Submitted:
22 April 2020
Posted:
24 April 2020
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
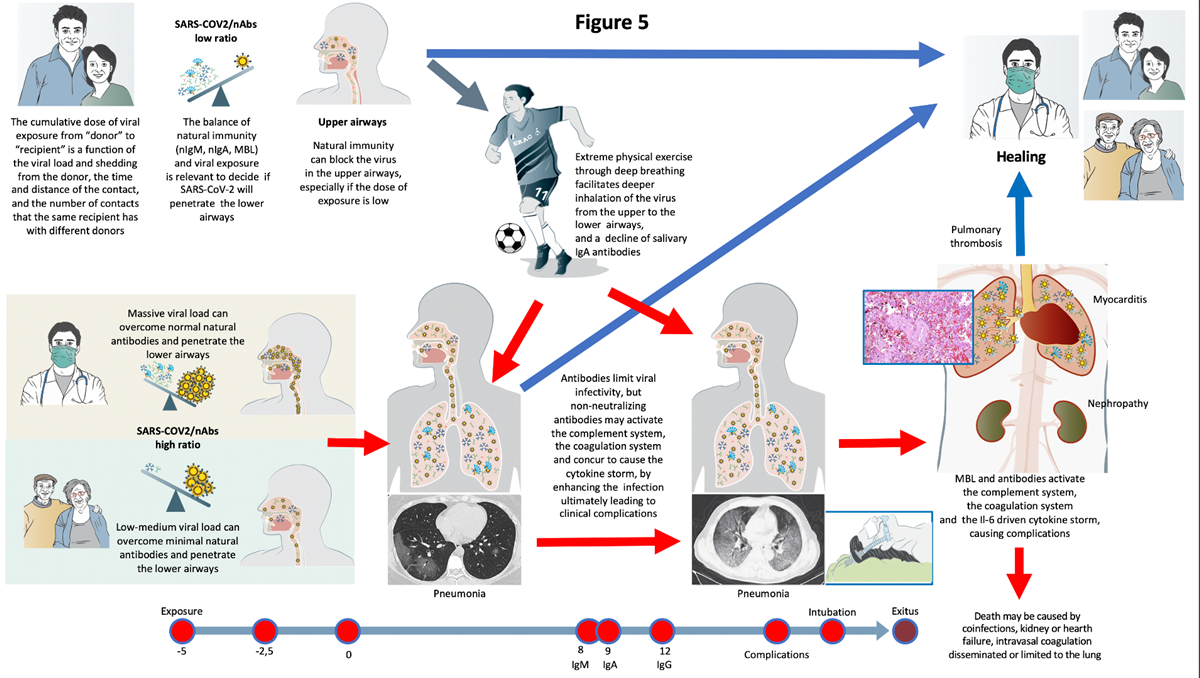
The natural history of COVID-19 caused by SARS-CoV-2 is extremely variable, ranging from asymptomatic infection, to pneumonia, and to complications eventually fatal. We propose here the first model, explaining how the outcome of first, crucial 10-15 days after infection, hangs on the balance between the cumulative dose of viral exposure and the efficacy of the local innate immune response (natural IgA and IgM antibodies, MBL). If SARS-CoV-2 runs the blockade of this innate immunity and spreads from the upper airways to the alveoli in the early phases of the infections, it can replicate with no local resistance, causing pneumonia and releasing high amounts of antigens. The delayed and strong adaptive immune response (high affinity IgM and IgG antibodies) that follows, causes severe inflammation and triggers mediator cascades (complement, coagulation, and cytokine storm) leading to complications often requiring intensive therapy and being, in some patients, fatal. Strenuous exercise and high flow air in the incubation days and early stages of COVID-19, facilitates direct penetration of the virus to the lower airways and the alveoli, without impacting on the airway’s mucosae covered by neutralizing antibodies. This allows the virus to bypass the efficient immune barrier of the upper airways mucosa in young and healthy athletes. In conclusion, whether the virus or the adaptative immune response reach the lungs first, is a crucial factor deciding the fate of the patient. This “quantitative and time-sequence dependent” model has several implications for prevention, diagnosis, and therapy of COVID-19.
Keywords:
antibodies
; COVID-19
; glycans
; immunoglobulin M
; SARS-CoV-2
; pneumonia
; prediction
; protection
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



