Submitted:
26 May 2023
Posted:
29 May 2023
You are already at the latest version
Abstract
Background: Micro-RNAs (miRNA) are emerging as biomarkers in the detection and prognosis of cancers due to their inherent stability and resilience.
Methods: To summarize evidence regarding urinary miRNA (umiRNAs) role in the detection, prognosis and therapeutic management of urological cancers, we performed a systematic review of the most important scientific databases using the following keywords: (urinary mir-na)AND(prostate cancer); (urinary mirna)AND(bladder cancer); (urinary mirna)AND(renal cancer); (urinary mirna)AND(testicular cancer); (urinary mirna)AND(urothelial cancer).
Results: Of all, 1364 articles were initially selected. Only original studies in the English language on human specimens were considered for inclusion in our systematic review. Thus, a convenient sample of 60 original articles was identified. Urinary miRNA (UmiRNAs) are downregulated in prostate cancers and may serve as potential non-invasive molecular biomarkers. Several umiR-NAs have been identified as diagnostic biomarkers of urothelial carcinoma and bladder cancer (BCa), allowing to discriminate malignant from non-malignant forms of haematuria. UmiRNAs could serve as therapeutic targets or recurrence markers of non-muscle invasive BCa and could predict the aggressivity and prognosis of muscle-invasive BCa. In renal cell carcinoma, miRNAs have been identified as predictors of tumour detection, aggressiveness, and progression to metastasis.
Conclusion: umiRNAs could play an important role in the diagnosis, prognosis, and therapy of urological cancers.
Keywords:
Micro-RNAs
; biomarkers
; urological cancers
; prostate cancer
; bladder cancer
; Upper Tract Urothelial Carcinoma
; renal cancer
1. Introduction
Urological cancers could affect the kidney, upper urinary tract, bladder, prostate, testis and penis. In developed countries, kidney, bladder, and prostate cancers are the three major types of genitourinary cancers, with 166.440, 228.730, and 486.840 worldwide deaths in 2019, respectively (1). Because of the high morbidity and mortality associated, the improvement in early diagnosis is crucial for better clinical results. Although the identification of emerging targets and novel molecules has resulted in encouraging progress in the management of genitourinary tumors, valuable tools for cancer diagnosis and follow-up continue to be lacking. Therefore, the research for reliable prognostic and predictive biomarkers for the early diagnosis in patients with genitourinary malignancies is actually an evolving landscape. In this context, an ideal biomarker should ensure high-accuracy results and should be as minimally invasive as possible to obtain (2).
In the last few years, microRNAs (miRNAs) emerged as useful markers thanks to their occurrence in all tissues. Indeed, normal and cancerous cells can use exosomes to secrete these molecules into blood or urine as free-circulating miRNAs (3).
MiRNAs are 20-25-nucleotide-long noncoding single-stranded RNA molecules which regulate gene expression, through the breakdown of the mRNA transcript or inhibiting translation of the mRNA to protein (4).
Changes in the expression of miRNAs have been associated with progression of different cancers (5). Indeed, miRNAs can disturb expression of oncogenic or tumor-suppressive target genes implicated in cancer pathogenesis (6). Notably, several miRNAs have been found to be upregulated or downregulated in various tumors, with oncogenes or oncosuppressor role (7).
MiRNAs are emerging as diagnostic tools in several tumors. Previous studies assessed their levels in surgical and liquid samples from patients with cancers. However, samples from operative specimens could be altered by coagulation, necrosis, and formalin fixation. In this context urinary miRNAs (umiRNAs) take advantages from bypassing alternating process and form the reduced vulnerability to urinary RNase in urine (8). Furthermore, compared to local tumor sample, urine is a readily accessible source that does not need invasive procedures and represents the genetic profile of the entire tumor (9).
In consequence, considering the high worldwide prevalence of urological cancers and the growing interest in the role of miRNAs, the current systematic review aims at summarizing the role of umiRNAs in the detection of any urological cancers.
2. Literature search results
The PRISMA flow chart of the study selection process is shown in Figure 1. Initial search identified 1364 studies. Of these, 253 were excluded for duplication. After applying selection criteria, other 989 records were excluded. A total of 36 studies, including over 3900 patients, were included in the systematic review. Sixteen studies, including 2498 patients, reported data for bladder cancer (Table 1). Ten studies, including 641 patients, reported data on miRNA for prostate cancer (Table 2). Eight studies, including 521 patients, reported data on renal cancer. (Table 3). Two studies with an overall of 240 patients reported results for urothelial cancer (Table 4).
3. Results
3.1. The role of micro-rna in the detection of bladder cancer
Bladder cancer (BC) is one of the most common urogenital cancers worldwide(10) . Among the other types, urothelial carcinoma (UC) is the most common histological type with a prevalence of almost 90% (11). According to European Association of Urology (EAU) guidelines, the diagnosis of BC is actually based on imaging, cytology, cystoscopy and histopathological analysis of sampled tissue from either cold-cup biopsy or trans-urethral resection (TURB) (12,13). Based on histological manifestations and biological traits, BC can be classified in non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC) (14).
Being these diagnostic methods uncomfortable for the patients and expensive for the healthcare system, new biomarkers as umiRNAs are crucial in the suspicion of BC (15,16).
Since the 2010s, numerous studies demonstrated how types and urinary concentration of miRNAs could reflect carcinogenicity and invasiveness of BC. For instance, Kim et al. have demonstrated over-expression of miR-214 in the urine samples of the NMIBC patients compared to control specimens (20.08±3.21 vs. 18.96±2.68, p=0.002). Furthermore, lower levels of the miR-214 were associated with a significantly longer recurrence-free survival time, making it an independent predictor of NMIBC recurrence (p=0.012) (17).
Over-expression of miR-155 in NMIBC patients has been reported by Zhang et al.. The authors showed how the tested umiRNA allow to discriminate between patients with NMIBC from patients with cystitis and healthy controls, with 80.2% of sensitivity and 84.6 % of specificity (18). Nevertheless, the relationship between miR-155 over-expression and bladder cancer development is not fully elucidated. A possible explanation is the action of miR-155 in promoting some tumor cell growth via Wnt/β-catenin signaling activation (19).
In 2018, Piao et al. explored a novel method to discriminate bladder cancer from benign hematuria by measuring the urinary miR-6124 to miR-4511 ratio. The capacity of this proposed diagnostic tool enabled the discrimination of BC from patients with hematuria under nonmalignant conditions with a sensitivity higher than 90% (AUC: 0.888, 91.5% SN, 76.2% SP) (p<0.001) (20) .
Differences in miR-20a expression in the urine samples from 80 NMIBC patients and 86 healthy individuals were investigated by Huang et al. They found that urinary concentration of miR-20a were significantly higher in NMIBC patients than in healthy controls (p<0.001). Moreover, they showed that larger tumor size and advanced tumor grade were associated with high expression of this umiRNA (all p<0.05)(21).
Sasaki et al. demonstrated that the expression level of miR-146a-5p in patients with BC was higher than healthy individuals (AUC=0.773,95% CI, 0.701-0.892)(p=0.014). Higher umiR-146a-5p concentrations were displayed in patients with high-grade BC and with MIBC with respect to those with low-grade tumors (p=0.0436) or NMIBC (p=0.1391). Moreover, the authors showed that levels of miR-146a-5p decreased to the normal range after TURB (22).
In the multitude of studies on BC, umiR-146 showed the most overlap. In this context, Andreu et al. reported over-expression in low-grade rather than in high-grade disease, whilst Baumgart et al. found overabundance in high-grade more than in lower-graded disease (23,24). Nevertheless, both the research groups showed that this umiR-146 in BC is indeed an inflammasome and the discordance of results might be explained by the inflammatory status in BC and not directly to the aggressiveness of the disease, thus further studies are needed to clarify its role.
Therefore, in addition to the over-expression of umiRNAs in BC, several studies have shown down-regulation of tumor suppressor miRNAs in urinary samples. In 2012, Yun et al. reported down-regulation of miR-145 in NMIBC and MIBC patients compared to healthy controls (77.8% sensitivity and 61.1% specificity for NMIBC, AUC 0.729; 84.1 and 61.1% for MIBC, respectively, AUC 0.790, p<0.001). Moreover, miR-145 urinary levels were lower in MIBC patients than in NMIBC patients (p=0.036). In addition, in the same study the authors reported that also the levels of miR-200a were significantly decreased in NMIBC and MIBC than healthy controls (p<0.001) (25).
In contrast to the previous finding, in 2023 Mamdouh et al. reported that the urinary concentration of miR-200, miR-145 and miR-21 were higher in case of low and high grade BC compared to the controls, depicting a possible oncogene role of those miRNAs (p= 0.02, 0.01 and 0.05 respectively)(26).
To improve accuracy of umiRNAs for the detection of BC, numerous studies analysed combination tests utilizing multiple umiRNAs. For instance, Mengual et al. identified a subset of six umiRNAs (miR-187, miR-18a*, miR-25, miR-142-3p, miR-140-5p, and miR-204) founding a specificity of 86.5% and a sensibility of 84.8% (AUC 0.92) in the diagnosis of BC (27).
Three urine microRNAs, miR-21-5p, miR-141-3p, and miR-205-5p, have been found by Ghorbanmehr et al. as prospective non-invasive diagnostic biomarkers candidates for the identification of both bladder and prostate cancer (28).
Hofbauer et al. achieved comparable results with 88.3% sensitivity using six different umiRNAs (let-7c, miR-135a, miR-135b, miR-148a,miR-204, and miR-345), which can predict the presence of BC from urine samples , independently from grading and staging (AUC 0.88) (29).
Pardini et al. also confirmed, by firstly using the Next-Generation Sequencing (NGS), that the combination of specific miRNAs profiles may provide more robust results than individual miRNAs. Indeed, the authors showed a statistically significant improvement in the AUC discrimination between BC and controls (from 50% to 70%), using a set of three umiRNAs (miR-30a-5p, let-7c-5p and miR-486-5p) (30). Accordingly, Braicu et al. proposed interactions between the genes associated to BC carcinogenesis (TP53, FGFR3, KDR, PIK3CA, and ATM) and altered miRNAs expressions (miR-139-5p, miR-143-5p, miR-23a-3p, miR-141-3p, miR-205-5p). In particular, three up-regulated miRNAs (miR-141b, miR-200 s or miR-205) and two downregulated (miR-139-5p and miR-143-5p) target these multiple genes involved in the carcinogenesis of bladder cancer (31).
Likewise, Lin et al. in 2021 concluded that let-7b-5p, miR-149-5p, miR-146a-5p, miR-193a-5p, and miR-423-5p were significantly increased in BC compared with healthy specimens. Moreover, these umiRNAs had a significant impact on cancer-related signaling pathways implied in cell growth, proliferation and survival, such as: PI3K/AKT, MAPK, focal adhesion and Erb(32,33).
In 2022, Moisoiu et al. firstly demonstrated an (AUC) of 0.92 ± 0.06 in discriminating patients with BC from controls by the combination of surface-enhanced Raman spectroscopy (SERS) with three differentially expressed miRNAs (miR-34a-5p, miR-205-3p, miR-210-3p). This unique method seems to guarantee a better BC’s diagnostic and molecular stratification, even if studies in larger cohorts should be performed to confirm these results (34).
In conclusion, in relation to T stage, De Long et al. identified seven miRNAs over-expressed in the bladder cancer group (p<0.05). Of the RNA analyzed, miR-940 was differentially expressed between patients with MIBC compared with patients with NMIBC. In particular, miR-940 level was the highest in advanced disease (pT1 G3 and ≥ pT2) and the lowest in absence of tumor (healthy volunteers with or without history of urothelial carcinoma) (35). Contrarily, Baumgart et al. demonstrated a downregulation of miR-138-5p between pT2 and pT3–4 tumors, indicating that low expression correlates with an aggressive phenotype(24). It might be explained by the fact that low expression of this miRNA, as shown in another two studies, results in higher expression of the EMT-associated protein ZEB2(36,37).
3.2. The role of micro-RNA in the detection of prostate cancer
Prostate cancer (PCa) is the most commonly diagnosed malignancy among men and the fifth cause of male cancer-related death worldwide (11,38).
The suspicion of prostate cancer arises from an abnormal digit-rectal examination or/and an elevated PSA value (39). The gold standard for the diagnosis is then obtained by transperineal or transrectal prostate biopsy(40). Multi-parametric magnetic resonance imaging (mpMRI) should be recommended before prostate biopsy(41).
Although serum prostate-specific antigen (PSA) is the most widely used biomarker for prostate cancer (PCa) screening, it has several limitations. The lack of specificity and the limited ability of this serum marker to distinguish between malignant and benign causes of its elevation, might in fact result in overdiagnosis and a significant risk of false-positive results (42).
To overcome these limitations, numerous studies have been conducted to identify new biomarkers and several miRNAs have been shown to be involved in the development and progression of PCa(43–45).
The first studies investigated the miRNAs profile directly in prostate carcinoma tissue. Indeed, in 2009, Schaefer et al. firstly showed the upregulation of miR-183 and the downregulation of miR-205 in PCa tissues (46).
After that, in 2015 Stephan et al. aimed to translate these results into a urine-based testing procedure. They enrolled 38 patients with PCa and 38 without PCa to test the clinical utility of miR-183 and miR-205 in urines samples founding that urinary concentration of those miRNAs were comparable in patients with and without PCa (47).
Salido-Guadarrama et al. showed that elevated urinary levels of miR-100 and miR-200b were associated with advanced PCa (48). Furthermore, miR-100 remained upregulated throughout the carcinogenic process and its downregulation has been observed for hormone-refractory PCa (49,50).
In 2017, Rodriguez et al. showed that miR-196a-5p and miR-501-3p, downregulated in urinary exosomes, are promising biomarkers for PCa (51). In the same year, Foj et al. observed that, when compared to samples from healthy men, the urinary pellet of PCa patients had higher concentrations of miR-21, miR-141, and miR-375 (p 0.001, 0.033, and 0.038, respectively). On the other hand, based on the study by Nadiminty et al. (52), they found no significant differences on the expression of let-7c . Moreover, they found also an higher expression of miR-141 in patients with higher Gleason score (p=0.034) (53).
Supporting these notions, Ghorbanmehr et al. collected urines samples from 110 men with BC (n = 45), PCa (n = 23) cancer, benign prostatic hyperplasia (BPH) (n = 22) and healthy men (n = 20). They assessed the expression of miR-21-5p, mi-R-141-3p, and miR-205p to identify and discriminate PCa patients from those with BPH (p 0.001, 0.005, and 0.020, respectively). Moreover, the authors reported how the upregulation of those miRNAs in urine sample was associated with higher cancer detection specificity in PCa compared to PSA test (28).
Markert et al. analyzed urine samples of 53 patients (25 with BPH and 28 with PCa) and showing that miR-19b and miR-26a were significantly downregulated in PCa patients compared to BPH patients (54). These microRNAs seem to play a role in regulating PTEN (Phosphatase and tensin homolog enzyme), whose mutation is a common event in Pca (55).
In 202,1 Hasanoglu et al. identified miR-320a as a valuable biomarker in the diagnosis of PCa, reporting higher concentrations in PCa patients compared to healthy controls (p= 0.0168) (56). The upregulation of this microRNA confirmed what Porkka et al. reported in a previous study (50).
Over the years, ratio analysis has been used to improve results in microRNA research. It consists of measuring and comparing the expression ratios of up-regulated to down-regulated miRNAs in PCa and control patients. Using this approach, Byun et al. observed that the urinary miR-1913 to miR-3659 ratio was increased in PCa (AUC=0.7,95% CI, 61.4% SN, 71.8% SP), declaring a particular utility in patients within the PSA gray zone ( defined as total serum PSA between 3 to 10 ng/mL) (57).
In addition, in Kang and collegues study the expression ratio of urinary miR-H9 to miR-3659 was quantified, and they affirmed that the ratio was significantly higher in the PCa group than healthy men group (AUC=0.803,95% CI) (p< 0.001) and that it could represents a non-invasive biomarker for PCa (58).
In conclusion, umiRNAs could serve as a supplemental biomarker to PSA for the diagnosis but also in the prediction of cancer progression according to the latest studies. Indeed, in 2022 Lee et al. reported that miR-21-5p, miR-574-3p, and miR6880-5p were significantly higher in patients with CRPC (castration-resistant prostate cancer) and they could be used as potential biomarkers for the prognosis of CRPC (59). In particular, overexpression of miR-21-5p downregulates programmed cell death protein 4, which is a regulator of PCa cell growth and castration resistance, whilst the overexpression of miR-574-3p reflect the down-regulation of the Notch signaling pathway, DNA damage and apoptosis (60,61).
3.3. The role of micro-RNA in the detection of renal cancer
Renal cell carcinoma (RCC) is the sixth most frequently diagnosed cancer in men and the 10th in
women representing the third most frequent urological malignancy worldwide and the 13th most common cause of cancer death worldwide (62–64).
Symptoms related to RCC are usually rare and occur in the late stages(65–67). In this context, several micro-RNA have been tested and identified as early diagnostic markers or as useful tools in the follow-up of treated patients(68). Overall, Cui and Cui, observed a significant positive correlation between human tissue miRNAs and the ones from urine specimen in patients with renal cancer (rho=0.51, p<0.001) (69).
In 2012, von Brandenstein et al. enrolled 25 patients with ccRCC and 5 healthy volunteers. They found that miR-15a levels from paraffin-embedded tissue and from urine samples are inversely related in malignant versus benign renal tumours. Thus, the authors suggested miR-15a as a potential new preoperatively urinary marker of patients with renal cancer (70).
Fedorko et al. analysed the role of the miRNA let-7 family which are widely accepted as a tumour suppressor miRNAs. Indeed, downregulation of the members of let-7 family has been observed in various types of tumour tissue including RCC, while the upregulation has been observed in BCa (71,72). For the specific purpose of their study, the authors analysed urine samples of 69 patients with non-metastatic ccRCC and 36 healthy controls. They identified 6 let-7 miRNA (let-7 let-7a, let-7b, let-7c, let-7d, let-7e, and let-7g) highly expressed in the urine of ccRCC patients with respect to healthy controls (all p<0.015), an in particular let-7a outperforms the others and may be considered as a promising non-invasive biomarker for the detection of clear-cell RCC (73).
Li et al. collected urinary samples from 75 patients diagnosed with ccRCC, 45 healthy volunteers and, to determine a decrease of umiRNAs concentration after surgery, they repeated the collection of urinary samples in 15 patients 7 days after tumour resection. The authors identified that free miR-210 levels were significantly higher in patients with ccRCC than in control subjects (p<0.001) regardless of tumour staging. Moreover, miR-210 levels were significantly reduced one week after surgery, thus directly reflecting the presence of ccRCC (74).
In 2018, Mytsyk et al. aimed at testing the utility of urinary miR-15a as a diagnostic molecular biomarker of ccRCC. They collected urinary samples from 67 patients with various solid renal tumours and 15 healthy controls. MirR-15a allowed to discriminate between malignant and benign renal masses (p<0.01) and its levels were significantly reduced after one week from tumour surgery. Thus, the authors affirmed that mir-15a could be used as a reliable marker for the diagnosis of ccRCC (75).
Song et al. detected the expression of dysregulated miRNAs in urine exosomes of ccRCC patients and healthy individuals, in order to identify a specific dysregulated miRNA. They identified several umiRNAs in patients with ccRCC, PCa, BCa and healthy individuals. Among them the expression levels of miR-30c-5p in the urinary exosomes of ccRCC patients were significantly lower than that of normal individuals. The sensitivity and specificity of urinary exosome miR-30c-5p in the diagnosis of ccRCC were found to be 68.57% and 100%, respectively (76).
In 2020, Cochetti et al. identified twenty-seven significantly overexpressed, and 30 significantly underexpressed, umiRNAs in ccRCC. Among them, they tested the two most overexpressed umiRNAs (miR-122 and miR-15b) plus four more randomly chosen overexpressed miRNAs (miR-1271, miR-629, miR-625, and miR-93), and the most underexpressed miRNA (miR-1260a) plus another randomly chosen underexpressed miRNA (miR-369). The authors compared urinary expression levels in patients vs. healthy controls and concluded that the combined use of urinary miR-122, miR-1271, miR-15b, together with imaging controls, allow to diagnose ccRCC with high sensitivity and specificity (77).
In conclusion, one of the opened challenge in renal cancer identification, is the differentiation with benign masses, such as Oncocytoma (78). To this regard, in 2018 von Brandenstein et al. aimed at finding urinary miRNA allowing to discriminate benign and malign masses. Thus, they collected urinary samples from 26 patients with renal masses and 17 urine samples of healthy volunteers or patients with other pathologies. They found that miR-498 (associated with formation of the oncocytoma-specific slice-form of vimentin, Vim3), miR-183 (associated with increased CO2 levels), miR-205, and miR-31 were specific urinary miRNA guiding the diagnosis for benign Oncocytoma (79). Accordingly, Di Meo et al. tested the sensibility of mi-RNA in discriminating benign oncocytoma from early-stage ccRCC, identifying miR-432-5p and miR-532-5p as presenting the higher discriminatory power, followed by miR-10a-5p, miR-144-3p, miR-28-3p, miR-326, miR-603, and miR-93-3p. In particular, miR-93-3p was identified as the only miRNA associate with progressive ccRCC when downregulated (p=0.042) and with longer overall survival when upregulated (p=0.016) (80).
3.4. The role of micro-RNA in the detection of upper tract urothelial carcinoma
Urothelial carcinomas (UCs) are the sixth most common tumours in developed countries (12). They can be localised in the lower (bladder and urethra) and/or the upper (pyelo-caliceal cavities and ureter) urinary tract. While BCa account for 90–95% of UCs, upper tract UCs (UTUCs) are uncommon and account for only 5–10% of UCs(81,82).
In this section, we aimed at focalising on the role of miRNA in UTUCs detection.
Back in 2011, Yamada et al. evaluated miRNAs expression in clinical samples, using specimens from 104 UC patients underwent cystectomy, between 2003 and 2007, and urine samples from another series of UCs patients (BCa, renal pelvic and ureter (UC)) who had undergone cystectomy, TUR-BT or nephrouretectomy, between 2008 and 2010. Moreover, they collected urine samples from 49 health volunteers and 25 urine samples from patients with urinary tract infections (UTIs). They tested miR-96, miR-183 and miR-190 which appeared upregulated in a previous study based on urine from UC patients (83). Urinary concentration of miR-190 presented no clinically significant difference between patients and controls, while miR-96 and miR-183 were significantly higher in UCs patients than controls or UTI samples (p<0.006) (84).
Matsuzaki et al. analysed, in 2017, urinary sample of 36 patients diagnosed with UC, and 24 controls (defined as without history of UC), and selected 5 miRNAs that showed a more than 2.5-fold higher expression and p-value <0.1 in urinary extracellular vesicles of UC patients, compared to those of healthy volunteers. The authors identified miR-155-5p, miR-15a-5p, miR-21-5p, miR-132-3p and miR-31-5p as all significantly more expressed in urinary extracellular vesicles of UC patients compared to those of the control (all p<0.0001). Through a logistic multivariate analyses, the authors found that miR-21-5p was the most important predictor of UC (AUC=0.900) and could be a candidate to early diagnosis of UC even in patients with negative urine cytology (85).
4. Materials and methods
A systematic review of the literature was performed in March 2023 using the PubMed®, Scopus®, Web of Science®, Clinical trial.gov, Cochrane Library® databases [MEDLINE, EMBASE, and Web of Science databases]. Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) recommendations were followed to design the search strategies, selection criteria, and evidence report. The International Prospective Register of Systematic Review (PROSPERO) protocol number is CRD42023402737. Patient-related and intervention search terms were combined to build the following search string: [(urinary miRNA) AND (prostate cancer); (urinary miRNA) AND (bladder cancer); (urinary miRNA) AND (renal cancer); (urinary miRNA) AND (testicular cancer); (urinary miRNA) AND (urothelial cancer)].
Search results were filtered by language (English only), species (human), publication type (article). Study eligibility was defined using the PICOS (patient, intervention, comparator, outcome, study type) approach. Inclusion criteria were:
(P) studies focused on adults (>18 yr of age) with a diagnosis of kidney, bladder, or prostate cancers.
(I) identification of miRNAs as diagnostic biomarkers.
(C) in which controls as healthy subjects were used as a comparator.
(O) evaluating one or more of the following outcomes: in the diagnosis, prognosis, and therapy of urological cancers.
(S) retrospective or prospective comparative studies, with a minimum cohort size of 10 patients.
Exclusion criteria were: (1) SP on animal or cadaveric models; (2) studies reporting fewer than five cases; and (3) non-original studies including editorial comments, meeting abstracts, case reports, or letters to the editor or any form of grey literature because of the general lack of details or peer review.
5. Conclusions
The development of brand-new diagnostic tools allowing the early detection of cancers is still evolving in the everyday clinical research. In this context, urinary miRNA are emerging as important and reliable tools which could help physicians in the diagnosis, prognosis, and in the therapeutic management of urological cancers.
Author Contributions
Conceptualization, S.D.P., A.A., and S.C.; methodology, F.L., P.V., M.F.; formal analysis, A.F., F.D.G..; investigation, R.C., G.S., L.N., and C.M.; data curation, C.C., F.C.; writing—original draft preparation, A.A., S.C.; writing—review and editing, R.N., A.S, G.L.; supervision, S.D.P., J.W., A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available in scientific databases.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tian YQ, Yang JC, Hu JJ, Ding R, Ye DW, Shang JW. Trends and risk factors of global incidence, mortality, and disability of genitourinary cancers from 1990 to 2019: Systematic analysis for the Global Burden of Disease Study 2019. Front Public Health. 2023 Feb 22;11:1119374. [CrossRef]
- Tölle A, Blobel CC, Jung K. Circulating miRNAs in blood and urine as diagnostic and prognostic biomarkers for bladder cancer: an update in 2017. Biomarkers in Medicine. 2018 Jun;12(6):667–76. [CrossRef]
- Oliveira MCD, Caires HR, Oliveira MJ, Fraga A, Vasconcelos MH, Ribeiro R. Urinary Biomarkers in Bladder Cancer: Where Do We Stand and Potential Role of Extracellular Vesicles. Cancers. 2020 May 29;12(6):1400. [CrossRef]
- Gharib AF, Eed EM, Khalifa AS, Raafat N, Shehab-Eldeen S, Alwakeel HR, et al. Value of Serum miRNA-96-5p and miRNA-99a-5p as Diagnostic Biomarkers for Hepatocellular Carcinoma. IJGM. 2022 Mar;Volume 15:2427–36. [CrossRef]
- Visone R, Croce CM. MiRNAs and Cancer. The American Journal of Pathology. 2009 Apr;174(4):1131–8. [CrossRef]
- Wu Z, Chen Q, Qu L, Li M, Wang L, Mir MC, et al. Adverse Events of Immune Checkpoint Inhibitors Therapy for Urologic Cancer Patients in Clinical Trials: A Collaborative Systematic Review and Meta-analysis. European Urology. 2022 Apr;81(4):414–25. [CrossRef]
- Ali Syeda Z, Langden SSS, Munkhzul C, Lee M, Song SJ. Regulatory Mechanism of MicroRNA Expression in Cancer. IJMS. 2020 Mar 3;21(5):1723. [CrossRef]
- Taheri M, Shirvani-Farsani Z, Ghafouri-Fard S, Omrani MD. Expression profile of microRNAs in bladder cancer and their application as biomarkers. Biomedicine & Pharmacotherapy. 2020 Nov;131:110703. [CrossRef]
- Endzeliņš E, Melne V, Kalniņa Z, Lietuvietis V, Riekstiņa U, Llorente A, et al. Diagnostic, prognostic and predictive value of cell-free miRNAs in prostate cancer: a systematic review. Mol Cancer. 2016 Dec;15(1):41. [CrossRef]
- Halaseh SA, Halaseh S, Alali Y, Ashour ME, Alharayzah MJ. A Review of the Etiology and Epidemiology of Bladder Cancer: All You Need To Know. Cureus [Internet]. 2022 Jul 27 [cited 2023 May 4]; Available from: https://www.cureus.com/articles/105534-a-review-of-the-etiology-and-epidemiology-of-bladder-cancer-all-you-need-to-know.
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA A Cancer J Clinicians. 2022 Jan;72(1):7–33. [CrossRef]
- Babjuk M, Burger M, Capoun O, Cohen D, Compérat EM, Dominguez Escrig JL, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur Urol. 2022 Jan;81(1):75–94. [CrossRef]
- Aveta A, Cacciapuoti C, Barone B, Di Zazzo E, Del Giudice F, Maggi M, et al. The Impact of Meat Intake on Bladder Cancer Incidence: Is It Really a Relevant Risk? Cancers. 2022 Sep 29;14(19):4775. [CrossRef]
- Babjuk M, Burger M, Compérat EM, Gontero P, Mostafid AH, Palou J, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ) - 2019 Update. European Urology. 2019 Nov;76(5):639–57. [CrossRef]
- Calace FP, Napolitano L, Arcaniolo D, Stizzo M, Barone B, Crocetto F, et al. Micro-Ultrasound in the Diagnosis and Staging of Prostate and Bladder Cancer: A Comprehensive Review. Medicina. 2022 Nov 10;58(11):1624. [CrossRef]
- Di Meo NA, Loizzo D, Pandolfo SD, Autorino R, Ferro M, Porta C, et al. Metabolomic Approaches for Detection and Identification of Biomarkers and Altered Pathways in Bladder Cancer. IJMS. 2022 Apr 10;23(8):4173. [CrossRef]
- Kim SM, Kang HW, Kim WT, Kim YJ, Yun SJ, Lee SC, et al. Cell-Free microRNA-214 From Urine as a Biomarker for Non-Muscle-Invasive Bladder Cancer. Korean J Urol. 2013;54(11):791. [CrossRef]
- Zhang X, Zhang Y, Liu X, Fang A, Wang J, Yang Y, et al. Direct quantitative detection for cell-free miR-155 in urine: a potential role in diagnosis and prognosis for non-muscle invasive bladder cancer. Oncotarget. 2016 Jan 19;7(3):3255–66. [CrossRef]
- Zhang P, Bill K, Liu J, Young E, Peng T, Bolshakov S, et al. MiR-155 Is a Liposarcoma Oncogene That Targets Casein Kinase-1α and Enhances β-Catenin Signaling. Cancer Research. 2012 Apr 1;72(7):1751–62. [CrossRef]
- Piao XM, Jeong P, Kim YH, Byun YJ, Xu Y, Kang HW, et al. Urinary cell-free microRNA biomarker could discriminate bladder cancer from benign hematuria: Urinary cell-free microRNA biomarker. Int J Cancer. 2019 Jan 15;144(2):380–8. [CrossRef]
- Huang X, Zhao H, Qian X, Qiu J. MiR-20a in cell-free urine as a potential diagnostic biomarker for non-muscle invasive bladder cancer: a Chinese population-based study. Int J Clin Exp Med. 11(1):209–16.
- Sasaki H, Yoshiike M, Nozawa S, Usuba W, Katsuoka Y, Aida K, et al. Expression Level of Urinary MicroRNA-146a-5p Is Increased in Patients With Bladder Cancer and Decreased in Those After Transurethral Resection. Clinical Genitourinary Cancer. 2016 Oct;14(5):e493–9. [CrossRef]
- Andreu Z, Otta Oshiro R, Redruello A, López-Martín S, Gutiérrez-Vázquez C, Morato E, et al. Extracellular vesicles as a source for non-invasive biomarkers in bladder cancer progression. European Journal of Pharmaceutical Sciences. 2017 Feb;98:70–9. [CrossRef]
- Baumgart S, Meschkat P, Edelmann P, Heinzelmann J, Pryalukhin A, Bohle R, et al. MicroRNAs in tumor samples and urinary extracellular vesicles as a putative diagnostic tool for muscle-invasive bladder cancer. J Cancer Res Clin Oncol. 2019 Nov;145(11):2725–36. [CrossRef]
- Yun SJ, Jeong P, Kim WT, Kim TH, Lee YS, Song PH, et al. Cell-free microRNAs in urine as diagnostic and prognostic biomarkers of bladder cancer. International Journal of Oncology. 2012 Nov;41(5):1871–8. [CrossRef]
- abdel-Hafiz S, Sherif H, Romeih M, Elesaily K. Urine micro-RNA signature as a potential non-invasive diagnostic biomarker in bladder cancer. Asian Pac J Cancer Prev. 2023 Jan 1;24(1):121–31. [CrossRef]
- Mengual L, Lozano JJ, Ingelmo-Torres M, Gazquez C, Ribal MJ, Alcaraz A. Using microRNA profiling in urine samples to develop a non-invasive test for bladder cancer: miRNA profiling in urine samples. Int J Cancer. 2013 May;n/a-n/a. [CrossRef]
- Ghorbanmehr N, Gharbi S, Korsching E, Tavallaei M, Einollahi B, Mowla SJ. miR-21-5p, miR-141-3p, and miR-205-5p levels in urine-promising biomarkers for the identification of prostate and bladder cancer. Prostate. 2019 Jan;79(1):88–95. [CrossRef]
- Hofbauer SL, De Martino M, Lucca I, Haitel A, Susani M, Shariat SF, et al. A urinary microRNA (miR) signature for diagnosis of bladder cancer. Urologic Oncology: Seminars and Original Investigations. 2018 Dec;36(12):531.e1-531.e8. [CrossRef]
- Pardini B, Cordero F, Naccarati A, Viberti C, Birolo G, Oderda M, et al. microRNA profiles in urine by next-generation sequencing can stratify bladder cancer subtypes. Oncotarget. 2018 Apr 17;9(29):20658–69. [CrossRef]
- Braicu C, Buiga R, Cojocneanu R, Buse M, Raduly L, Pop LA, et al. Connecting the dots between different networks: miRNAs associated with bladder cancer risk and progression. J Exp Clin Cancer Res. 2019 Dec;38(1):433. [CrossRef]
- Cantley LC. The Phosphoinositide 3-Kinase Pathway. Science. 2002 May 31;296(5573):1655–7. [CrossRef]
- Lin JT, Tsai KW. Circulating miRNAs Act as Diagnostic Biomarkers for Bladder Cancer in Urine. IJMS. 2021 Apr 20;22(8):4278. [CrossRef]
- Moisoiu T, Dragomir MP, Iancu SD, Schallenberg S, Birolo G, Ferrero G, et al. Combined miRNA and SERS urine liquid biopsy for the point-of-care diagnosis and molecular stratification of bladder cancer. Mol Med. 2022 Dec;28(1):39. [CrossRef]
- Long JD, Sullivan TB, Humphrey J, Logvinenko T, Summerhayes KA, Kozinn S, et al. A non-invasive miRNA based assay to detect bladder cancer in cell-free urine. Am J Transl Res. 2015;7(11):2500–9.
- Sun DK, Wang JM, Zhang P, Wang YQ. MicroRNA-138 Regulates Metastatic Potential of Bladder Cancer Through ZEB2. Cell Physiol Biochem. 2015;37(6):2366–74. [CrossRef]
- Yang R, Liu M, Liang H, Guo S, Guo X, Yuan M, et al. miR-138-5p contributes to cell proliferation and invasion by targeting Survivin in bladder cancer cells. Mol Cancer. 2016 Dec;15(1):82. [CrossRef]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J Clin. 2021 May;71(3):209–49. [CrossRef]
- Merriel SW, Seggie A, Ahmed H. Diagnosis of prostate cancer in primary care: navigating updated clinical guidance. Br J Gen Pract. 2023 Feb;73(727):54–5. [CrossRef]
- Sekhoacha M, Riet K, Motloung P, Gumenku L, Adegoke A, Mashele S. Prostate Cancer Review: Genetics, Diagnosis, Treatment Options, and Alternative Approaches. Molecules. 2022 Sep 5;27(17):5730. [CrossRef]
- Kasivisvanathan V, Rannikko AS, Borghi M, Panebianco V, Mynderse LA, Vaarala MH, et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018 May 10;378(19):1767–77. [CrossRef]
- M. Hafron J, Yu H, Juang A, Vuong D, Kamer S, Carbonell L, et al. New developments in prostate cancer screening using a novel cancer-specific, non-PSA biomarker assay derived from autoantibody signatures. J Med Therap [Internet]. 2017 [cited 2023 Apr 27];1(4). Available from: http://www.oatext.com/new-developments-in-prostate-cancer-screening-using-a-novel-cancer-specific-non-psa-biomarker-assay-derived-from-autoantibody-signatures.php. [CrossRef]
- Di Minno A, Aveta A, Gelzo M, Tripodi L, Pandolfo SD, Crocetto F, et al. 8-Hydroxy-2-Deoxyguanosine and 8-Iso-Prostaglandin F2α: Putative Biomarkers to assess Oxidative Stress Damage Following Robot-Assisted Radical Prostatectomy (RARP). JCM. 2022 Oct 17;11(20):6102. [CrossRef]
- Luca LD, Crocetto F, Barone B, Creta M, Pesce S, Aveta A, et al. Granulomatous prostatitis mimicking prostate cancer in a patient with psoriatic arthritis: a case report. Future Science OA. 2020 Aug 1;6(7):FSO591. [CrossRef]
- Pandolfo SD, Crauso F, Aveta A, Cilio S, Barone B, Napolitano L, et al. A Novel Low-Cost Uroflowmetry for Patient Telemonitoring. IJERPH. 2023 Feb 13;20(4):3287. [CrossRef]
- Schaefer A, Jung M, Mollenkopf HJ, Wagner I, Stephan C, Jentzmik F, et al. Diagnostic and prognostic implications of microRNA profiling in prostate carcinoma. Int J Cancer. 2009;NA-NA. [CrossRef]
- Stephan C, Jung M, Rabenhorst S, Kilic E, Jung K. Urinary miR-183 and miR-205 do not surpass PCA3 in urine as predictive markers for prostate biopsy outcome despite their highly dysregulated expression in prostate cancer tissue. Clinical Chemistry and Laboratory Medicine (CCLM) [Internet]. 2015 Jan 1 [cited 2023 Apr 27];53(7). Available from: https://www.degruyter.com/document/doi/10.1515/cclm-2014-1000/html. [CrossRef]
- Salido-Guadarrama AI, Morales-Montor JG, Rangel-Escareño C, Langley E, Peralta-Zaragoza O, Colin JLC, et al. Urinary microRNA-based signature improves accuracy of detection of clinically relevant prostate cancer within the prostate-specific antigen grey zone. Molecular Medicine Reports. 2016 Jun;13(6):4549–60. [CrossRef]
- Leite KRM, Tomiyama A, Reis ST, Sousa-Canavez JM, Sañudo A, Camara-Lopes LH, et al. MicroRNA expression profiles in the progression of prostate cancer—from high-grade prostate intraepithelial neoplasia to metastasis. Urologic Oncology: Seminars and Original Investigations. 2013 Aug;31(6):796–801. [CrossRef]
- Porkka KP, Pfeiffer MJ, Waltering KK, Vessella RL, Tammela TLJ, Visakorpi T. MicroRNA Expression Profiling in Prostate Cancer. Cancer Research. 2007 Jul 1;67(13):6130–5. [CrossRef]
- Rodríguez M, Bajo-Santos C, Hessvik NP, Lorenz S, Fromm B, Berge V, et al. Identification of non-invasive miRNAs biomarkers for prostate cancer by deep sequencing analysis of urinary exosomes. Mol Cancer. 2017 Dec;16(1):156. [CrossRef]
- Nadiminty N, Tummala R, Lou W, Zhu Y, Shi XB, Zou JX, et al. MicroRNA let-7c Is Downregulated in Prostate Cancer and Suppresses Prostate Cancer Growth. Das GM, editor. PLoS ONE. 2012 Mar 30;7(3):e32832. [CrossRef]
- Foj L, Ferrer F, Serra M, Arévalo A, Gavagnach M, Giménez N, et al. Exosomal and Non-Exosomal Urinary miRNAs in Prostate Cancer Detection and Prognosis: Urinary miRNAs in Prostate Cancer. Prostate. 2017 May;77(6):573–83. [CrossRef]
- Markert L, Holdmann J, Klinger C, Kaufmann M, Schork K, Turewicz M, et al. Small RNAs as biomarkers to differentiate benign and malign prostate diseases: An alternative for transrectal punch biopsy of the prostate? Lobaccaro JMA, editor. PLoS ONE. 2021 Mar 24;16(3):e0247930. [CrossRef]
- Tian L, Fang Y xiang, Xue J lun, Chen J zhong. Four microRNAs promote prostate cell proliferation with regulation of PTEN and its downstream signals in vitro. PLoS One. 2013;8(9):e75885. [CrossRef]
- Hasanoğlu S, Göncü B, Yücesan E, Atasoy S, Kayali Y, Özten Kandaş N. Investigating differential miRNA expression profiling using serum and urine specimens for detecting potential biomarkers for early prostate cancer diagnosis. Turk J Med Sci. 2021 Aug 30;51(4):1764–74. [CrossRef]
- Byun YJ, Piao XM, Jeong P, Kang HW, Seo SP, Moon SK, et al. Urinary microRNA-1913 to microRNA-3659 expression ratio as a non-invasive diagnostic biomarker for prostate cancer. Investig Clin Urol. 2021;62(3):340. [CrossRef]
- Kang HW, Byun YJ, Moon SM, Kim K, Piao XM, Zheng CM, et al. Urinary hsv2-miR-H9 to hsa-miR-3659 ratio is an effective marker for discriminating prostate cancer from benign prostate hyperplasia in patients within the prostate-specific antigen grey zone. Investig Clin Urol. 2022;63(2):238. [CrossRef]
- Lee H, Kang SJ, Lee J, Park KH, Rhee WJ. Isolation and Characterization of Urinary Extracellular Vesicles from Healthy Donors and Patients with Castration-Resistant Prostate Cancer. IJMS. 2022 Jun 27;23(13):7134. [CrossRef]
- Zennami K, Choi SM, Liao R, Li Y, Dinalankara W, Marchionni L, et al. PDCD4 Is an Androgen-Repressed Tumor Suppressor that Regulates Prostate Cancer Growth and Castration Resistance. Molecular Cancer Research. 2019 Feb 1;17(2):618–27. [CrossRef]
- Ashraf NM, Imran K, Kastner DW, Ikram K, Mushtaq A, Hussain A, et al. Potential involvement of mi-RNA 574-3p in progression of prostate cancer: A bioinformatic study. Molecular and Cellular Probes. 2017 Dec;36:21–8. [CrossRef]
- Capitanio U, Bensalah K, Bex A, Boorjian SA, Bray F, Coleman J, et al. Epidemiology of Renal Cell Carcinoma. Eur Urol. 2019 Jan;75(1):74–84. [CrossRef]
- Cinque A, Vago R, Trevisani F. Circulating RNA in Kidney Cancer: What We Know and What We Still Suppose. Genes (Basel). 2021 May 28;12(6):835. [CrossRef]
- Cancer (IARC) TIA for R on. Global Cancer Observatory [Internet]. [cited 2023 Apr 15]. Available from: https://gco.iarc.fr/.
- Ljungberg B, Albiges L, Abu-Ghanem Y, Bedke J, Capitanio U, Dabestani S, et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. European Urology. 2022 Oct;82(4):399–410. [CrossRef]
- Napolitano L, Manfredi C, Cirillo L, Fusco GM, Passaro F, Abate M, et al. Cytoreductive Nephrectomy and Metastatic Renal Cell Carcinoma: State of the Art and Future Perspectives. Medicina. 2023 Apr 15;59(4):767. [CrossRef]
- Lasorsa F, Di Meo NA, Rutigliano M, Milella M, Ferro M, Pandolfo SD, et al. Immune Checkpoint Inhibitors in Renal Cell Carcinoma: Molecular Basis and Rationale for Their Use in Clinical Practice. Biomedicines. 2023 Apr 2;11(4):1071. [CrossRef]
- Di Meo NA, Lasorsa F, Rutigliano M, Loizzo D, Ferro M, Stella A, et al. Renal Cell Carcinoma as a Metabolic Disease: An Update on Main Pathways, Potential Biomarkers, and Therapeutic Targets. IJMS. 2022 Nov 18;23(22):14360. [CrossRef]
- Cui C, Cui Q. The relationship of human tissue microRNAs with those from body fluids. Sci Rep. 2020 Mar 27;10(1):5644. [CrossRef]
- von Brandenstein M, Pandarakalam JJ, Kroon L, Loeser H, Herden J, Braun G, et al. MicroRNA 15a, inversely correlated to PKCα, is a potential marker to differentiate between benign and malignant renal tumors in biopsy and urine samples. Am J Pathol. 2012 May;180(5):1787–97. [CrossRef]
- Mlcochova H, Hezova R, Stanik M, Slaby O. Urine microRNAs as potential noninvasive biomarkers in urologic cancers. Urol Oncol. 2014 Jan;32(1):41.e1-9. [CrossRef]
- Liu Q, Shin Y, Kee JS, Kim KW, Mohamed Rafei SR, Perera AP, et al. Corrigendum to “Mach-Zehnder interferometer (MZI) point-of-care system for rapid multiplexed detection of microRNAs in human urine specimens” [Biosens. Bioelectron. 71 (2015) 365-372]. Biosens Bioelectron. 2016 Nov 15;85:996. [CrossRef]
- Fedorko M, Juracek J, Stanik M, Svoboda M, Poprach A, Buchler T, et al. Detection of let-7 miRNAs in urine supernatant as potential diagnostic approach in non-metastatic clear-cell renal cell carcinoma. Biochem Med (Zagreb). 2017 Jun 15;27(2):411–7. [CrossRef]
- Li G, Zhao A, Péoch M, Cottier M, Mottet N. Detection of urinary cell-free miR-210 as a potential tool of liquid biopsy for clear cell renal cell carcinoma. Urol Oncol. 2017 May;35(5):294–9. [CrossRef]
- Mytsyk Y, Dosenko V, Borys Y, Kucher A, Gazdikova K, Busselberg D, et al. MicroRNA-15a expression measured in urine samples as a potential biomarker of renal cell carcinoma. Int Urol Nephrol. 2018 May;50(5):851–9. [CrossRef]
- Song S, Long M, Yu G, Cheng Y, Yang Q, Liu J, et al. Urinary exosome miR-30c-5p as a biomarker of clear cell renal cell carcinoma that inhibits progression by targeting HSPA5. J Cell Mol Med. 2019 Oct;23(10):6755–65. [CrossRef]
- Cochetti G, Cari L, Nocentini G, Maulà V, Suvieri C, Cagnani R, et al. Detection of urinary miRNAs for diagnosis of clear cell renal cell carcinoma. Sci Rep. 2020 Dec 4;10(1):21290. [CrossRef]
- Ferro M, Musi G, Marchioni M, Maggi M, Veccia A, Del Giudice F, et al. Radiogenomics in Renal Cancer Management-Current Evidence and Future Prospects. Int J Mol Sci. 2023 Feb 27;24(5):4615. [CrossRef]
- von Brandenstein M, Schlosser M, Herden J, Heidenreich A, Störkel S, Fries JWU. MicroRNAs as Urinary Biomarker for Oncocytoma. Dis Markers. 2018;2018:6979073. [CrossRef]
- Di Meo A, Brown MD, Finelli A, Jewett MAS, Diamandis EP, Yousef GM. Prognostic urinary miRNAs for the assessment of small renal masses. Clin Biochem. 2020 Jan;75:15–22. [CrossRef]
- Rouprêt M, Seisen T, Birtle AJ, Capoun O, Compérat EM, Dominguez-Escrig JL, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. European Urology. 2023 Mar;S0302283823026520. [CrossRef]
- Wu Z, Li M, Wang L, Paul A, Raman JD, Necchi A, et al. Neoadjuvant systemic therapy in patients undergoing nephroureterectomy for urothelial cancer: a multidisciplinary systematic review and critical analysis. Minerva Urol Nephrol [Internet]. 2022 Sep [cited 2023 May 8];74(5). Available from: https://www.minervamedica.it/index2.php?show=R19Y2022N05A0518. [CrossRef]
- Chiyomaru T, Enokida H, Tatarano S, Kawahara K, Uchida Y, Nishiyama K, et al. miR-145 and miR-133a function as tumour suppressors and directly regulate FSCN1 expression in bladder cancer. Br J Cancer. 2010 Mar 2;102(5):883–91. [CrossRef]
- Yamada Y, Enokida H, Kojima S, Kawakami K, Chiyomaru T, Tatarano S, et al. MiR-96 and miR-183 detection in urine serve as potential tumor markers of urothelial carcinoma: correlation with stage and grade, and comparison with urinary cytology. Cancer Sci. 2011 Mar;102(3):522–9. [CrossRef]
- Matsuzaki K, Fujita K, Jingushi K, Kawashima A, Ujike T, Nagahara A, et al. MiR-21-5p in urinary extracellular vesicles is a novel biomarker of urothelial carcinoma. Oncotarget. 2017 Apr 11;8(15):24668–78. [CrossRef]
Figure 1.
Prisma Flow Chart – Study selection with inclusion and exclusion criteria of reviewed studies.
Figure 1.
Prisma Flow Chart – Study selection with inclusion and exclusion criteria of reviewed studies.
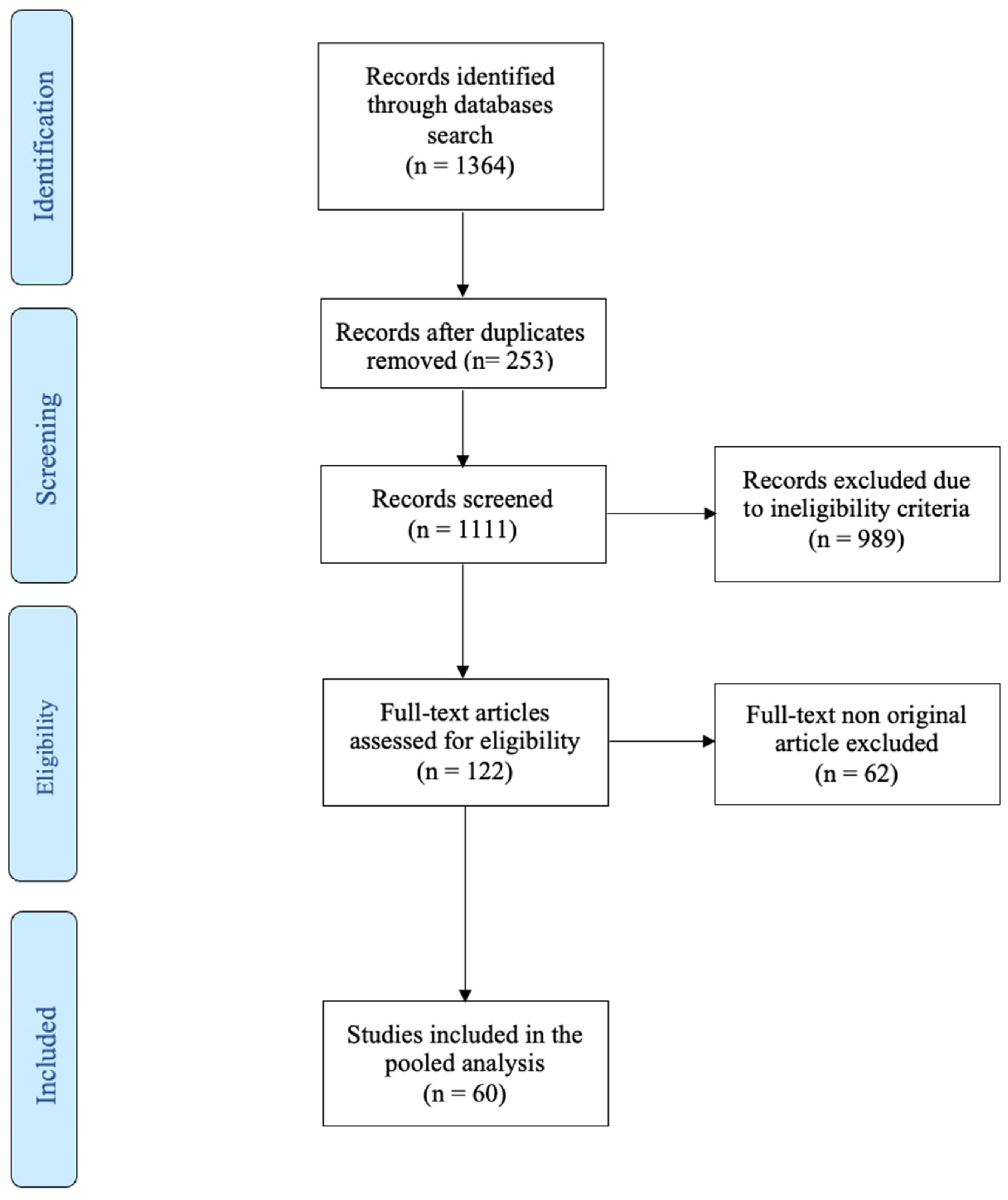

Table 1.
Characteristics of the included studies of bladder cancer classified according to year of publication (2023-2012).
Table 1.
Characteristics of the included studies of bladder cancer classified according to year of publication (2023-2012).
| Authors | Year of Publication |
Number of Patients (BC/Ctl) |
Study Design | Target (microRNA in PCa) |
Primary Findings |
|---|---|---|---|---|---|
| Mamdouh et al. | 2023 | 111/25 |
Retrospective |
miR-200 (↑) miR-145 (↑) miR-21(↑) |
Positive correlation (p=0.02) high and low grade > controls (p=0.01) high and low grade > controls (p=0.05) high and low grade > controls |
| Moisoiu et al. | 2022 | 15/16 |
Retrospective |
Panel of three miRNAs: miR-34a-5p (↑) miR-205-5p (↑) miR-210-3p (↑) |
AUC 0.92 (miRNA + SERS) |
| Lin et al. | 2021 | 180/100 |
Retrospective |
let-7c-5p (↑) miR-146a-5p (↑) miR-149-5p (↑) miR-193a-5p (↑) miR-423-5p (↑) |
Positive correlation BC > Ctl |
| Baugmart et al. | 2019 | 37/0 |
Retrospective |
miR-146 (↑) | Positive correlation High grade > low grade |
| Braicu et al. | 2019 | 23/23 |
Retrospective |
miR-141-3p (↑) miR-205-5p (↑) miR-139-5p (↓) miR-143-5p (↓) miR-200b-3p (↑) |
AUC 0.86 (overall) AUC 0.89 (overall) BC < Ctl BC < Ctl BC > Ctl |
| Pardini et al. | 2018 | 66/48 |
Retrospective |
Panel of three miRNAs: let-7c-5p (↑) miR-30a-5p (↑) miR-486-5p (↓) |
AUC 0.70 (overall) AUC 0.73 (low-grade NMIBC) AUC 0.95 (high-grade NMIBC) AUC 0.99 (MIBC) |
| Huang et al. | 2018 | 80/86 |
Retrospective |
miR-20a (↑) |
Positive correlation (p<0.001) Associated with larger tumour size and advanced tumour grade in NMIBC (all p<0.05) |
| Ghorbanmehr et al. | 2018 | 45/20 |
Retrospective |
miR-21-5p (↑) miR141-3p (↑) mir205-5p (↑) |
Positive correlation 84% SN, 59% SP; AUC 0.76 (overall) 71% SN, 71% SP; AUC 0.74 (overall) 82% SN, 62% SP; AUC 0.73 (overall) |
| Piao et al. | 2018 | 35/20 |
Retrospective |
miR-6124 to miR-4511 ratio (↑) | Positive correlation (AUC: 0.888, 91.5% SN, 76.2% SP) (p < 0.001) |
| Hofbauer et al. | 2018 | 87/115 |
Retrospective |
Panel of six miRNAs: Let-7c (↓) miR-135a (↓) miR-135b (↑) miR-148a (↓) miR-204 (↓) miR-345 (↑) |
AUC 0.88 (overall) AUC 0.91 (MIBC) |
| Andreu et al. | 2017 | 36/9 | Retrospective | miR-146 (↑) | Low grade > high grade |
| Sasaki et al. | 2016 | 28/19 | Retrospective | miR-146a-5p (↑) | Positive correlation (AUC=0.773,95% CI, 0.701-0.892) (p=0.014) (p=0.0436) (high-grade > low-grade) (p=0.1391) (MIBC > NMIBC) |
| Zhang et al. | 2016 | 162/162 | Retrospective |
miR-155 (↑) | Positive correlation (AUC=0.804; 95% CI, 0.756-0.845,80.2% SN, 84.6% SP )(NMIBC) |
| Kim et al. | 2013 | 138/144 | Retrospective | miR-214 (↑) | Positive correlation 20.08±3.21 vs. 18.96±2.68, (p=0.002) (NMIBC) |
| Mengual et al. | 2013 | 181/136 | Retrospective | Panel of six miRNAs: miR-18a (↑) miR-25 (↑) miR-140-5p (↓) miR-187 (↑) miR-142-3p (↓) miR-204 (↓) |
84.8% SN, 86.5% SP; AUC 0.92 (overall) 87.1% SN, 86.5% SP (MIBC) |
| Yun et al. | 2012 | 207/144 |
Retrospective |
miR-145 (↓) miR-200a (↓) |
Negative correlation miR-145 (AUC=0.729;77.8% SN, 61.1% SP) (NMIBC < healthy controls) miR-145 (AUC=0.79;84.1% SN, 61.1% SP) (MIBC < healthy controls) miR-145 (p=0.036) (MIBC<NMIBC) miR-200a (p<0.001) (MIBC and NMIBC<healthy controls) |
Abbreviations: BC: bladder cancer; Ctl: control participants; NMIBC: non-muscle-invasive bladder cancer; AUC: area under the curve; CI: confidence interval; p: p-value; SN: sensitivity; SP: specificity; SERS: surface-enhanced Raman spectroscopy.
Table 2.
Characteristics of the included studies of prostate cancer classified according to year of publication (2022-2015).
Table 2.
Characteristics of the included studies of prostate cancer classified according to year of publication (2022-2015).
| Authors | Year of Publication |
Number of Patients (PCa/Ctl) |
Study Design | Target (microRNA in PCa) |
Primary Findings |
|---|---|---|---|---|---|
| Lee et al. | 2022 | 6/8 | Retrospective | miR-21-5p, miR-574-3p, and miR6880-5p (↑) | Positive correlation in CRPC miR-21-5p, miR-574-3p (p <0.05) miR6880-5p (p <0.01) |
| Kang et al. | 2022 | 63/53 | Retrospective | miR-H9 to miR-3659 ratio (↑) | Positive correlation (AUC=0.803,95% CI) (p= 0.001) |
| Byun et al. | 2021 | 14/5 | Retrospective | miR-1913 to miR-3659 ratio (↑) | Positive correlation (AUC=0.7,95% CI, 61.4% SN, 71.8% SP) |
| Hasanoglu et al. | 2021 | 8/30 | Retrospective | miR-320a (↑) | Positive correlation p=0.0168 |
| Markert et al. | 2021 | 28/25 | Retrospective | miR-19b and miR-26a (↓) | Negative correlation AUC=0.7 |
| Ghorbanmehr et al. | 2020 | 23/42 | Retrospective | miR-21-5p (↑) mi-R-141-3p (↑) miR-205p (↑) |
Positive correlation p=0.001 p=0.005 p=0.020 |
| Foj et al. | 2017 | 60/10 | Retrospective | miR-21, miR-141, and miR-375 (↑) let-7c |
Positive correlation miR-21 (p=0.001) miR-141(p=0.033); higher Gleason score (p=0.034) miR-375 (p=0.038) let-7c (no correlation) |
| Rodriguez et al. | 2017 | 28/19 | Retrospective | miR-196a-5p and miR-501-3p (↓) | Negative correlation miR-196a-5p (AUC=0.73,95% CI 0.56 to 0.86) miR-501-3p (AUC=0.69%, 95% CI 0.52 to 0.85) |
| Salido-Guadarrama et al. | 2016 | 73/70 | Retrospective | miR-100 and miR-200b (↑) | Positive correlation (p=0.0355; Spearman coefficient=0.18) |
| Stephan et al. | 2015 | 38/38 | Retrospective | miR-183 and miR-205 | No correlation |
Abbreviations: PCa: prostate cancer; Ctl: control participants; AUC=area under the curve; CI= confidence interval; p= p-value; SN= sensitivity; SP=specificity; CRPC= castration-resistant prostate cancer.
Table 3.
Characteristics of the included studies of Renal cancer classified according to year of publication (2020-2012).
Table 3.
Characteristics of the included studies of Renal cancer classified according to year of publication (2020-2012).
| Authors | Year of Publication |
Number of Patients (RCC/Ctl) |
Study design | Target (microRNA in RCC) |
Primary Findings |
|---|---|---|---|---|---|
| Di Meo et al. | 2020 | 6/8 | Retrospective | miR-432-5p and miR-532-5p (↑↑) miR-10a-5p, miR-144-3p, miR-28-3p, miR-326, miR-328-3p, miR-603, and miR-93-3p (↑) |
Positive correlation miR-432-5p (AUC: 0.71, 95% CI: 0.59 to 0.83, p=0.003) miR-532-5p (AUC: 0.70, 95%CI: 0.57–0.82, p=0.007) miR-10a-5p (AUC: 0.66, 95% CI: 0.53–0.79) miR-144-3p (AUC: 0.68, 95% CI: 0.55–0.81) miR-28-3p (AUC: 0.65, 95% CI: 0.52–0.78) miR-326 (AUC: 0.68, 95% CI: 0.55–0.81) miR-328-3p (AUC: 0.65, 95% CI: 0.52–0.78) miR-603 (AUC: 0.67, 95% CI: 0.55–0.80), and miR-93-3p (AUC: 0.68, 95% CI: 0.54–0.81), all p<0.05 |
| Cochetti et al. | 2020 | 13/14 | Retrospective | Panel of: miR-122, miR-1271, miR-15b (↑) |
(100% SN (95% CI 75–100%), and 86% SP (95% CI 57–98%), AUC of 0.96 and p<0.001) |
| Song et al. | 2019 | 70/30 | Retrospective | miR-30c-5p (↓) | Negative correlation (68.57% SN and 100%SP) |
| von Brandenstein et al. | 2018 | 26/17 | Retrospective | miR-498, miR-183, miR-205, and miR-31(↑) | Positive correlation with Oncocytoma |
| Mytsyk et al. | 2018 | 67/15 | Retrospective | miR-15a (↑) | Positive correlation between miR-15a levels and tumour size (98.1% SP, 100% SN, AUC=0.955, p<0.001) |
| Li et al. | 2017 | 75/45 | Retrospective | miR-210 (↑) | Positive correlation P<0.001 (SN of 57.8% and SP of 80.0%) |
| Fedorko et al. | 2017 | 69/36 | Retrospective | all let-7 miRNAs (let-7a, let-7b, let-7c, let-7d, let-7e and let-7g (↑) | Positive correlation (AUC=0.8307, 71% SN, 81% SP), all p<0.05. |
| von Brandenstein et al. | 2012 | 25/5 | Retrospective | miR-15a (↑) | Positive correlation (p not reported) |
Abbreviations: RCC: Renal Cell Carcinoma; Ctl: control participants; AUC=area under the curve; CI= confidence interval; p= p-value; SN= sensitivity; SP=specificity.
Table 4.
Characteristics of the included studies of Upper Tract urothelial carcinoma classified according to year of publication (2017-2011).
Table 4.
Characteristics of the included studies of Upper Tract urothelial carcinoma classified according to year of publication (2017-2011).
| Authors | Year of Publication |
Number of Patients (UTUC/Ctl) |
Study design | Target (microRNA in UTUC) |
Primary Findings |
|---|---|---|---|---|---|
| Matsuzaki et al. | 2017 | 36/26 | Retrospective | miR-155-5p, miR-15a-5p, miR-21-5p, miR-132-3p and miR-31-5p (↑) | Positive correlation in UTUC (all p<0.001) miR-21-5p (AUC=0.900) |
| Yamada et al. | 2011 | <104/74 | Retrospective | miR-190 (=) miR-96 and miR-183 (↑) |
Positive correlation (p=0.006) |
Abbreviations: UTUC: Upper Tract Urothelial Carcinoma; Ctl: control participants; AUC=area under the curve; CI= confidence interval; p= p-value; SN= sensitivity; SP=specificity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



