M.J.; Oh, S.Y.; Lee, H.; Lee, H.S.; Park, S.H. Isolated nodular infarction. Stroke 2009, 40, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.P.; Oliveira, J.E.S.L.; Farah, W.; Seisa, M.O.; Balla, A.K.; Christensen, A.; Farah, M.; Hasan, B.; Bellolio, F.; Murad, M.H. Diagnostic accuracy of the physical examination in emergency department patients with acute vertigo or dizziness: A systematic review and meta-analysis for GRACE-3. Acad Emerg Med 2023, 30, 552–578. [Google Scholar] [CrossRef] [PubMed]
- Perloff, M.D.; Patel, N.S.; Kase, C.S.; Oza, A.U.; Voetsch, B.; Romero, J.R. Cerebellar stroke presenting with isolated dizziness: Brain MRI in 136 patients. Am J Emerg Med 2017, 35, 1724–1729. [Google Scholar] [CrossRef] [PubMed]
- Carmona, S.; Martinez, C.; Zalazar, G.; Koohi, N.; Kaski, D. Acute truncal ataxia without nystagmus in patients with acute vertigo. Eur J Neurol 2023, 30, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Honda, S.; Inatomi, Y.; Yonehara, T.; Hashimoto, Y.; Hirano, T.; Ando, Y.; Uchino, M. Discrimination of acute ischemic stroke from nonischemic vertigo in patients presenting with only imbalance. J Stroke Cerebrovasc Dis 2014, 23, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.P.; Oliveira, J.E.S.L.; Farah, W.; Seisa, M.; Kara Balla, A.; Christensen, A.; Farah, M.; Hasan, B.; Bellolio, F.; Murad, M.H. Diagnostic accuracy of neuroimaging in emergency department patients with acute vertigo or dizziness: A systematic review and meta-analysis for the Guidelines for Reasonable and Appropriate Care in the Emergency Department. Acad Emerg Med 2022. [Google Scholar] [CrossRef]
- Korda, A.; Wimmer, W.; Zamaro, E.; Wagner, F.; Sauter, T.C.; Caversaccio, M.D.; Mantokoudis, G. Videooculography "HINTS" in Acute Vestibular Syndrome: A Prospective Study. Front Neurol 2022, 13, 920357. [Google Scholar] [CrossRef]
- Nham, B.; Reid, N.; Bein, K.; Bradshaw, A.P.; McGarvie, L.A.; Argaet, E.C.; Young, A.S.; Watson, S.R.; Halmagyi, G.M.; Black, D.A.; et al. Capturing vertigo in the emergency room: three tools to double the rate of diagnosis. J Neurol 2022, 269, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Newman-Toker, D.E.; Curthoys, I.S.; Halmagyi, G.M. Diagnosing Stroke in Acute Vertigo: The HINTS Family of Eye Movement Tests and the Future of the "Eye ECG". Semin Neurol 2015, 35, 506–521. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



