
Submitted:
29 April 2023
Posted:
29 April 2023
You are already at the latest version
Abstract
The sustainable development goals(SDG) of the UNO would be difficult to achieve without prevention of metabolic diseases and other non-communicable diseases (NCDs). Western diet and lifestyle, which are major risk factors of NCDs, are known to cause oxidative stress and decrease in production of molecular hydrogen in the intestines which leads to a decline in endogenous antioxidant status in the body, leading to increase in systemic inflammation. Many experts consider molecular hydrogen as a potential nutrient, which may be administered as gas in the body. There are gaps in the knowledge about the role molecular hydrogen plays, in the treatment of metabolic diseases and other NCDs This review aims to discuss the role of hydrogen in the pathogenesis and prevention of NCDs. Molecular hydrogen (H2) has been studied extensively as a therapeutic gas, with an estimated 2000 publications to date, exploring its potential therapeutic use in 170 disease models across every organ in the mammalian body. Hydrogen therapy can be administered through several methods, such as H2 inhalation, dissolving H2 gas in water to make hydrogen-rich water (HRW) for oral consumption or topical application, or hydrogen-rich saline. The exact mechanism of action of molecular hydrogen is not known but it is in itself a potential antioxidant that can also inhibit hydroxyl and nitrosyl radicals in the cells and tissues. Hydrogen is known to cause a marked decline in oxidative stress, and inflammation that are crucial in the pathogenesis of NCDs. Hydrogen therapy has been found protective against NCDs, including, metabolic diseases, cardiovascular diseases (CVDs), neurodegenerative diseases, chronic kidney disease, cancer and chronic lung diseases.
Keywords:
Hydrogen
; cardiovascular
; metabolic diseases
; diet
; oxidative stress
; inflammation
Introduction
Cohort studies have demonstrated that metabolic diseases; obesity, type 2 diabetes mellitus (T2DM) and other chronic diseases; cardiovascular diseases (CVDs), cancer, osteoporosis and neurodegenerative diseases have become a public health problem in both developed and developing countries of the world [1-3]. The increase in risk of these non-communicable diseases (NCDs), may be due to western type diet, sedentary behavior, increase intake of tobacco and alcoholism [1]. Nutrition in transition from poverty to affluence may be associated with increased intake of wester foods and lower intake traditional foods with increased use of automobiles resulting in to physical inactivity leading to obesity and metabolic syndrome [1-3].
Western diet and lifestyle are known to cause obesity with an increase in the reactive oxygen species (ROS), along with possible decrease in the production of molecular hydrogen in the intestines with an accompanying decline in endogenous antioxidant status in the body, leading to an increase in systemic inflammation [4,5].The increase in oxidative stress and inflammation in the adipocytes predisposes obesity and central obesity, and increased inflammation in the beta cells of the pancreas, predisposes T2DM. Inflammation of the LDL receptors in the hepatocytes, endothelium, neurons, osteocytes and gut may predispose related NCDs; CVDs, neuro-degenerative diseases, bone and joint diseases and cancer that are major causes of mortality [6,7]. Figure 1
It seems that the existing gaps in knowledge do not allow us to understand how free radical-induced damage in the tissues and concerned organs predispose metabolic diseases and other NCDs. It is possible that increased intake of antioxidants can cause decline in free radical generation and reactive oxygen species (ROS) leading to decline in oxidative stress and inflammation [4-7]. The proposed hypothesis is that the Mediterranean type of diet which is rich in antioxidants can act as potential antioxidant, due to its protective effects on gut microbiota and increased production of molecular hydrogen, due to degradation of dietary fiber in the gut. Molecular hydrogen is known to regulate oxidative stress and inflammation and may maintain cell and tissue homeostasis, with decline in inflammation and risk of NCDs, including metabolic diseases [8-12]. The objective of this article is to highlight the role of molecular hydrogen, in the management of NCDs.
Oxidative Stress and Antioxidants in the Pathogenesis of Chronic Diseases
Several unhealthy substances and health behaviors such as western diet, fried and fast foods, alcoholism, tobacco smoke, pesticides, radiation, and pollutants can all generate free radicals [4,5,12-14]. The body tissues are under constant attack from these free radicals, because inhaled oxygen undergoes single electron reduction to form superoxide radicals (O2-). This radical can initiate radical propagation, and also be converted to hydrogen peroxide (H2O2) and hydroxyl radicals (·OH) [15]. Free oxygen radicals are characterized as having an unpaired electron, which makes them very reactive as they seek another electron to have a stable pair. These free oxygen radicals scavenge the body tissue to seek out other electrons, so they can become a pair, which causes damage to cells, proteins, lipoproteins and DNA resulting in diseases [15]. There is evidence that unhealthy diet and lifestyle may increase the production of free radicals and ROS in the tissues due to high levels of protein carbonylation and lipid peroxidation products [4,5]. There is decline in the antioxidant defense status, such as decreased production of molecular hydrogen in the gut, as well as antioxidant enzymes; in the tissues. However, certain foods as component of the Mediterranean type of diets, and nutrients, such as dietary fiber, flavonoids and omega-3 fatty acids [10], may produce protective molecules in the gut [11], such as molecular hydrogen, which is a potential free radical scavenger [12, 14].
It seems that numerous free radicals, reactive oxygen species (ROS) and reactive nitrogen species are produced due to endogenous oxidants, exposure to different physiochemical conditions or pathological processes [15]. In the physiology and metabolism, there is a need to have balance between free radical generation and antioxidant status for proper metabolic function, so that there is no increase in oxidative stress-induced cell damage resulting in to greater risk of NCDs including T2DM [8,9,12-14]. Butylated hydroxytoluene and butylated hydroxyanisole are synthetic antioxidants used as food additives to prevent peroxidation of foods that are known to be hazardous for human health [4,5,15]. Hydroxyl and nitrosyl radicals represent the major cause of the destruction of body tissues, either by a direct reaction, or by triggering a chain reaction of free radicals [4,5,15]. It seems that physiological levels of free radicals are protective for cells, hence endogenous antioxidants are crucial to prevent free radical-induced damage to tissues [4,5]. Therefore, there is a focused attention toward the role of free radical biochemistry and free radical biology. in the physiology and metabolism as well as in the pathogenesis of chronic diseases [4, 5]. There is evidence that xanthine oxidase, nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, and leakage of electron from the respiratory chain of mitochondria, are crucial in damaging the cells by superoxide radical [16,17]. These free radicals attenuate the biological presence of NO by neutralizing it via conversion to a more detrimental peroxy-nitrite radical. The oxidases that enzymatically generate H2O2 and superoxide, are accumulated in the proteins related to Nox family, the main source of vascular free radicals [16-19]. The shear stress in the vessels activates the Nox proteins; Nox 1, Nox2 and Nox3 that are considered to have crucial role in vascular function [18,19]. The superoxide radicals are particularly produced via Nox1 and Nox2 via a single transfer of electron to hydrogen molecule. The superoxide radical reacts rapidly in the cells, to inactivate excess of NO, that produces perozxynitrite, known to have adverse effects on the vasodilation induced by nitric oxide [19]. In such situations of oxidative dysfunction in the presence of peroxynitrite, it may inhibit the release of endothelial nitric oxide synthase (eNOS) enzymes causing decline in the production of NO. The cofactor of eNOS, tetrahydrobiopterin (BH4), responsible for oxidation may inactive it to, 7,8-dihydropterin (BH2), causing uncoupling of eNOS. and this mechanism, generates the superoxide. Molecular hydrogen has been found to be useful in protecting against free radical induced damage due to its potential antioxidant effects in various conditions [20-29]. However, the exact mechanisms, how molecular hydrogen protects the body tissues is not clear. Research has found that increased supplementation of molecular hydrogen can inhibit free radical generation with decline in inflammation, which may be protective against NCDs including metabolic diseases [10-15].
Physiology of Molecular Hydrogen and the Gut Microbiota
The microbiota in the gastrointestinal tract, is crucial in the prevention of NCDs including metabolic diseases. Indo-Mediterranean-style foods such as butter milk, curd and yoghurt, are used to alter the composition and improve function of the communities of the microbes that develop colonies in the gut for improvement of health, and protect from NCDs [8,9]. Increased production of molecular hydrogen is one of the important mechanisms by which healthy foods provide the beneficial effects in health and diseases [8-11]. The mechanisms by which molecular hydrogen provides the benefits are not well understood. Increased production of intestinal hydrogen along with recovery in muscle function has been reported following intensive exercises [30]. A previous study reported increased production of acetate which mediates a microbiome–brain–β- cell axis to have influence on metabolic syndrome [31]. However, increased generation of metabolites such as short chain fatty acids, BDNF and hydrogen from gut microbiota may enhance benefits in the metabolism via gut-brain neural circuits [32]. The microbes present in the gut can metabolize several of these polysaccharides into more useful fatty acids. These short-chain fatty acids (SCFAs); propionate, butyrate, acetate, and gases; methane and hydrogen have potential anti-inflammatory effects [8-11,31,32].
There are several biochemical pathways by which microbes convert the complex polysaccharides into monosaccharides, that are mediated by the enzymatic actions [32,33]. Hydrogen gas in the body is also produced through fermentation of carbohydrates; lactose, lactulose, and fructose by intestinal bacteria. The bacteria normally present in the large intestine are mainly Bacteroides fragilis group, Clostridium perfringens and Pseudomonas that possess hydrogenases to produce hydrogen. The presence of SCFAs in the gut indicates that fermentation due to microbes, occurs in the colon; with a greater level in the proximal colon but lower in the distal colon. The region of distal colon may have the highest number of microbes and with highest level of gases. Since all the Mediterranean type of diets promote the growth of gut microbiota, hydrogen is produced in liter quantities by the intestinal bacteria, in particular, if the individual has a healthy bacterial population in the gut and high fibers and probiotics in the diets [33-35].
The hydrogen production in the gastrointestinal tract in man is primarily dependent upon the delivery of ingested, fermentable fibrous substrates to an abundant intestinal flora [33]. This is normally present mainly in the colon and produce relatively large amounts of H2. The removal of excess hydrogen through methanogenesis from the gut is not the only microbial mechanism to remove excess hydrogen from the gut; this can also be mediated through the reduction of sulphate to sulphide by sulphate-reducing bacteria. At least one explanation is possible applying the pathogens that can provoke inflammation by remodeling the microbiota [34]. Certain low-abundance microbial pathogens may orchestrate inflammatory disease by remodeling a normally benign microbiota into a dysbiotic one [35]. There is evidence that, Citrobacter rodentium causes in mice global changes in microbial community structure, apparently dependent upon the ability of this pathogen to cause inflammation [35]. Induction of gut inflammation by administration of dextran sodium sulfate leading to a dysbiotic microbiota, and improvement in gut microbiom by healthy diets suggest, an intimate relationship between the inflammatory status of the intestine and gut microbiota [33-36]. Figure 2.
The research on molecular hydrogen is intensified in search of an effective, nontoxic natural compound, with potential anti-oxidant activity for prevention of chronic NCDs [12-15]. It seems that after the discovery of the biological significance of the molecular hydrogen produced in the intestines, there has been a dramatic shift to the belief that hydrogen may have a critical protective role in health and disease [14-17]. In the last 20 years, large number of studies have been published indicating that molecular hydrogen, either produced endogenously via consuming healthy foods or via any releasing agents, administered exogenously via inhalation or hydrogen rich water (HRW), acts as potential antioxidant in a wide range of physiological and pathophysiological processes [16,17]. Molecular hydrogen in itself appear to be a potential antioxidant that can also inhibit hydroxyl and nitrosyl radicals in the cells and tissues, causing a marked decline in oxidative stress, leading to a decline in the inflammation that is marker in the pathogenesis of NCDs. Slezak et al. and other experts [12-15] have demonstrated that hydrogen can also rapidly diffuse into tissues and cells without affecting metabolic redox reactions and signaling reactive species [12-15] Apart from its direct neutralizing effects on reactive oxidants, hydrogen, directly decreases free radical stress by regulation of expression of genes [16, 17]. It seems that molecular hydrogen not only regulate gene expression but also does epigenetic modulation, which could be alternative mechanisms for decline in oxidative stress-induced damage to genes, resulting in to increase in its anti-inflammatory and anti-apoptotic potential [16,17]. It is proposed that apart from improvement in gut microbiota, molecular hydrogen may also activate the production of bioactive lipids that are potential anti-inflammatory metabolites. This potential of molecular hydrogen may be utilized for preventive and therapeutic applications. (Figure 3).
The emergence of gut microbiome in the signaling of neuronal cells and neurogenesis poses the possibility that targeting the gut–brain axis could be a new strategy for treatment of neurodegenerative diseases and other NCDs [39]. Apart from SCFA, there may be increased production of bioactive lipids; protectins, maresins, resolvins, and nitrolipids that are also anti-inflammatory molecules. Several studies concerned with diseases of gastroentestinal, metabolic, cardiovascular and neurodegeneration support the existence of a bidirectional communication network of signaling mediators, such as bioactive lipids, that can interact with molecular hydrogen in modulation of inflammation, gut permeability, microbiota composition, and the gut–brain axis [39].The crosstalk between the gut–brain axis, microbiome, molecular hydrogen and bioactive lipids may emerge as the basis of a promising therapeutic strategy to counteract the pathogenesis of many of the NCDs. The results from recent studies, can contribute to the explanation of a new beneficial mechanism of hydrogen on a part of antioxidant protection in organism [44-46]. The hydrogen produced in the large intestine is metabolized, and excreted in the large intestine [44], by the microbes. [45]. The largest amount of hydrogen is produced by Blautia coccoides and Clostridium leptum. [45]. However, depending on microbiota composition, substantial amounts of hydrogen molecules are consumed by methanogenic and sulfate-reducing bacteria [45,46].
Molecular Hydrogen; A New Therapeutic Agent
Hydrogen is the most abundant element in the universe, which typically exists as molecular hydrogen in its diatomic form (H2). It has been considered as a biologically inert gas initially, although later on, in 1975, bio-therapeutic effects of hydrogen were observed, by Dole and co-workers, for the first time [47]. It is only recently, with the discovery of the antioxidant properties of hydrogen, its beneficial effects have been reported in the peer-reviewed journals, [48]. The new discoveries drew increasing attention on new therapeutic strategies such as drinking HRW, inhalation of hydrogen gas, injecting the saline rich in hydrogen, along with topical administration via hydrogen baths, and its buccal consumption. It has been reviewed that in all the NCDs, in which oxidative stress-related damage is the major problem, molecular hydrogen may be administered as an effective antioxidant for the prevention of these chronic diseases [37-41]. Hydrogen also alleviates blood-brain barrier impairment and improves cognitive dysfunction [23]. Hydrogen therapy has been found to ameliorate cardiac remodeling [24], dyslipidemia and metabolic syndrome [25] oxygen saturation in chronic lung disease [26] and in NSAID-induced enteropathy [27]. Hydrogen therapy as combine treatment showed beneficial effects in facial paralysis [28], on physical fatigue via prefrontal cortex activation during and after high intensity exercise [29]. The oxidation of LDL by myeloperoxidase produces ROS along with free radical generation which may be protected by antioxidants such as hydrogen [40-43].
Effects of Molecular Hydrogen on Obesity, Diabetes and Metabolic Syndrome.Molecular hydrogen therapy has been used among patients with metabolic diseases by the several experts [49-56]. Obesity is the first metabolic disease which begins with hypertrophy of adipocyte causing overweight and central obesity leading to metabolic syndrome and T2DM [51-53]. Metabolic syndrome may be defined as an accumulation of at least three risk factors out of obesity, diabetes, hypertension, hyperlipidemia and low HDL. It is possible that free radical stress with or without inflammation, with decrease in high density lipoprotein (HDL) cholesterol are crucial in the development of metabolic syndrome which is a risk factor of T2DM and CVDs [49,51-55]. Treatment with HRW may improve metabolism of glucose and lipids in T2DM patients or those with glucose intolerance because both conditions are associated with oxidative stress [49,50]. The effectiveness of HRW (1.5–2 L/day) was examined in an open label, 8-week study in 20 subjects with potential metabolic syndrome [51]. HRW was produced by placing a metallic magnesium stick into drinking water (hydrogen concentration; 0.55–0.65 mM) by the following chemical reaction: Mg + 2H2O → Mg (OH)2 + H2. The consumption of hydrogen-rich water for 8 weeks resulted in a 39% increase (p<0.05) in antioxidant enzyme superoxide dismutase (SOD) and a 43% decrease (p<0.05) in thiobarbituric acid reactive substances (TBARS) in urine [49]. Further, subjects showed an 8% increase in high-density lipoprotein (HDL)-cholesterol and a 13% decrease in total cholesterol/HDL-cholesterol from reference to week 4. There was no change in fasting glucose concentrations during the 8-week study. Drinking hydrogen-rich water may represent a potentially novel therapeutic and preventive strategy for metabolic syndrome.
In a randomized, controlled trial, Singh,s group administered HRW showing favorable effects on multiple parameters of metabolic syndrome after treatment for 24-week [25]. Compared to control group (P < 0.05), (P = 0.309), HRW group showed significant decline in the parameters of central obesity BMI and WHR after treatment with HRW (P < 0.05) [25]. In addition, treatment with HRW caused a significant decline in blood lipids as given in the table 1. Table 1.
Treatment with HRW also showed decline in fasting blood glucose after 24-week, in the active treatment group, along with a significant decline in HbA1C (12%, P < 0.05) compared to baseline levels and placebo group [25]. Treatment with HRW also reduced the markers of inflammation; TNF-α, and IL-6 (P<0.05). Interestingly, markers of oxidation showed significant decline, while vitamins C and E showed rise in the hydrogen group. Serum levels of angiotensin converting enzyme showed significant decline whereas serum nitrite level showed significant increase, which may cause decline in blood pressures. Table 2.
In a cross-over, randomized, controlled, trial in 30 patients with T2DM and 6 patients with impaired glucose tolerance, patients took either 900 mL/d of HRW or 900 mL of placebo water for 8 weeks, with a 12-week period of washout [50]. Intake of HRW was associated with a significant decline in the concentrations of modified LDL cholesterol, small dense LDL, and urinary 8-isoprostanes by 15.5% (P < 0.01), 5.7% (P < 0.05), and 6.6% (P < 0.05), respectively. Intake of HRW was also associated with a trend of decreased serum concentrations of oxidized LDL and free fatty acids, and increased plasma concentrations of adiponectin and extracellular-superoxide dismutase [50]. These results suggest that supplementation with HRW may have a beneficial role in the prevention of T2DM and insulin resistance, without any adverse effects [51]. This observational, non-interventional, retrospective, double-arm, 6-month clinical study included T2DM patients (n=1088), receiving anti-diabetes drugs with or without hydrogen initiation from 2018 to 2021[52]. Interestingly, subjects in hydrogen group maintained greater improvement in the level of HbA1c (-0.94% vs -0.46%), fasting blood glucose (-22.7 mg/dL vs -11.7 mg/dL), total cholesterol (-12.9 mg/dL vs -4.4 mg/dL), HOMA-IR (-0.76 vs -0.17) and HOMA-β (8.2% vs 1.98%) with all p< 0.001 post the treatment, compared to control group. Logistics regression analysis revealed that the likelihood of reaching HbA1c< 7%, ≥ 7% to< 8% and > 1% reduction at the follow-up period was higher in the hydrogen group, while patients in the control group were more likely to attain HbA1c ≥ 9%. Patients in hydrogen group had a lower incidence of several adverse effects including hypoglycemia (2.0% vs 6.8%), vomiting (2.6% vs 7.4%), constipation (1.7% vs 4.4%) and giddiness (3.3% vs 6.3%) with significance in comparison to the control group [52]. It is clear that hydrogen therapy as an adjunct, may benefit glycemic control, lipid metabolism, insulin resistance and incidence of adverse events in T2DM patients after 6-month treatment.
Hydrogen may activate ATP-binding cassette transporter A1-dependent efflux, enhance HDL anti-atherosclerotic functions, and have beneficial lipid-lowering effects. In a more recent randomized trial among 30 subjects with nonalcoholic fatty liver disease (NAFLD), treatment with HRW was administered for eight weeks [57]. Despite short period of therapy, beneficial trends (p > 0.05) were observed in decreased weight (≈1 kg) and body mass index as well as a trend of improved lipid profile and reduced lactate dehydrogenase levels, in the HRW group. HRW tended to non-significantly decrease levels of nuclear factor kappa B, heat shock protein 70 and matrix metalloproteinase-9. In a recent controlled trial, including 43 subjects, inhalation of hydrogen/oxygen improved serum lipid and liver enzymes [56]. There was a significantly improvement in liver fat content detected by ultrasound and CT scans after hydrogen/oxygen inhalation depending upon severity. In the same study, including diet-induced mice model, the effect of hydrogen on mouse NASH showed that hydrogen/oxygen inhalation improved systemic inflammation and liver histology. Molecular hydrogen also inhibited lipid accumulation in AML-12 cells indicating that hydrogen/oxygen inhalation can inhibit NAFLD which may be due to hepatic autophagy [56]. Since metabolic syndrome has become a worldwide problem, hydrogen therapy may be a new approach for the prevention of metabolic disease [51-57].
Hydrogen therapy may positively affect mitochondrial bioenergetics. In an experimental study in rats, Gvozdjakova et al. reported, increased state 3 respiration with both CI and CII-linked substrates in cardiac mitochondria after H2 administration [70]. It is proposed that H2 may convert the quinone intermediates in the Q-cycle to the fully reduced ubiquinol, increasing this way antioxidant capacity of the quinone pool and preventing mitochondrial ROS generation [71].
The increase in the rate of ATP production was accompanied with increased concentration of CoQ9 in heart tissue and mitochondria and decreased plasma levels of malondialdehyde [71]. Beneficial effects of molecular hydrogen in various experimental models of human diseases and in many clinical studies was documented. H2 can be administered by various ways, as a gas inhalation, drinking of hydrogen-enriched water, or taking a hydrogen-dissolved bath as well as in saline infusions [70-72]. As antioxidant, hydrogen selectively scavenges hydroxyl and peroxynitrite radicals, and decreases oxidative stress, however, the hydrogen effect on antioxidant–coenzyme Q information is lacking. A recent review has reemphasized, that Indo-Mediterranean type of foods or DASH diet that are known to decrease blood pressure, may also produce greater amount of hydrogen in the gut, which may be responsible for prevention of hypertension [58].
Effects of Hydrogen Therapy on Blood Lipids
High LDL cholesterol is known to predispose atherosclerosis which is recognized as a chronic inflammatory condition that begins with the dysfunction or activation of arterial endothelium. Low-density lipoprotein (LDL) and especially its oxidized form play a key role in endothelial dysfunction and atherogenesis. Several small-scale studies evaluating the effects of HRW, indicated an advantageous effects in regulating blood lipid profiles. In a recent meta-analysis, including seven studies, the finding reported a significant decline in total cholesterol, LDL, and triglycerides after HRW intake (p = 0.01), with small to moderate effects [42]. The results indicate that drinking HRW can cause significant benefit in the lipid profile of the patients. The Forest Plot of studies shows total cholesterol with a small negative effect (pooled SMD = −0.23 [from −0.40 to 0.05]; p ≤ 0.01), (b) LDL with small effect (pooled SMD = −0.22 [from −0.39 to 0.04]; p ≤ 0.01), and (c) triglycerides, with a moderate beneficial effect (pooled SMD = −0.38 [from −0.59 to 0.18], p ≤ 0.01).( Figure 4).
Increase in triglycerides with decline in HDL cholesterol are important characteristics of metabolic syndrome, which are common in most of the clinical trials, using HRW among patients with metabolic syndrome [25,52-57]. Treatment with HRW was associated with beneficial effects on blood glucose and blood lipids with significant decline in blood lipoproteins [25, 52-56] and a beneficial trend in some of the trials [57].
Effects of Hydrogen Therapy on Blood Pressures
Previous studies showed that hydrogen supplementation m a decrease blood pressures (59, 60). Nakayama et al. developed a hydrogen enriched dialysate by reverse osmosis via the electrolysis of purified tap water. He and found that compared to hemodialysis with standard dialysate, dialysis with hydrogen-enriched dialysate reduces blood pressure, in particular systolic blood pressure, in patients on chronic maintenance hemodialysis [60]. In an experimental study, 5/6 nephrectomized rats given inhalation of either hydrogen (1.3% H2 + 21% O2 + 77.7% N2) or control (21% O2 + 79% N2) gas mixture for 1 h per day [59]. Addition of hydrogen significantly suppressed the rise in blood pressure after 5/6 nephrectomy. Interestingly, blood pressure lowering effect of hydrogen was also confirmed in rats in a stable hypertensive state 3 weeks after nephrectomy. Implantation of telemetry system for continuous blood pressure monitoring revealed, that an anti-hypertensive effect was observed during daytime rest, as well as during night-time activities. It seems that hydrogen therapy caused improvement in blood pressure variability and autonomic imbalance, by suppressing the overly active sympathetic nervous system and augmenting parasympathetic nervous system activity [59]. It is possible that 1-h daily exposure to hydrogen supplementation exerts an anti-hypertensive effect in an animal model of hypertension. This experiment provide further support that decline in blood pressure variability via DASH diet, may be because increased production of hydrogen in the gut, due to high content of fiber, flavonoids and omega-3 fatty acids in the diet [58]. In a randomized, controlled trial [25], supplementation with HRW was associated with significant decline in systolic and diastolic blood pressures, as well as heart rate (Personal communication, by Singh et al). This study also found that hydrogen therapy was associated with significant decline in angiotensin converting enzyme(ACE) and nitrite, a precursor of nitric oxide (NO) [25]. Decline in ACE and increase in NO can cause decrease in blood pressures. Larger randomized, controlled trials would be necessary to confirm the blood pressure controlling role of hydrogen therapy in hypertension.
In a controlled trial, of 60 patients randomized to treatment, 56 patients completed the study (27 in the Air group and 29 in the H2-O2 group). The right and left arm systolic blood pressure (SBP) were significantly declined in H2-O2 group compared with the baseline levels (151.9 ± 12.7 mmHg to 147.1 ± 12.0 mmHg, and 150.7 ± 13.3 mmHg to 145.7 ± 13.0 mmHg, respectively; all p < 0.05). Interestingly, treatment with hydrogen, significantly reduced diastolic nighttime ambulatory blood pressure by 2.7 ± 6.5 mmHg (p < 0.05). In the placebo group, all blood pressures showed no affect (all p > 0.05). In addition, the angiotensin II, aldosterone, and cortisol levels as well as the aldosterone-to-renin ratio in plasma were significantly lower in H2-O2 group compared with baseline (p < 0.05). No significant differences were observed in the Air group before and after the intervention. It is clear, that inhalation of a low-dose H2-O2 mixture exerts a favorable effect on blood pressure, and reduces the plasma levels of hormones associated with hypertension on renin-angiotensin-aldosterone system and stress in midlife/older adults with hypertension.
Effects of Hydrogen Therapy on Endothelial Function
NO is a signaling molecule involved in many physiological and pathological processes and a vasodilator in the vascular system. The endothelium is the major source of NO, under healthy conditions, Release of NO from the endothelium may be examined by finding out the flow-mediated dilation (FMD) that occur due to hyperemia caused by atherosclerotic occlusion of brachial artery [13]. It seems that the effects of cardiovascular risk factors; tobacco, aging, obesity, hyperlipidemia, diabetes and hypertension, as well as hyperglycemia after meals on endothelial dysfunction may be examined by this method. These risk factors may increase the oxidative stress resulting into endothelial dysfunction due to redox imbalance. The role of ROS is crucial in the development of vascular disease, but physiological generation of ROS is necessary for vasomotor function in most of the vessels [13]. Thus the imbalance in the redox state between NO and superoxide radical produced in the endothelial cells may be crucial in causing endothelial dysfunction. For example, another ROS; H2O2 may cause either detrimental or beneficial influence on vascular function, depending on presence endogenous antioxidants in the arterial cells. The role of hydroxyl radical, produced as byproduct of decay of hydrogen peroxide is unclear, although it is known that it causes impairment in the endothelium, which can be neutralized by molecular hydrogen [13]. In a clinical study, administration of hydrogen was associated with significant rise in FMD, from (mean ± SD) 6.80%±1.96% to 7.64%±1.68%, whereas in the control group, there was a decline from 8.07%±2.41% to 6.87%±2.94% [13]. There was a significant beneficial effect in the ratio of FMD in the high-H2 group than to the control group [13]. It is possible that treatment with hydrogen may protect the vasculature from shear stress-derived detrimental hydroxyl radical by maintaining the nitric oxide-mediated vasomotor response.
Effects of Molecular Hydrogen in Stroke
In experimental studies, molecular hydrogen therapy was found to act as an antioxidant, and inhalation of hydrogen gas (1-4%) was markedly effective for the improvement of cerebral infarction [62-65]. Inhalation hydrogen during normoxic resuscitation was also found to improve neurological outcomes in a cardiac arrest. In a controlled trial, 50 patients were randomized to (25 each in the hydrogen group and the control group) a therapeutic time window of 6 to 24 hours [65]. The hydrogen group inhaled 3% hydrogen gas (1 hour twice a day), and the control group received conventional intravenous medications for the initial 7 days. Treatment with hydrogen was associated with no significant adverse effects but with improvements in oxygen saturation. The relative signal intensity of MRI of brain was significant, indicating the severity of the infarction site, National Institute of Health(NIH) Stroke Scale scores for clinically quantifying stroke severity, and physical therapy evaluation, as judged by the Barthel Index were also significant in the hydrogen group[65].It is clear that hydrogen treatment was safe and beneficial in patients with cerebral infarction. In another controlled trial, the safety and effectiveness of H2 hydrogen therapy was examined in patients with cerebral infarction in an acute stage with mild- to moderate-severity (NIH) stroke scale scores (NIHSS = 2-6) [66]. No significant adverse effects were noted in the hydrogen group, with improvements in oxygen saturation. The following significant effects were found: the relative signal intensity of MRI, which indicated the severity of the infarction site, NIHSS scores for clinically quantifying stroke severity, and physical therapy evaluation, as judged by the Barthel Index were significant changes in the hydrogen group compared to control group. It is possible that hydrogen acts by reducing cerebral artery vasospasm and direct beneficial effects on neurons, by improving mitochondrial function and over all vascular function, due to its anti-inflammatory, and improved signal transduction and gene function effects [67-70].
In a case study among 200 patients, those treated with H2 gas had significantly greater improvement in NIH stroke scale score than patients treated with standard therapy [67]. The neurological improvement was significantly greater in patients treated with hydrogen gas than those that received standard therapy for all the days tested (p < 0.05). The onset of NIH stroke scale score reduction was faster in patients treated with hydrogen gas when compared to standard therapy. Hydrogen therapy also showed significant improvement in MRI signal Intensity score, which indicates that hydrogen was effective in recovery of infraction site[67]. The findings of this study show that hydrogen gas administered via the inhalation route is effective and safe in Chinese patients with acute cerebral infarction, and is therefore, superior to standard therapy.
Effects of Molecular Hydrogen on Ischemia and Reperfusion Injury
There is evidence that oxidative and pro-inflammatory stress are underlying causative factors in myocardial ischemia/reperfusion (I/R) injury, in which hydrogen therapy may be useful [37,38,71]. It seems that increased amounts of ATP are required by the cardiac myocytes, for their physiological function, which needs high density of mitochondria are to allow their high energy needs. These mitochondria, filled with reactive intermediates and pro-apoptotic signals, are intimately involved in I/R injury [63]. The inner mitochondrial membrane is responsible for maintaining mitochondrial transmembrane potential, and is usually impermeable to ions and proteins [69]. However, under stress, the opening of the mitochondrial permeability transition pore (mPTP) creates a non-selective channel between the inner membrane of the mitochondrion and the sarcoplasm. This results in to a loss of the electrochemical gradient, production of ROS, Ca2+ overload, and formation of apoptosomes responsible for apoptosis [72]. It is well known that that there is free radical generation through partial reduction of oxygen during I/R injury, that can rapidly overwhelm the cell’s endogenous antioxidant self-defense system [71-74]. These reactions may cause cellular injury by damaging lipids, proteins, DNA, and RNA. The xanthine oxidase substrates, xanthine and hypoxanthine, accumulate during [73]. ischemia, which triggers xanthine oxidase activation and consequently increased production of ROS. These ROS can also elicit the opening of the mPTP resulting in a positive feedback loop of increased ROS production from the mitochondria [72,74].
It seems that restoration of blood flow in an acutely obstructed coronary artery, represents the most effective, long-term clinical therapy for AMI, which is also responsible for I/R injury in the myocardial cells. The myocardial remodeling and fibrosis, as component of healing are the most important targets of hydrogen therapy that can influence the outcomes in patients with myocardial infarction [24]. In presence of metabolic diseases and CVDs, the amount of fibrosis and apoptosis are crucial for the development of heart failure. The novel therapeutic approaches for the management of cardiac remodeling and fibrosis of myocardium are important for increased survival of patients with CVDs. In a rat model of myocardial infarction, the treatment included inhalation of 2 % hydrogen daily for 3 hours, for a duration of 28 days [24]. The results revealed that treatment with hydrogen may be associated with improved function of the heart with decrease in the area of fibrosis. It seems that treatment with hydrogen provides special beneficial effect, in the I/R injury of the cardiomyocyte, via reducing pyroptosis mediated by NLRP3, that occur after restoration of blood flow in the coronary artery [24]. Table 3.
Many cellular and molecular processes contribute to ventricular remodeling in response to myocardial irradiation, myocardial I/R injury, myocardial infarction, hypertension, neuro-humoral activation or other pathophysiological stimuli [75]. Increased production of endothelin-1 (ET-1), angiotensin II, catecholamines and pro-inflammatory cytokines, bind to their cognate receptors and activate the downstream signaling events, results in the remodeling. These pathophysiological alterations may cause either necrosis, apoptosis, autophagy, or hypertrophy of the cardiomyocytes. There may be activation of fibroblast to produce collagen and other proteins that cause fibrosis [75,76]. Although restoration of blood flow in the coronary artery, is critical, the perfusion of oxygen-rich blood induces cytotoxic ROS production. This eruption of ROS leads to cellular necrosis and apoptosis, a process may be called lethal reperfusion injury [77]. Such injury accounts for up to 50% of the final size of the infarct [78]. In addition, the cascade of events occurring within cardiomyocytes, the endothelium is also actively involved in the I/R injury.
NO elicits vasodilation, which provides protective effects during I/R, in part by influencing oxygen consumption, platelet aggregation, leukocyte adhesion, and free radical metabolism [79]. High concentrations of NO exacerbate I/R injury largely by producing highly reactive peroxynitrite In addition to NO, the coronary endothelium has several other pathophysiological roles in I/R, such as serving as a source of non-NO vasoactive substances, activating the immune system, and an increased expression of cytokines, chemokines, and various adhesion molecules [72]. It is possible that increased availability of hydrogen due to inhalation of HRW, may blunt the adverse effects of NO, resulting in to overall beneficial effects.In an experimental study, treatment with hydrogen improved the size of myocardial infarction, cardiac function, apoptosis and cytokine release following myocardial ischemia(MI)/Reperfusion ® in rats [80]. Hydrogen also improved cell viability and LDH release following hypoxia/reoxygenation in myocardial cells in- vitro. Apart from these effects, hydrogen exerted an anti-inflammatory and anti-apoptotic effect in myocardial cells induced by H/R via PINK1/Parkin mediated autophagy. It is clear that hydrogen-rich saline alleviated the inflammation response and apoptosis induced by MI/R or H/R in vivo or in vitro, and that hydrogen-rich saline contributed to the increased expression of proteins associated with autophagy. The present study indicated that treatment with hydrogen-rich saline improved the inflammatory response and apoptosis in MI/R. In a clinical study among 20 patients with ST segment elevation myocardial infarction, hydrogen inhalation during angioplasty was associated with good feasibility and safety, which may have also promoted left ventricular reverse remodeling at 6 months after infarction [81].
Effects of Hydrogen Therapy in Neurodegenerative Diseases
As a recognized reducing gas, hydrogen has shown great anti-oxidative stress and anti-inflammatory effect in many cerebral disease models [82-86]. It can ameliorate neuronal damage, maintain the number of neurons, prolong the lifespan of neurons, and ultimately inhibit disease progression. Hydrogen exhibits the potential to treat Alzheimer's disease [82]. Stereotactic injection has been previously used as an invasive method of administering active hydrogen, but this method has limitations in clinical practice. In this study, triple transgenic (3×Tg) Alzheimer's disease mice were treated with HRW for 7 months. The results showed that treatment with HRW prevented synaptic loss and neuronal death, inhibited senile plaques, and reduced hyperphosphorylated tau and neurofibrillary tangles in 3×Tg Alzheimer's disease mice. In addition, hydrogen-rich water improved Interestingly, disorders of brain energy metabolism disorders, intestinal flora imbalances and reduction in inflammatory reactions were also observed on treatment with HRW. The results indicated that HRW therapy is an effective hydrogen donor that can treat Alzheimer's disease [82,83], anxiety like behavior [84]. Parkinson,s disease [85] and ageing [86].
Effects of Molecular Hydrogen on Bone and Joint Diseases
There is evidence that compared to common antioxidants vitamin C and vitamin E, molecular hydrogen has two unique characteristics; hydrogen selectively reduces cytotoxic ROS such as the hydroxyl radical and does not react with other ROS that possesses physiological roles. Secondly, since molecular hydrogen is small and electrically neutral, it easily penetrates membranes and enters cells and organelles including nucleus and mitochondria, where normal antioxidant cannot reach [22]. In an experimental study in ovariectomized rats, treatment with HRW was associated with reduction of bone mass including bone mineral content and bone mineral density in femur and vertebrae, and preserved mechanical strength including ultimate load, stiffness, and energy, and bone structure. Interestingly, trabecular bone volume fraction, trabecular number, and trabecular thickness in femur as well as mechanical strength including ultimate load and stiffness, and bone structure including trabecular bone volume fraction and trabecular number in vertebrae also showed benefit on hydrogen administration. In addition, treatment with HW abated oxidative stress and suppressed IL-6 and TNF-α mRNA expressions in femur of ovariectomized rats; treatment with HW increased femur endothelial NOS activity and enhanced circulating NO level in ovariectomized rats, indicating that intake of hydrogen can prevent osteopenia by decreasing oxidative stress and inflammation. The results of this study were also confirmed in another study among rats having bone loss induced by microgravity in which, treatment with hydrogen molecule abated oxidative stress and alleviated bone loss [88].
Effects of Hydrogen on Cancer
Hydrogen therapy has been found to have positive effects in terms of quality of life in patients with cancer [89-95]. It was examined and suggested to use hydrogen therapy in cancer in 1975 [92]. Treatment with hydrogen may improve liver function in patients who were administered chemotherapy, as well as reduce side effects for those receiving radiation therapy, and has protective effects against radiation-induced bone marrow damage in cancer patients [89-91].
Hydrogen has an anti-proliferative, anti-oxidative, pro-apoptotic and anti-tumor effects in carcinogenesis [90]. In a meta-analysis, out of the 677 studies, 27 fulfilled the eligibility criteria, where data was compiled into a table, outlining the general characteristics and findings. Analysis of data found that hydrogen plays a promising therapeutic role as an independent therapy as well as an adjuvant in combination therapy, resulting in an overall improvement in survival, quality of life, blood parameters, and tumor reduction [90].
Previous studies showed that hydrogen display anti-cancer properties when administered on its own. In mice with squamous cell carcinoma, hyperbaric hydrogen therapy has been examined as a potential cancer therapy, revealing potent anti-tumor effects [92]. In another experimental study, study in mice with colon cancer, treatment with HRW was found to cause benefit dose-dependently potentiating the tumor-inhibitory activity of 5-furourasil (5-FU) by enhancing cellular apoptosis of the cancer cells [93]. In a recent experimental study including 24 mice bearing tumors were randomly divided into four groups (n = 6 per group) [94]. Combined treatment with HRW and 5-FU or HRW alone, significantly improved tumor size and weight, collagen content and fibrosis as compared to the colorectal cancer control group. Interestingly, HRW alone also attenuated oxidative stress and potentiated antioxidant activity, whereas treatment with 5-FU exacerbated oxidative stress and blunted antioxidant effects due to tissue damage. These findings from experimental study indicate that treatment with HRW, with or without 5-FU, may serve as a therapeutic agent for treating colorectal cancer. Hydrogen enhances proliferation of four out of seven human cancer cell lines indicating response to therapy [95]. The effects showing proliferation-promotion may not correlate with basal levels of cellular ROS. The expression profile of the seven cells showed that the responders have higher gene expression of mitochondrial electron transport chain (ETC) molecules than the non-responders.
Effects of Hydrogen Therapy in Kidney Diseases
Common types of kidney disease include acute kidney injury (AKI), drug toxicity, renal fibrosis, polycystic kidney disease, ischemia reperfusion injury and renal cell carcinoma [96-103]. In most of the kidney diseases also, oxidative stress, inflammatory mediators and inflammatory effector cells and the imbalance between pro-inflammatory cytokines and anti-inflammatory cytokines play an important role in the occurrence and progression of kidney diseases [96]. It seems that the role of hydrogen in regulating and maintaining homeostasis in inflammatory kidney disease and the treatment of inflammatory kidney diseases from the perspective of pro-inflammatory cytokines and anti-inflammatory cytokines may be an interesting route for further research [96-104]. Nephropathy is a serious complication of obesity and diabetes mellitus. Metabolic disorders can occur and manifest as local inflammation of the kidney that can lead to fibrosis and structural remodeling of the organ [104]. Therefore, tackling the immune-mediated inflammation is very significant for the treatment of metabolic nephropathy [105]. There is an activation of immune cells, in AKIs, such as renal artery infarction or toxin-mediated kidney injury [99-101].
It seems that renal epithelial cells damage, activate the stress response pathways, leading to the secretion of cytokines and vasoactive factors, resulting in immune-pathological damage [105]. Hydrogen, on the other hand, can suppress the production of immune-reactive substances [96]. Treatment with HRW has been found to inhibit cyclosporine A-induced nephrotoxicity via the Keap1/Nrf2 signaling pathway [97], kidney fibrosis due to AKI by retaining Klotho expression [99], after ischemia/reperfusion injury in rats via anti-oxidative stress, anti-apoptosis and anti-inflammation [100]. Hydrogen also acts by increased expression of heme-oxygenase-1 in aged rats [101, 102], in mice with calcium oxalate-induced renal injury [103] and immune cell damage in diabetic nephropathy [104] as well as in patients on peritoneal dialysis with peritoneal damage in chronic kidney disease [105]. It seems that the endoplasmic reticulum (ER) stress is characterized with pathological stress inducing an accumulation of unfolded proteins in the ER [96]. It has been observed that the inhalation of hydrogen significantly decreased the ER stress-related protein levels with decline in the tissue damage in myocardial IRI [105]. Similar mechanisms may be involved showing that hydrogen is able to ameliorate chronic intermittent hypoxia (CIH)-induced kidney injury by decreasing ER stress and activating autophagy.
Effects of Hydrogen in Chronic Lung Diseases
Chronic lung diseases affect the airways; alveoli, bronchioles and bronchi as well as other structures of the lungs. Some of the most common lung diseases are; chronic obstructive pulmonary diseases (COPD), bronchial asthma, occupational lung diseases, tuberculosis, cancer, and pulmonary hypertension [1]. All the chronic lung diseases such as bronchial asthma and COPD, as well as post COVID-19 pulmonary fibrosis, may be associated with lung damage along with fibrosis and emphysema [106]. Major pathogenic factors that contribute to developing lung disease include infection and inflammation, protease and antiprotease imbalance, and oxidative stress, which overwhelms the antioxidant defenses. Moreover, ROS play a pivotal role in the incidence of acute exacerbations of diseases [106]. The major feature of COPD and other united airway diseases is characterized with an abnormal response to infection or allergen–induced injury, causing oxidative stress and chronic inflammation, and subsequent activation of macrophages, eosinophils, neutrophils, T lymphocytes, and fibroblasts in the lung [106].
Recently, molecular hydrogen has been suggested for the treatment of COVID-19 [107-108], as well as COPD [109,110] due to its potential antioxidant and anti-inflammatory effects. In a randomized, double-blinded, placebo-controlled trial involving 10 centers, patients (n=54 in each group) with acute exacerbation of COPD (AECOPD) and a Breathlessness, Cough, and Sputum Scale (BCSS) score of at least 6 points were randomly assigned to receive a hydrogen/oxygen therapy or oxygen only [110]. Improvements in the BCSS score in the hydrogen/oxygen group was significantly greater compared to the oxygen only group (− 5.3 vs. − 2.4 point; difference: − 2.75 [95% CI − 3.27 to − 2.22], indicating superiority. Other time points from day 2 through day 6, had similar findings. Cough Assessment Test score also showed significant decline in the hydrogen/oxygen group compared to control (− 11.00 vs. − 6.00, p < 0.001). Changes in pulmonary function, arterial blood gas and noninvasive oxygen saturation did not differ significantly between groups as well as other endpoints. However, similar to our findings, analysis of the per-protocol set did find significant group interactions with respect to the changes from baseline in SpO2 (P<0.0001). Acute exacerbations were reported in 34 (63.0%) patients in hydrogen/oxygen group and 42 (77.8%) in oxygen group. This trial demonstrated that hydrogen/oxygen therapy is superior to oxygen therapy in patients with acute exacerbation of COPD with acceptable safety and tolerability profile [110]. Inhalation of hydrogen has been found to protect against acute lung injury induced by hemorrhagic shock and resuscitation[111], as well as in adjuvant therapy in COVID-19 [112,113] and chronic heart failure [114].In a clinical observation among 10 patients with chronic lung diseases, HRW administration was associated with a significant increase in oxygen saturation (SpO2) and decrease in TBARS, MDA, and diene conjugates, with an increase in vitamin E and nitrite levels, compared to baseline levels [115]. Physical training done after HRW therapy appeared to increase exercise tolerance and decrease hypoxia, as well as delay the need for oxygen therapy. Treatment with HRW in patients with hypoxia from chronic lung diseases may decrease oxidative stress and improve oxygen saturation in some patients. Mechanisms of benefit via hydrogen therapy are given in Figure 5.
Apart from above diseases, molecular hydrogen may be protective against peripheral arterial disease [117.118], gene expression [119,120], acute cerebral ischemia [121], sleep deprivation [122], traumatic brain injury [123], aneurismal sub-arachnoid hemorrhage [124], radiation induced bone-marrow damage [125], non-small-cell lung cancer [126], restore exhausted CD8+ T cells in lung cancer [127], cognitive function in women [128],alcohol induced hangover [129], idiopathic sudden sensorineural hearing loss[130], post-cardiac arrest syndrome [131], gut microbiota [132],cardiopulmonary bypass surgery [133], stimulation of cardiac autonomic activity [134] and dry eye syndrome [135]. vascular aging of the aorta [137], radiation therapy for cancer [138].
Conclusions
All the risk factors of NCDs, in particular diet, act by damaging the concerned organ which is mainly involved in producing a disease by causing oxidative stress and inflammations in the cells and tissues. In obesity, adipocytes are the main target but systemic inflammation also occur in the beta cells of pancreas, endothelial cells, smooth muscle cells and hepatocytes resulting in to metabolic syndrome and T2DM. Inflammation in the cardiomyocytes, may predispose cardiac hypertrophy resulting in to heart failure, whereas inflammation in the vasculature, including endothelium and smooth muscle cells, may predispose atherosclerosis and hypertension respectively. Similarly, cellular damage in neurons, osteocytes and osteoblast, bronchial tree, glomerular cells in kidney, may be responsible for development of related diseases. Since oxidative stress enhances systemic inflammation, it may damage the function of cardiomyocyte, beta cells, kidney cells and bone marrow, as well as neurons, apart from endothelium, predisposing development of concerned diseases. Treatment with hydrogen may inhibit the free radical generation with decline in inflammation, resulting in to restoration of cell function, causing improvement in the related organ and concerned NCDs.
Acknowledgments
We thank International College of Nutrition for providing logistic support to write this article.
Conflicts of Interest
AT is involved in the commercial industry pertaining to molecular hydrogen for health, RBS has accepted travel grant to present this work in a conference. All other authors declare no conflict of interest.
References
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021. [CrossRef]
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. [CrossRef]
- 3. Vaduganathan M, Mensah GA, Varieur Turco J, et al. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. Journal of the American College of Cardiology. 12 December. [CrossRef]
- Jiang S, Liu H, Li C. Dietary regulation of oxidative stress in chronic metabolic diseases. Foods. 2021 Aug 11;10(8):1854. [CrossRef]
- Aleksandrova, K.; Koelman, L. Rodrigues CE. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biology 2021, 42, 101869. [Google Scholar] [CrossRef] [PubMed]
- Micha R, Penalyo JL, Cidhea F, Imamura F, Rehm CD, Mozaffarian D. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA 2017; 317 (9): 912-924. [CrossRef]
- Sacco RL, Roth GA, Reddy KS, Arnett DK, Bonita R, Gaziano TA, Heidenreich PA, Huffman MD, Mayosi BM, Mendis S, Murray CJL, Perel P, Piñeiro DJ, Smith SC Jr, Taubert KA, Wood DA, Zhao D, Zoghbi WA. The heart of 25 by 25: achieving the goal of reducing global and regional premature deaths from cardiovascular diseases and stroke: a modeling study from the American Heart Association and World Heart Federation. Circulation 2016; 133: e674-e690. [CrossRef]
- Singh, R.B.; Fedacko, J.; Fatima, G.; Magomedova, A.; Watanabe, S.; Elkilany, G. Why and How the Indo-Mediterranean Diet May Be Superior to Other Diets: The Role of Antioxidants in the Diet. Nutrients 2022; 14, 898. [CrossRef]
- Singh, R.B.; Fedacko, J.; Pella, D.; Fatima, G.; Elkilany, G.; Moshiri, M.; Hristova, K.; Jakabcin, P.; Vanova, N. High Exogenous Antioxidant, Restorative Treatment (Heart) for Prevention of the Six Stages of Heart Failure: The Heart Diet. Antioxidants 2022, 11, 1464. [Google Scholar] [CrossRef]
- Mojto, V.; Singh, R.B.; Gvozdjakova, A.; Pella, D.; Fedacko, J.; Pella, D. Molecular hydrogen: a new approach for the management of cardiovascular diseases. World Heart J 2018, 10, 83–93. [Google Scholar]
- Ichikawa Y, Yamamoto H, Hirano Si, Sato B, Takefuji Y, Satoh F. The overlooked benefits of hydrogen-producing bacteria. Med Gas Res 2022;12. Available online: https://www.medgasres.com/preprintarticle.asp?id=344977 (accessed on 20 December 2022).
- Slezák, J.; Kura, B.; Frimmel, K.; Zálešák, M.; Ravingerová, T.; Viczenczová, C.; Okruhlicová, Ľ.; Tribulová, N. Preventive and therapeutic application of molecular hydrogen in situations with excessive production of free radicals. Physiol. Res. 2016, 65 (Suppl. 1), S11–S28. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Sato, B.; Hara, K.; Hara, Y.; Naritomi, Y.; Koyanagi, S.; Hara, H.; Nagao, T.; Ishibashi, T. Consumption of water containing over 3.5 mg of dissolved hydrogen could improve vascular endothelial function. Vascular Health and Risk Management 2014, 10, 591–597. [Google Scholar]
- Ichihara, M.; Sobue, S.; Ito, M.; Ito, M.; Hirayama, M.; Ohno, K. Beneficial biological effects and the underlying mechanisms of molecular hydrogen- Comprehensive review of 321 original articles. Med. Gas Res. 2015, 5, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Lobo V, Patil A, Phatak A, Chandra N. Free radicals, antioxidants and functional foods: Impact on human health. Pharmacognosy Reviews 2010; 4 (8): 118-126. [CrossRef]
- Takac, I.; Schroder, K.; Brandes, R.P. The Nox family of NADPH oxidases: friend or foe of the vascular system. Curr Hypertens Rep 2012, 14, 70–78. [Google Scholar] [CrossRef]
- Montezano, A.C.; Touyz, R.M. Reactive oxygen species and endothelial function role of nitric oxide synthase uncoupling and Nox family nicotinamide adenine dinucleotide phosphate oxidases. Basic Clin Pharmacol Toxicol 2012, 110, 87–94. [Google Scholar] [CrossRef]
- Al Ghouleh, I.; Khoo, N.K.; Knaus, U.G. Oxidases and peroxidases in cardiovascular and lung disease: new concepts in reactive oxygen species signaling. Free Radic Biol Med 2011, 51, 1271–1288. [Google Scholar] [CrossRef]
- Bedard, K.; Krause, K.H. The NOX family of ROS-generating NADPH oxidases: physiology and pathophysiology. Physiol Rev 2007, 87, 245–313. [Google Scholar] [CrossRef]
- Deryugina AV, Danilova DA, Brichkin YD, Taranov EV, Nazarov EI, Pichugin VV, Medvedev AP, Riazanov MV, Fedorov SA, Andrej YS, Makarov EV. Molecular hydrogen exposure improves functional state of red blood cells in the early postoperative period: a randomized clinical study.Med Gas Res. 2023 Apr-Jun;13(2):59-66. [CrossRef]
- Yang M, Dong Y, He Q, et al. Hydrogen: a novel option in human disease treatment. Oxid Med Cell Longev. 2020;2020:8384742. /: https. [CrossRef]
- Ohsawa I, Ishikawa M, Takahashi K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13(6):688-694. [CrossRef]
- Yu Y, Feng J, Lian N, et al. Hydrogen gas alleviates blood-brain barrier impairment and cognitive dysfunction of septic mice in an Nrf2-dependent pathway. Int Immunopharmacol. 2020, 85, 106585. [Google Scholar] [CrossRef] [PubMed]
- Nie C, Zou R, Pan S, A R, Gao Y, Yang H, Bai J, Xi S, Wang X, Hong X, Yang W. Hydrogen gas inhalation ameliorates cardiac remodelling and fibrosis by regulating NLRP3 inflammasome in myocardial infarction rats. J Cell Mol Med. 2021 Sep;25(18):8997-9010. [CrossRef]
- LeBaron, T.; Singh, R.B.; Fatima, G.; Kartikey, K.; Sharma, J.P.; Ostojic, S.M.; Gvozdjakova, A.; Kura, B.; Noda, M.; Mojto, V.; Niaz, M.A.; Slezak, J. The Effects of 24-Week, High-Concentration Hydrogen-Rich Water on Body Composition, Blood Lipid Profiles and Inflammation Biomarkers in Men and Women with Metabolic Syndrome: A Randomized Controlled Trial. 2020, 13, 889–896. [CrossRef]
- Singh RB, Halabi G, Fatima G, Rai RH, Tarnava AT, LeBaron TW. Molecular hydrogen as an adjuvant therapy may be associated with increased oxygen saturation and improved exercise tolerance in a COVID-19 patient. Clin Case Reports 9: e05039. | 1 of 6. [CrossRef]
- Akita Y, Higashiyama M, Kurihara C, Ito S, Nishii S, Mizoguchi A, Inaba K, Tanemoto R, Sugihara N, Hanawa Y, Wada A, Horiuchi K, Okada Y, Narimatsu K, Komoto S, Tomita K, Takei F, Satoh Y, Saruta M, Hokari R. Ameliorating Role of Hydrogen-Rich Water Against NSAID-Induced Enteropathy via Reduction of ROS and Production of Short-Chain Fatty Acids.Dig Dis Sci. 2022 Dec 7:1-11. [CrossRef]
- Koyama Y, Harada S, Sato T, Kobayashi Y, Yanagawa H, Iwahashi T, Tanaka H, Ohata K, Imai T, Ohta Y, Kamakura T, Kobayashi H, Inohara H, Shimada S. Therapeutic strategy for facial paralysis based on the combined application of Si-based agent and methylcobalamin. Biochem Biophys Rep. 2022 Nov 21;32:101388. [CrossRef]
- Hong Y, Dong G, Li Q, Wang V, Liu M, Jiang G, Bao D, Zhou J. Effects of pre-exercise H2 inhalation on physical fatigue and related prefrontal cortex activation during and after high-intensity exercise. Front Physiol. 2022 Sep 2;13:988028. eCollection 2022. [CrossRef]
- Eda, N.; Tsuno, S.; Nakamura, N.; Sone, R.; Akama, T.; Matsumoto, M. Effects of IntestinalBacterial Hydrogen Gas Production on Muscle Recovery following Intense Exercise in Adult Men: A Pilot Study. Nutrients 2022, 14, 4875. [Google Scholar] [CrossRef] [PubMed]
- Perry RJ, Peng L, Barry NA, Cline GW, Zhang D, Cardone RL, Petersen KF, Kibbey RG, Goodman AL, Shulman GI. Acetate mediates a microbiome–brain–β- cell axis to promote metabolic syndrome. Nature 2016; 534: 213-217. [CrossRef]
- De Vadder F, Kovatcheva-Datchary P, Goncalves D, Vinera J, Zitoun C, Duchampt A, Bäckhed F, Mithieux G. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell 2014; 156: 84-96. [CrossRef]
- Levitt, MD. Excretion of hydrogen gas in man. N Engl J Med 1969; 281: 122-127. [CrossRef]
- Hajishengallis G, Darveau RP, Curtis MA. The keystone-pathogen hypothesis. Nat Rev Microbiol 2012; 10 (10): 717–725. [CrossRef]
- Lupp, C.; Robertson, M.L.; Wickham, M.E.; Sekirov, I.; Champion, O.L.; Gaynor, E.C.; Finlay, B.B. Host-mediated inflammation disrupts the intestinal microbiota and promotes the overgrowth of Enterobacteriaceae. Cell Host Microbe 2007, 2, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.M. Introduction to the special focus issue on the impact of diet on gut microbiota composition and function and future opportunities for nutritional modulation of the gut microbiome to improve human health. Gut Microbes 2017, 8, 75–81. [Google Scholar] [CrossRef] [PubMed]
- LeBaron TW, Kura B, Kalocayova B, Tribulova N, Slezak J. A New Approach for the Prevention and Treatment of Cardiovascular Disorders. Molecular Hydrogen Significantly Reduces the Effects of Oxidative Stress. Molecules 2019; 24(11): 276. [CrossRef]
- LeBaron TW, Sharpe R, Ohno K. Electrolyzed-Reduced Water: Review I. Molecular Hydrogen Is the Exclusive Agent Responsible for the Therapeutic Effects. Int J Mol Sci. 2022 Nov 25;23 (23):14750. [CrossRef]
- Baptista LC, Sun Y, Carter CS, Buford TW. Crosstalk Between the Gut Microbiome and Bioactive Lipids: Therapeutic Targets in Cognitive Frailty. Front Nutr. 2020 Mar 11;7:17. [CrossRef]
- Carr, A.C.; McCall, M.R.; Frei, B. Oxidation of LDL by myeloperoxidase and reactive nitrogen species: reaction pathways and antioxidant protection. Arterioscler Thromb Vasc Biol 2000, 20, 1716–1723. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Kisugi, R. Mechanisms of LDL oxidation. Clin Chim Acta 2010, 411, 1875–1882. [Google Scholar] [CrossRef]
- Todorovic N, Fernández, Landa, J, Santibañez A., Kura, B, Stajer V, Korovljev D, Ostojic, SM. The Effects of Hydrogen-Rich Water on Blood Lipid Profiles in Clinical Populations: A Systematic Review and Meta-Analysis. Pharmaceuticals 2023;16:142. [CrossRef]
- Ge L, Yang M, Yang NN, Yin XX, Song WG. Molecular hydrogen: a preventive and therapeutic medical gas for various diseases. Oncotarget. 2017;8(60):102653-102673. [CrossRef]
- Christl, S.U.; Murgatroyd, P.R.; Gibson, G.R.; Cummings, J.H. Production, metabolism, and excretion of hydrogen in the large intestine. Gastroenterology 1992, 102 Pt 1, 1269–77. [Google Scholar] [CrossRef]
- Suzuki A, Ito M, Hamaguchi T, Mori H, Takeda Y, Baba R, Watanabe T, Kurokawa K, Asakawa S, Hirayama M, Ohno K. Quantification of hydrogen production by intestinal bacteria that are specifically dysregulated in Parkinson's disease. PLoS One. 2018, 13(12):e0208313. [CrossRef]
- Ishibashi, T. Therapeutic Efficacy of Molecular Hydrogen: A New Mechanistic Insight. Curr Pharm Des. 2019;25(9):946-955. [CrossRef]
- Dole, M.; Wilson, F.R.; Fife, W.P. Hyperbaric hydrogen therapy: A possible treatment for cancer. Science 1975, 190, 152–154. [Google Scholar] [CrossRef]
- Ohsawa, I.; Ishikawa, M.; Takahashi, K.; Watanabe, M, Nishimaki, K, Yamagata, K, Katsura, K. I., Katayama Y, Asoh, S, Ohta S. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat. Med. 2007, 13, 688–694. [Google Scholar] [CrossRef]
- Nakao A, Toyoda Y, Sharma P, Evans M, Guthrie N. Effectiveness of hydrogen rich water on antioxidant status of subjects with potential metabolic syndrome—an open label pilot study. Journal of Clinical Biochemistry and Nutrition 2010; 46 (2): 140-149. [CrossRef]
- Kajiyama S, Hasegawa G, Asano M, Hosoda H, Fukui M, Nakamura N, Kitawaki J, Imai S, Nakano K, Ohta M, Adachi T, Obayashi H, Yoshikawa T. Supplementation of hydrogen-rich water improves lipid and glucose metabolism in patients with type 2 diabetes or impaired glucose tolerance. Nutr Res 2008; 28 (3): 137-143. [CrossRef]
- Guihua, L.; Tongsu, N. Efficacy and safety of hydrogen inhalation therapy in patients with type 2 diabetes mellitus with poor response to metformin. Advances in Clinical Medicine 2022, 12, 9605–9612. [Google Scholar]
- Zhao Z, Ji H, Zhao Y, Liu Z, Sun R, Li Y and Ni T. Effectiveness and safety of hydrogen inhalation as an adjunct treatment in Chinese type 2 diabetes patients: A retrospective, observational, double-arm, real-life clinical study. Front. Endocrinol. 2023;13:1114221. [CrossRef]
- Korovljev D, Trivic T, Drid P, Ostojic SM. Molecular hydrogen affects body composition, metabolic profiles, and mitochondrial function in middle-aged overweight women. Ir J Med Sci 2018; 187 (1): 85-89. [CrossRef]
- Song, G.; Li, M.; Sang, H.; Zhang, L.; Li, X.; Yao, S.; Yu, Y.; Zong, C.; Xue, Y.; Qin, S. Hydrogen-rich water decrease serum low-density lipoprotein cholesterol levels and improves high density lipoprotein function in patients with potential metabolic syndrome. J Lipid Res 2013, 54, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Song G, Lin Q, Zhao H, Liu M, Ye F, Sun Y, Yu Y, Guo S, Jiao P, Wu Y, Ding G, Xiao Q, Qin S. Hydrogen activates ATP-binding cassette transporter A1-dependent efflux ex vivo and improves high-density lipoprotein function in patients with hypercholesterolemia: A double-blinded, randomized, and placebo-controlled trial. J Clin Endocrinol Metab 2015; 100 (7): 2724-2733. [CrossRef]
- Tao, G.; Zhang, G.; Chen, W.; Yang, C.; Xue, Y.; Song, G.; Qin, S. A randomized, placebo-controlled clinical trial of hydrogen/oxygen inhalation for non-alcoholic fatty liver disease. J Cell Mol Med. 2022, 26, 4113–4123. [Google Scholar] [CrossRef] [PubMed]
- Kura, B.; Szantova, M.; LeBaron, T.W.; Mojto, V.; Barancik, M.; Szeiffova Bacova, B.; Kalocayova, B.; Sykora, M.; Okruhlicova, L.; Tribulova, N.; et al. Biological Effects of Hydrogen Water on Subjects with NAFLD: A Randomized, Placebo-Controlled Trial. Antioxidants 2022, 11, 1935. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.B.; Nabavizadeh, F.; Fedacko, J.; Pella, D.; Vanova, N.; Jakabcin, P.; Fatima, G.; Horuichi, R.; Takahashi, T.; Mojto, V.; et al. Dietary Approaches to Stop Hypertension via Indo-Mediterranean Foods, May Be Superior to DASH Diet Intervention. Nutrients 2023, 15, 46. [Google Scholar] [CrossRef]
- Sugai K, Tamura T, Sano M, Uemura S, Fujisawa M, Katsumata Y, Endo J, Yoshizawa J, Homma K, Suzuki M, Kobayashi E, Sasaki J, Hakamata Y. Daily inhalation of hydrogen gas has a blood pressure-lowering effect in a rat model of hypertension. Sci Rep. 2020 Nov 26;10(1):20173. [CrossRef]
- Nakayama M, et al. Novel haemodialysis (HD) treatment employing molecular hydrogen (H2)-enriched dialysis solution improves prognosis of chronic dialysis patients: A prospective observational study. Sci. Rep. 2018;8:254. [CrossRef]
- Liu B, Jiang X, Xie Y, Jia X, Zhang J, Xue Y and Qin S. The effect of a low dose hydrogen-oxygen mixture inhalation in midlife/older adults with hypertension: A randomized, placebo-controlled trial. Front. Pharmacol. 13:1025487. [CrossRef]
- Chen, C.H.; Manaenko, A.; Zhan, Y.; Liu, W.W.; Ostrowki, R.P.; Tang, J.; Zhang, J.H. Hydrogen gas reduced acute hyperglycemia-enhanced hemorrhagic transformation in a focal ischemia rat model. Neuroscience 2010, 169, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Nagatani, K.; Wada, K.; Takeuchi, S.; Kobayashi, H.; Uozumi, Y.; Otani, N.; Fujita, M.; Tachibana, S.; Nawashiro, H. Effect of hydrogen gas on the survival rate of mice following global cerebral ischemia. Shock (Augusta, Ga) 2012, 37, 645–652. [Google Scholar] [CrossRef]
- Manaenko, A.; Lekic, T.; Ma, Q.; Ostrowski, R.P.; Zhang, J.H.; Tang, J. Hydrogen inhalation is neuroprotective and improves functional outcomes in mice after intracerebral hemorrhage. Acta Neurochir Suppl. 2011, 111, 179–183. [Google Scholar]
- Ono H, Nishijima Y, Adachi N, et al. A basic study on molecular hydrogen (H2) inhalation in acute cerebral ischemia patients for safety check with physiological parameters and measurement of blood H2 level. Med Gas Res, 2 (2012), p. 21. [CrossRef]
- Ono H, Nishijima Y, Ohta S, Sakamoto M, Kinone K, Tohru Horikosi T, et al. Hydrogen Gas Inhalation Treatment in Acute Cerebral Infarction: A Randomized Controlled Clinical Study on Safety and Neuroprotection. Journal of Stroke and Cerebrovascular Diseases,2017; 26:2587-94. [CrossRef]
- Yao W, Shen L, Ma Z et al. Efficacy and safety of hydrogen gas versus standard therapy in Chinese patients with cerebral infarction: A pilot study Trop. J Pharm Res 2022, 21, 671. [Google Scholar]
- Gvozdjáková A, Kucharská J, Kura B, Vančová O, Rausová Z, Sumbalová Z, Uličná O, Slezák J. A new insight into the molecular hydrogen effect on coenzyme Q and mitochondrial function of rats. Can J Physiol Pharmacol. 2020 Jan;98(1):29-34. [CrossRef]
- Kucharská J, Gvozdjáková A, Kura B, et al. Effect of molecular hydrogen on coenzyme Q in plasma, myocardial tissue and mitochondria of rats. J Nutr Health Food Eng. 2018;8(5): 362‒364. [CrossRef]
- Sobue S, Inoue C, Hori F, Qiao S, Murate T, Ichihara M. Molecular hydrogen modulates gene expression via histone modification and induces the mitochondrial unfolded protein response. Biochem Biophys Res Commun. 2017 Nov 4;493(1):318-324. [CrossRef]
- Zhang, Y.; Sun, Q.; He, B.; Xiao, J.; Wang, Z.; Sun, X. Anti-inflammatory effect of hydrogen-rich saline in a rat model of regional myocardial ischemia and reperfusion. Int J Cardiol 2011, 148, 91–95. [Google Scholar] [CrossRef]
- Turer A.T., Hill J.A. Pathogenesis of Myocardial Ischemia-Reperfusion Injury and Rationale for Therapy. Am. J. Cardiol. 2010;37:761–771. [CrossRef]
- Xia Y., Zweier J.L. Substrate control of free radical generation from xanthine oxidase in the postischemic heart. J. Biol. Chem. 1995;270:18797–18803. [CrossRef]
- Zorov D.B., Filburn C.R., Klotz L.-O., Zweier J.L., Sollott S.J. Reactive Oxygen Species (ROS)-induced ROS Release: A New Phenomenon Accompanying Induction of the Mitochondrial Permeability Transition in Cardiac Myocytes. J. Exp. Med. Bull. 2000;192:1001–1014. [CrossRef]
- Zhang Y., Tan S., Xu J., Wang T. Hydrogen Therapy in Cardiovascular and Metabolic Diseases: From Bench to Bedside. Cell. Physiol. Biochem. 2018;47:1–10. [CrossRef]
- Ichihara, G.; Katsumata, Y.; Moriyama, H.; Kitakata, H.; Hirai, A.; Momoi, M.; Ko, S.; Shinya, Y.; Kinouchi, K.; Kobayashi, E.; et al. Pharmacokinetics of hydrogen after ingesting a hydrogen-rich solution: A study in pigs. Heliyon 2021, 7, e08359. [Google Scholar] [CrossRef]
- Braunwald, E. , Kloner R.A. Myocardial reperfusion: A double-edged sword? J. Clin. Invest. 1985, 76, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Yellon, D.M. Preconditioning and postconditioning: United at reperfusion. Pharmacol. Ther. 2007, 116, 173–191. [Google Scholar] [CrossRef]
- Ma, X. L, Weyrich A.S., Lefer D.J., Lefer A.M. Diminished basal nitric oxide release after myocardial ischemia and reperfusion promotes neutrophil adherence to coronary endothelium. Circ. Res. 1993, 72, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Chen, H.; Wu, Q.; Xie, K. Hydrogen-rich saline alleviates inflammation and apoptosis in myocardial I/R injury via PINK-mediated autophagy. Int J Mol Med. 2019, 44, 1048–1062. [Google Scholar] [CrossRef]
- Katsumata Y, Fumiya Sano F, Takayuki Abe T, et al. The Effects of Hydrogen Gas Inhalation on Adverse Left Ventricular Remodeling After Percutaneous Coronary Intervention for ST-Elevated Myocardial Infarction― First Pilot Study in Humans. Circulation Journal 2017, 81, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Lin YT, Shi QQ, Zhang L, Yue CP, He ZJ, Li XX, et al. Hydrogen-rich water ameliorates neuropathological impairments in a mouse model of Alzheimer's disease through reducing neuroinflammation and modulating intestinal microbiota. Neural Regeneration Research 2022, 17, 409–417. [Google Scholar] [CrossRef]
- Tan X, Shen F, Dong WL, Yang Y, Chen G. The role of hydrogen in Alzheimer's disease. Med Gas Res. 2019 Jan 9;8(4):176-180. [CrossRef]
- Wen D, Zhao P, Hui R, et al. Hydrogen-rich saline attenuates anxiety-like behaviors in morphine-withdrawnmice. Neuropharmacology 2017, 118, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Yoshii Y, Inoue T, Uemura Y, et al. Complexity of stomach-brain interaction induced by molecular hydrogen in Parkinson’s disease model mice. Neurochem Res. 2017, 42, 2658–2665. [Google Scholar] [CrossRef]
- Zanini, D.; Todorovic, N.; Korovljev, D.; Stajer, V.; Ostojic, J.; Purac, J.; Kojic, D.; Vukasinovic, E.; Djordjievski, S.; Sopic, M.; Guzonjic, A.; Ninic, A.; Erceg, S.; Ostojic, S.M. The effects of 6-month hydrogen-rich water intake on molecular and phenotypic biomarkers of aging in older adults aged 70 years and over: A randomized controlled pilot trial. Experimental Gerontology 2021, 155. [Google Scholar] [CrossRef]
- Guo JD, Li L, Shi YM, Wang HD, Hou SX. Hydrogen water consumption prevents osteopenia in ovariectomized rats. Br J Pharmacol. 2013 Mar;168(6):1412-20. [CrossRef]
- Sun Y, Shuang F, Chen DM, Zhou RB. Treatment of hydrogen molecule abates oxidative stress and alleviates bone loss induced by modeled microgravity in rats. Osteoporos Int. 2013 Mar;24(3):969-78. [CrossRef]
- Yang, Q.; Ji, G.; Pan, R.; Zhao, Y.; Yan, P. Protective effect of hydrogen-rich water on liver function of colorectal cancer patients treated with mFOLFOX6 chemotherapy. Mol Clin Oncol. 2017, 7, 891–896. [Google Scholar] [CrossRef]
- Mohd Noor, MNZ., Alauddin, AS., Wong, YH., Looi, CY., Wong, EH., Madhavan, P., Yeong, CHA Systematic Review of Molecular Hydrogen Therapy in Cancer management Asian Pacific Journal of Cancer Prevention, 2023; 24(1): 37-47. ,. [CrossRef]
- Hirano, S.I.; Aoki, Y.; Li, X.K.; Ichimaru, N.; Takahara, S.; Takefuji, Y. Protective effects of hydrogen gas inhalation on radiation-induced bone marrow damage in cancer patients: a retrospective observational study. Med Gas Res. 2021, 11, 104–109. [Google Scholar]
- Dole, M.; Wilson, F.R.; Fife, W.P. Hyperbaric hydrogen therapy: a possible treatment for cancer. Science 1975, 190, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Runtuwene, J.; Amitani, H.; Amitani, M.; Asakawa, A.; Cheng, K.C.; Inui, A. Hydrogen-water enhances 5-fluorouracil-induced inhibition of colon cancer. Peer J. 2015, 3, e859. [Google Scholar] [CrossRef]
- Asgharzadeh, F.; Tarnava, A.; Mostafapour, A.; Khazaei, M.; LeBaron, T.W. Hydrogen-rich water exerts anti-tumor effects comparable to 5-fluorouracil in a colorectal cancer xenograft model. World J Gastrointest Oncol 2022, 14, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa T, Ito M, Hasegawa et al. Molecular Hydrogen Enhances Proliferation of Cancer Cells That Exhibit Potent Mitochondrial Unfolded Protein Response. Int. J. Mol. Sci. 2022, 23, 2888. [Google Scholar] [CrossRef] [PubMed]
- Wang B, Li Z, Mao L, Zhao M, Yang B, Tao X, Li Y, Yin G. Hydrogen: A Novel Treatment Strategy in Kidney Disease. Kidney Dis (Basel). 2022 Jan 12;8(2):126-136. [CrossRef]
- Lu Y, Li CF, Ping NN, Sun YY, Wang Z, Zhao GX, et al. Hydrogen-rich water alleviates cyclosporine A-induced nephrotoxicity via the Keap1/Nrf2 signaling pathway. J Biochem Mol Toxicol. 2020, 34, e22467. [Google Scholar]
- Xing Z, Pan W, Zhang J, Xu X, Zhang X, He X, et al. Hydrogen rich water attenuates renal injury and fibrosis by regulation transforming growth factor-β induced Sirt1. Biol Pharm Bull. 2017, 40, 610–5. [Google Scholar] [CrossRef] [PubMed]
- Chen J, Zhang H, Hu J, Gu Y, Shen Z, Xu L, et al. Hydrogen-rich saline alleviates kidney fibrosis following AKI and retains Klotho expression. Front Pharmacol. 2017, 8, 499. [Google Scholar] [CrossRef]
- Li J, Hong Z, Liu H, Zhou J, Cui L, Yuan S, et al. Hydrogen-rich saline promotes the recovery of renal function after ischemia/reperfusion injury in rats via anti-apoptosis and anti-inflammation. Front Pharmacol. 2016, 7, 106. [Google Scholar]
- Xu X, He X, Liu J, Qin J, Ye J, Fan M. Protective effects of hydrogen-rich saline against renal ischemia-reperfusion injury by increased expression of heme oxygenase-1 in aged rats. Int J Clin Exp Pathol. 2019, 12, 1488–1496. [Google Scholar]
- Nishida T, Hayashi T, Inamoto T, Kato R, Ibuki N, Takahara K, et al. Dual gas treatment with hydrogen and carbon monoxide attenuates oxidative stress and protects from renal ischemia-reperfusion injury. Transplant Proc. 2018, 50, 250–8. [Google Scholar] [CrossRef]
- Lu H, Ding J, Liu W, Peng Z, Chen W, Sun X, et al. UPLC/MS-based metabolomics investigation of the protective effect of hydrogen gas inhalation on mice with calcium oxalate-induced renal injury. Biol Pharm Bull. 2018, 41, 1652–1658. [Google Scholar] [CrossRef]
- Zheng Z, Zheng F. Immune cells and inflammation in diabetic nephropathy. J Diabetes Res. 2016, 2016, 1841690. [Google Scholar]
- Trionfetti F, Marchant V, González-Mateo GT et al. Novel Aspects of the Immune Response Involved in the Peritoneal Damage in Chronic Kidney Disease Patients under Dialysis. Int. J. Mol. Sci. 2023; 24(6):5763. [CrossRef]
- Fischer BM, Voynow JA, Ghio AJ. COPD: balancing oxidants and antioxidants. Int J Chron Obstruct Pulmon Dis. 2015;10:261-76. [CrossRef]
- Wang ST, Bao C, He Y, Tian X, Yang Y, Zhang T, Xu KF. Hydrogen gas (XEN) inhalation ameliorates airway inflammation in asthma and COPD patients. QJM. 2020 Dec 1;113(12):870-875. [CrossRef]
- Suzuki, Y. , Sato, T., Sugimoto, M., Baskoro, H., Karasutani, K., Mitsui, A., Nurwidya, F., Arano, N., Kodama, Y., Hirano, S.I. and Ishigami, A.. Hydrogen-rich pure water prevents cigarette smoke-induced pulmonary emphysema in SMP30 knockout mice. Biochemical and biophysical research communications 2017, 492, 74–81. [Google Scholar] [CrossRef]
- Singh RB, Halabi G, Fatima G, Rai RH, Tarnava AT, LeBaron TW. Molecular hydrogen as an adjuvant therapy may be associated with increased oxygen saturation and improved exercise tolerance in a COVID-19 patient. Clin Case Reports 9: e05039. | 1 of 6. [CrossRef]
- Zheng, ZG., Sun, WZ., Hu, JY. et al. Hydrogen/oxygen therapy for the treatment of an acute exacerbation of chronic obstructive pulmonary disease: results of a multicenter, randomized, double-blind, parallel-group controlled trial. Respir Res 2021;22, 149. [CrossRef]
- Kohama K, Yamashita H, Aoyama-Ishikawa M, Takahashi T, Billiar TR, Nishimura T, Kotani J, Nakao A. Hydrogen inhalation protects against acute lung injury induced by hemorrhagic shock and resuscitation. Surgery. 2015;158:399–407. [CrossRef]
- Yang F, Yue R, Luo X, Liu R, Huang X. Hydrogen: A Potential New Adjuvant Therapy for COVID-19 Patients. Front Pharmacol. 2020;11:543718. [CrossRef]
- Wang M, Peng J, Hui J, Hou D, Li W, Yang J. Hydrogen therapy as an effective and novel adjuvant treatment against COVID-19. QJM. 2021;114(1):74-5. [CrossRef]
- Deryugina, A.V.; Danilova, D.A.; Pichugin, V.V.; Brichkin, Y.D. The Effect of Molecular Hydrogen on Functional States of Erythrocytes in Rats with Simulated Chronic Heart Failure. Life 2023, 13, 418. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, Y.; Zhang, J. Saturated hydrogen saline attenuates endotoxin-induced lung dysfunction. J Surg Res. 2015, 198, 41–49. [Google Scholar] [CrossRef]
- Singh RB, Gupta AK, Fatima G, Fedacko J et al. Can molecular hydrogen therapy enhance oxygen saturation among patients with chronic lung disease. Presented and abstracted in the First conference of the European Academy of Molecular Hydrogen Research in Biomedicine. Smolenice Castle, Slovakia, (Abstract Page 69) Oct 17-20,2022.
- Ishibashi, T.; Kawamoto, K.; Matsuno, K.; Ishihara, G.; Baba, T.; Komori, N. Peripheral endothelial function can be improved by daily consumption of water containing over 7 ppm of dissolved hydrogen: A randomized controlled trial. PLoS One 2020, 15, e0233484. [Google Scholar] [CrossRef]
- Gu, Q. , Liu, B., Xue, J., Zhao, M., Zhang, X., Wang, M., Zhang, M., Xue, Y., Qin, S. (2020). Effects of drinking hydrogen-rich water in men at risk of peripheral arterial disease: A randomized placebo-controlled trial. [CrossRef]
- Asada, R.; Tazawa, K.; Sato, S.; Miwa, N. Effects of hydrogen-rich water prepared by alternating-current-electrolysis on antioxidant activity, DNA oxidative injuries, and diabetes-related markers. Medical Gas Research 2020, 10, 114–121. [Google Scholar] [CrossRef]
- Kamimura N, Ichimiya H, Iuchi K, Ohta S. Molecular hydrogen stimulates the gene expression of transcriptional coactivator PGC-1α to enhance fatty acid metabolism. NPJ Aging Mech Dis. 2016 Apr 28;2:16008. eCollection 2016. [CrossRef]
- Nagatani K, Nawashiro H, Takeuchi S, et al. Safety of intravenous administration of hydrogen-enriched fluid in patients with acute cerebral ischemia: initial clinical studies. Med Gas Res. 2013, 3, 13. [Google Scholar] [CrossRef]
- Zanini, D.; Stajer, V.; Ostojic, S.M. Hydrogen vs. caffeine for improved alertness in sleep-deprived humans. Neurophysiology 2020, 52, 67–72. [Google Scholar] [CrossRef]
- LeBaron, W. T. , Kharman, J., McCullough, L. Michael. (2021). An H2-infused, nitric oxide-producing functional beverage as a neuroprotective agent for TBIs and concussions. Journal of Integrative Neuroscience 2021, 20. [Google Scholar]
- Takeuchi, S.; Kumagai, K.; Toyooka, T.; Otani, N.; Wada, K.; Mori, K. Intravenous Hydrogen Therapy With Intracisternal Magnesium Sulfate Infusion in Severe Aneurysmal Subarachnoid Hemorrhage. Stroke 2021, 52, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Hirano SI, Aoki Y, Li XK, Ichimaru N, Takahara S, Takefuji Y. Protective effects of hydrogen gas inhalation on radiation-induced bone marrow damage in cancer patients: a retrospective observational study. Med Gas Res. 2021 Jul-Sep;11(3):104-109. [CrossRef]
- Chen JB., Kong, XF., Qian, W, Mu, F., Lu, TY., Lu, YY., & Xu, KC. Two weeks of hydrogen inhalation can significantly reverse adaptive and innate immune system senescence patients with advanced non-small cell lung cancer: A self-controlled study. Medical Gas Research, 2020;10(4), 149–154. 127.Akagi J, Baba H. Hydrogen gas activates coenzyme Q10 to restore exhausted CD8+ T cells, especially PD-1+Tim3+terminal CD8+ T cells, leading to better nivolumab outcomes in patients with lung cancer. Oncol Lett. 2020 Nov;20(5):258. doi: 10.3892/ol.2020.12121.
- Korovljev, D.; Trivic, T.; Stajer, V.; Drid, P.; Sato, B.; Ostojic, S.M. Short-term H2 inhalation improves cognitive function in older women: A pilot study. International Journal of Gerontology 2019, 14, 149–150. [Google Scholar]
- Lv X, Lu Y, Ding G, et al. Hydrogen Intake Relieves Alcohol Consumption and Hangover Symptoms in Healthy Adults: a Randomized and Placebo-Controlled Crossover Study [published online ahead of print, 2022 Sep 16]. Am J Clin Nutr. 2022;nqac261. [CrossRef]
- Okada M, Ogawa H, Takagi T, Nishihara E, Yoshida T, Hyodo J, Shinomori Y, Honda N, Fujiwara T, Teraoka M, Yamada H, Hirano S-i and Hato N. A double-blinded, randomized controlled clinical trial of hydrogen inhalation therapy for idiopathic sudden sensorineural hearing loss. Front. Neurosci. 2022;16:1024634. [CrossRef]
- Tamura, T.; Suzuki, M.; Hayashida, K.; Kobayashi, Y.; Yoshizawa, J.; Shibusawa, T.; Sano, M.; Hori, S.; Sasaki, J. Hydrogen gas inhalation alleviates oxidative stress in patients with post-cardiac arrest syndrome. Journal of Clinical Biochemistry and Nutrition 2020, 67, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Kiuchi, M.; Higashimura, Y.; Naito, Y.; Koyama, K. The effects of ingestion of hydrogen-dissolved alkaline electrolyzed water on stool consistency and gut microbiota: a double-blind randomized trial. Medical Gas Research 2021, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Danilova DA, Brichkin YD, Medvedev AP, Pichugin VV, Fedorov SA, Taranov EV, Nazarov EI, Ryazanov MV, Bolshukhin GV, Deryugina AV. Application of Molecular Hydrogen in Heart Surgery under Cardiopulmonary Bypass. Sovrem Tekhnologii Med. 2021;13(1):71-75. [CrossRef]
- Increased Sympathetic Cardiac Activity in Healthy Females, Hydrogen Water.
- Botek, M.; Sládečková; B; Krejčí; J; Pluháček, F. ; Najmanová; E Acute hydrogen-rich water ingestion stimulates cardiac autonomic activity in healthy females. Acta Gymnica 2021, 51, e2021–009. [Google Scholar] [CrossRef]
- Li, D.; Yan, M. Clinical assessment of hydrogen-rich water and oxycodone hydrochloride controlled-release tablets in the treatment of malignant neuropathic pain. Journal of Chinese Physician 2016, 18, 1329–1331. [Google Scholar]
- Kubota, M.; Kawashima, M.; Inoue, S.; Imada, T.; Nakamura, S.; Kubota, S.; Watanabe, M.; Takemura, R.; Tsubota, K. Randomized, crossover clinical efficacy trial in humans and mice on tear secretion promotion and lacrimal gland protection by molecular hydrogen. Scientific Reports 2021, 11, 6434. [Google Scholar] [CrossRef]
- Iketani, M.; Sekimoto, K.; Igarashi, T.; Takahashi, M.; Komatsu, M.; Sakane, I.; Takahashi, H.; Kawaguchi, H.; Ohtani-Kaneko, R.; Ohsawa, I. Administration of hydrogen-rich water prevents vascular aging of the aorta in LDL receptor-deficient mice. Sci Rep. 2018 Nov 14;8(1):16822. [CrossRef]
- Kang, K.M.; Kang, Y.N.; Choi, I.B.; Gu, Y.; Kawamura, T.; Toyoda, Y.; Nakao, A. Effects of drinking hydrogen-rich water on the quality of life of patients treated with radiotherapy for liver tumors. Med Gas Res. 2011, 1, 11. [Google Scholar] [CrossRef]
Figure 1.
Pathways for development of non-communicable diseases.
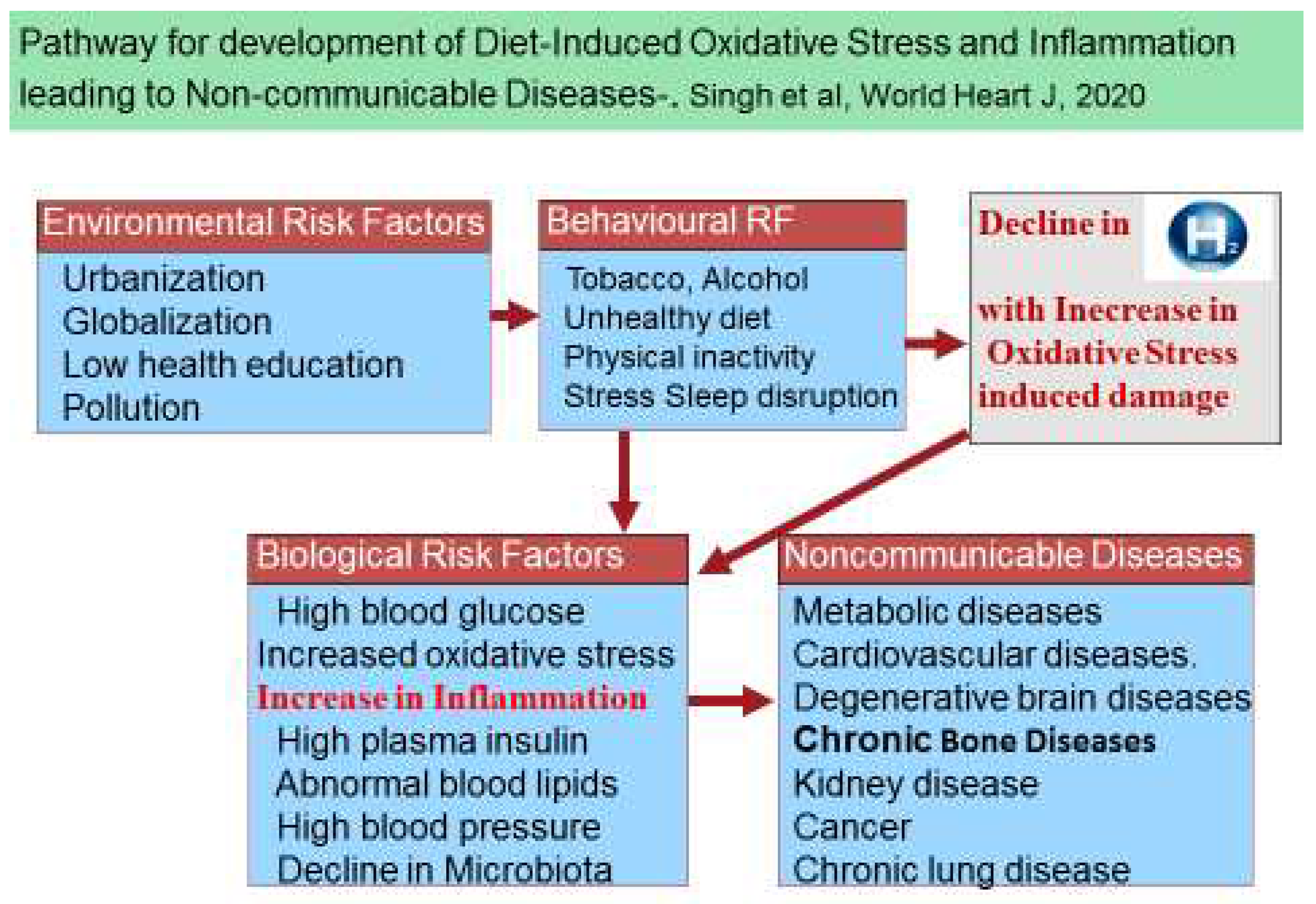
Figure 2.
Mechanism of production and inhibition of molecular hydrogen due to diets via microbiota in the gut, and its effects on anti-inflammatory molecules and risk of chronic diseases.
Figure 2.
Mechanism of production and inhibition of molecular hydrogen due to diets via microbiota in the gut, and its effects on anti-inflammatory molecules and risk of chronic diseases.
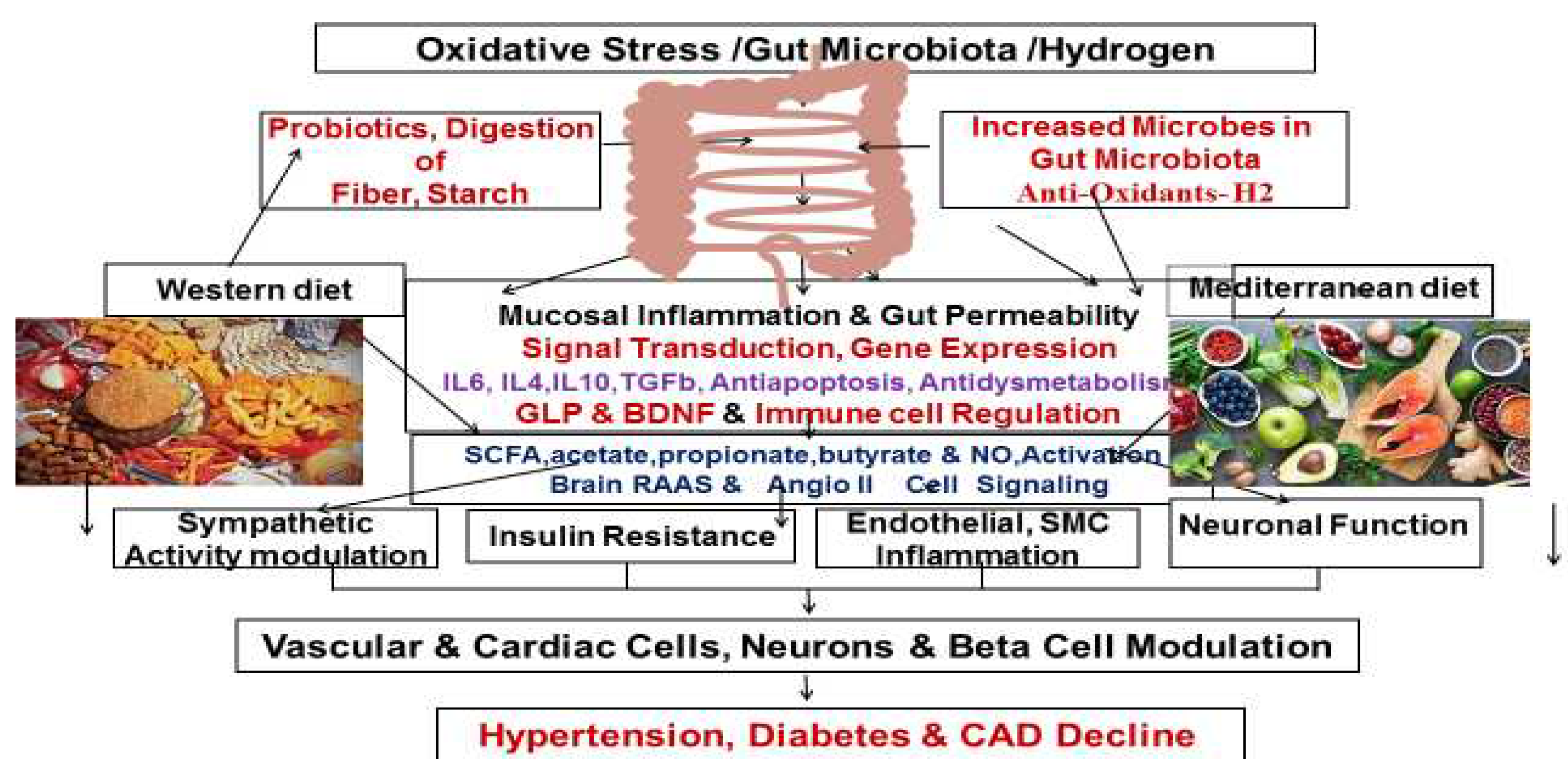
Figure 3.
Molecular mechanisms of hydrogen action resulting in to beneficial effects. (Modified from Ichihara et al, reference 14).
Figure 3.
Molecular mechanisms of hydrogen action resulting in to beneficial effects. (Modified from Ichihara et al, reference 14).
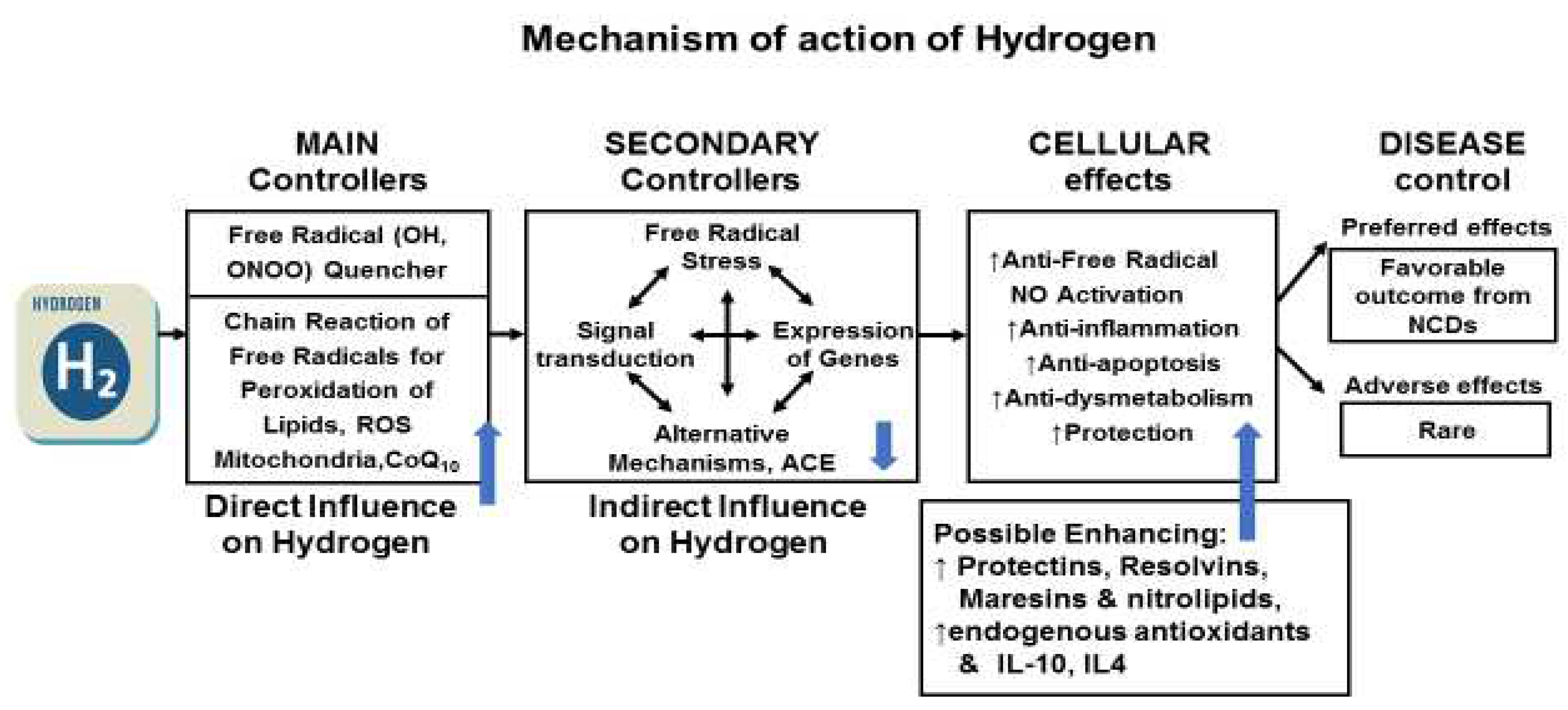
Figure 4.
Forest plots of included studies comparing the effects of HRW supplementation on blood lipids. (Adapted from reference 42).
Figure 4.
Forest plots of included studies comparing the effects of HRW supplementation on blood lipids. (Adapted from reference 42).
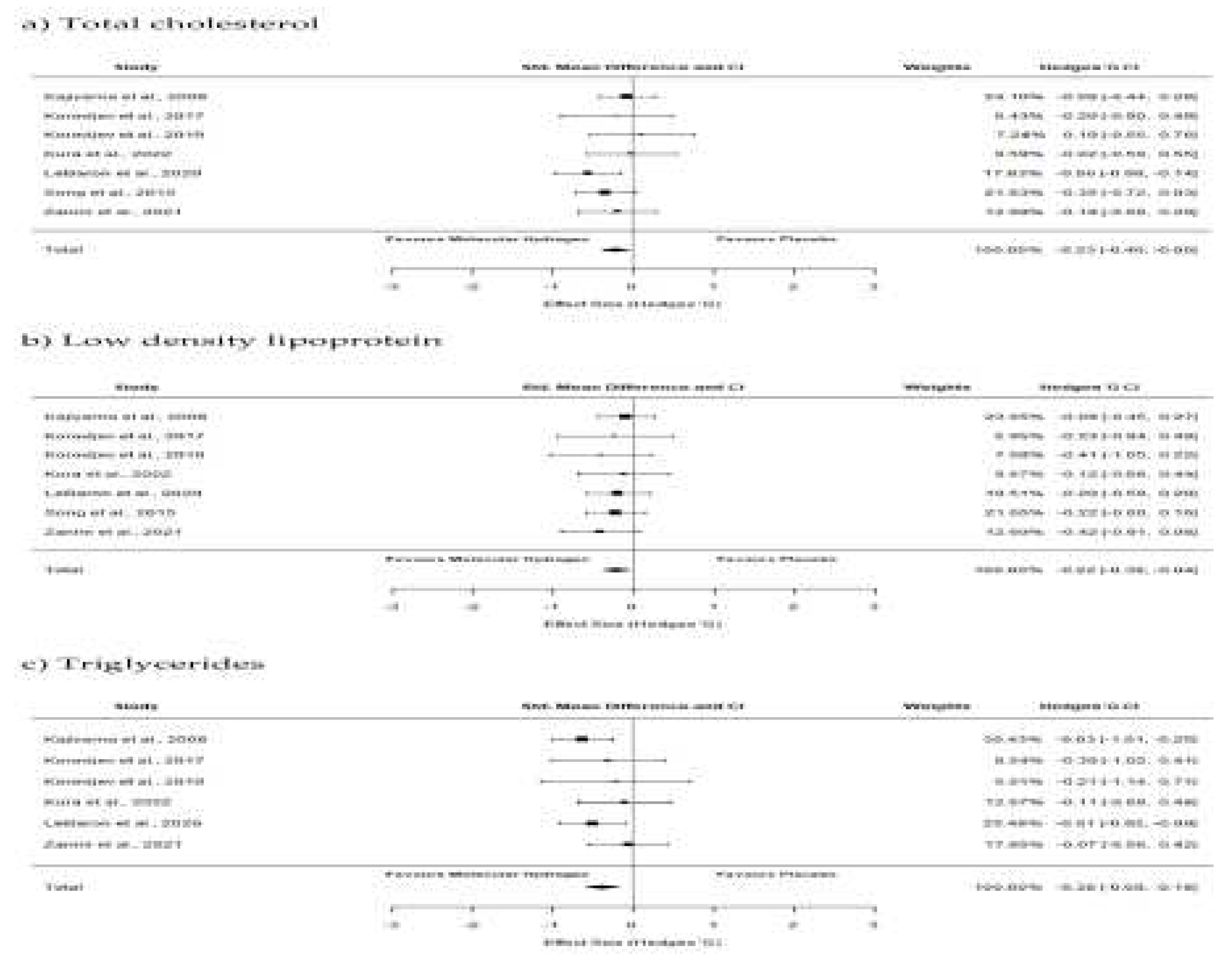
Figure 5.
Mechanisms of the effects of hydrogen therapy on pro-inflammatory biomarkers and non-communicable diseases. (Modified from LeBaron et al, 2019, reference 17).
Figure 5.
Mechanisms of the effects of hydrogen therapy on pro-inflammatory biomarkers and non-communicable diseases. (Modified from LeBaron et al, 2019, reference 17).
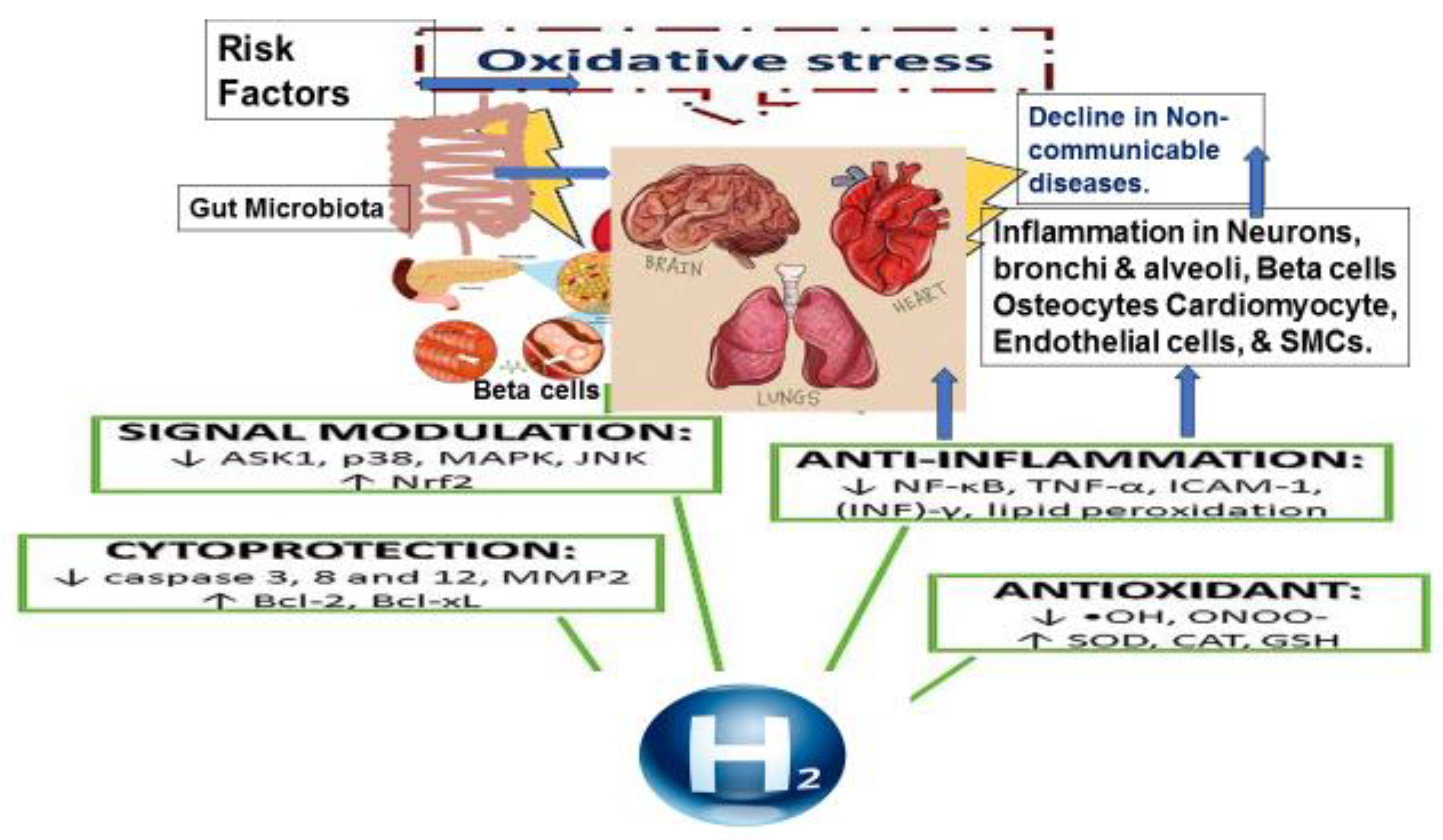

Table 1.
Effects of hydrogen rich water on blood lipoproteins in patients with metabolic syndrome [25].
Table 1.
Effects of hydrogen rich water on blood lipoproteins in patients with metabolic syndrome [25].
| Data | Hydrogen rich water (n-30) | Placebo (n=30) | ||
| Data, mg/dl | Baseline | After 24 weeks | Baseline | After 24 weeks |
| Cholesterol | 187.7 ± 32.4 | 169.2 ± 26.1*** | 184.3 ± 37.4 | 184.4 ± 38.6 |
| LDL-Cholesterol | 109.0 ± 34.4 | 102.5 ± 28.0 | 105.5 ± 42.0 | 106.0 ± 43.3 |
| HDL cholesterol | 41.7 ± 4.2 | 40.4 ± 1.8 | 41.8 ± 2.3 | 42.3 ± 2.4 |
| VLDL cholesterol | 37.3 ± 17.9 | 28.0 ± 11.3** | 36.8 ± 20.6 | 37.3 ± 20.5 |
| Triglycerides | 189.8 ± 93.3 | 142.4 ± 65.0** | 184.4 ± 102.8 | 185.6 ± 101.3 |
| C-reactive proteins | 0.5 ± 0.2 | 0.5 ± 0.1* | 0.6 ± 0.5 | 0.6 ± 0.5 |
*** = p value <0.0001, **= p value <0.01, *= p value <0.05, by comparison of baseline and after follow up using analysis of variance. (Modified from reference 25}.
Table 2.
Effect of hydrogen rich water on glycaemia, oxidative stress and cytokines in patients with metabolic syndrome [25].
Table 2.
Effect of hydrogen rich water on glycaemia, oxidative stress and cytokines in patients with metabolic syndrome [25].
| Hydrogen rich water(n=30) | Placebo (n=30) | |||
| Data, mg/dl | Baseline | After 24 weeks | Baseline | After 24 weeks |
| Fasting blood glucose | 121.5 ± 61.0 | 103.1 ± 33.0* | 123.9 ± 43.4 | 126.4 ± 42.3 |
| HbA1c, % | 5.8 ± 0.9 | 5.1 ± 0.2*** | 6.2 ± 1.2 | 6.1 ± 1.2 |
| TNF-α | 4.8 ± 1.2 | 3.9 ± 0.6*** | 4.8 ± 1.3 | 4.8 ± 1.3 |
| IL-6 | 1.9 ± 0.7 | 1.6 ± 0.2** | 1.6 ± 0.6 | 1.7±0.6 |
| TBARS | 2.5 ± 0.3 | 1.6 ± 0.3* | 2.5 ± 0.3 | 2.5 ± 0.3 |
| Melondialdehyde | 3.4 ± 0.2 | 2.7 ± 0.2*** | 3.4 ± 0.2 | 3.5 ± 0.2 |
| Diene conjugates | 27.8 ± 1.0 | 26.7 ± 0.5*** | 28.3 ± 0.8 | 28.3 ± 0.8 |
| Vitamin E | 23.0 ± 2.3 | 26.8 ± 1.9*** | 23.0 ± 1.5 | 23.1 ± 1.1 |
| Vitamin C | 20.7 ± 2.5 | 24.2 ± 1.8*** | 20.7 ± 2.5 | 20.8 ± 2.4 |
| Nitrite | 0.63 ± 0.06 | 0.68 ± 0.06*** | 0.66 ± 0.04 | 0.65 ± 0.03 |
| Angiotensin converting enzyme | 85.2 ± 7.8 | 80.7 ± 5.8*** | 84.5 ± 8.8 | 83.8 ± 8.7 |
*** = p value <0.0001, **= p value <0.01, *= p value <0.05, by comparison of baseline and after follow up using analysis of variance. (Modified from reference 25}.
Table 3.
Mechanisms underlying pathophysiology of myocardial ischemia/reperfusion injury. (Modified from reference 72).
Table 3.
Mechanisms underlying pathophysiology of myocardial ischemia/reperfusion injury. (Modified from reference 72).
| Alterations due I/R injury | Mechanisms |
| Ion flux | Accumulation of intracellular calcium, a2+-induced “stone-heart”, increased Na influx, Abnormal K flux. Drop in pH followed by normalization upon reperfusion. |
| Loss of myocardial membrane potential. | Opening of myocardial permeability transition pore (mPTP) |
| Reactive Oxygen Species (ROS) | Substrate-level induction of xanthine oxidase resulting in more ROS. Impaired mitochondrial function, worsen with Q10 deficiency, Neutrophil infiltration, ROS induced ROS chain. |
| Dysregulation of Nitric Oxide (NO) metaboilism. | Loss of NO vasodilation, Production of Peroxynitrite, Abnormal S-nitrosation, |
| Apoptosis | JNK Pathway, ceramide generation, cytoplasm acidification, caspase activation. |
| Autophagic cell death. | Excessive AMPK activation, Excess of induction of HIF-1α |
| Endothelial dysfunction | Cytokine,myokine, chemokine signaling. Expression of cellular adhesion markers, Impaired vasodilation. |
| Platelet aggregationAuto-immune activation | Innate immunity; complement activation, induction of TLRNeutrophil accumulation. |
JNK = c-Jun N-terminal kinase, AMPK = AMP-activated protein kinase, HIF-1α = Hypoxia-inducible factor 1-alpha.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



