Submitted:
10 November 2025
Posted:
12 November 2025
You are already at the latest version
Abstract
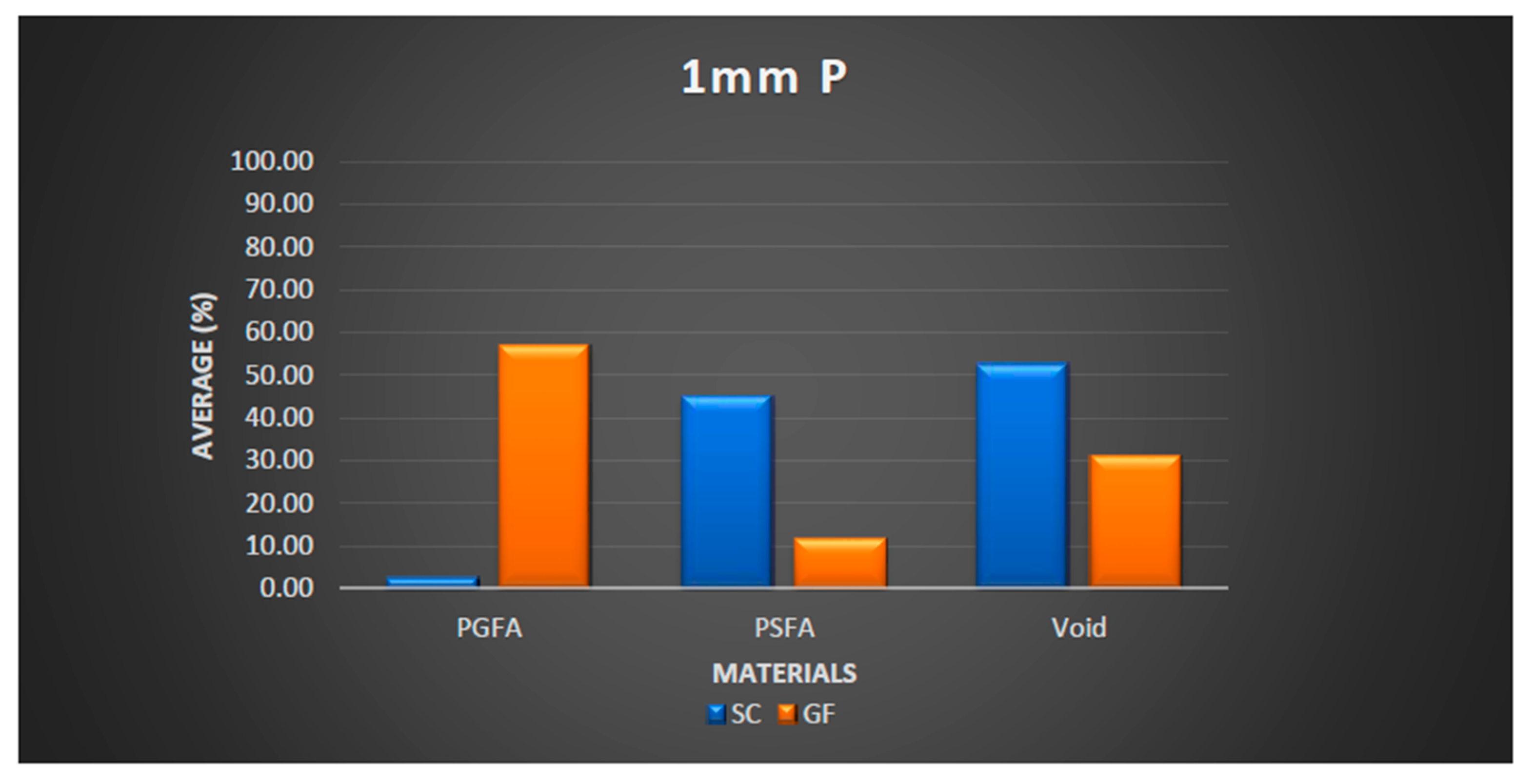
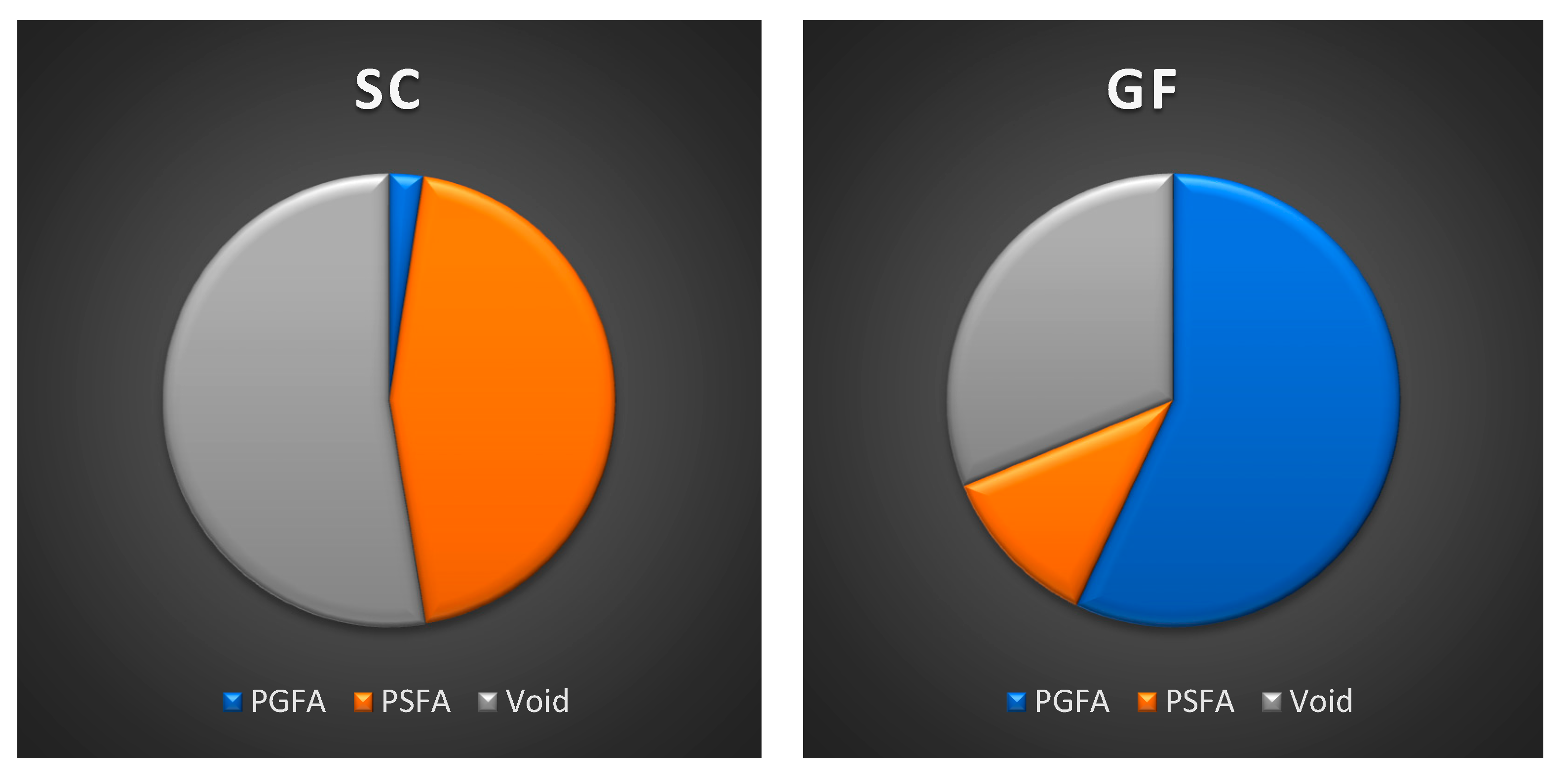
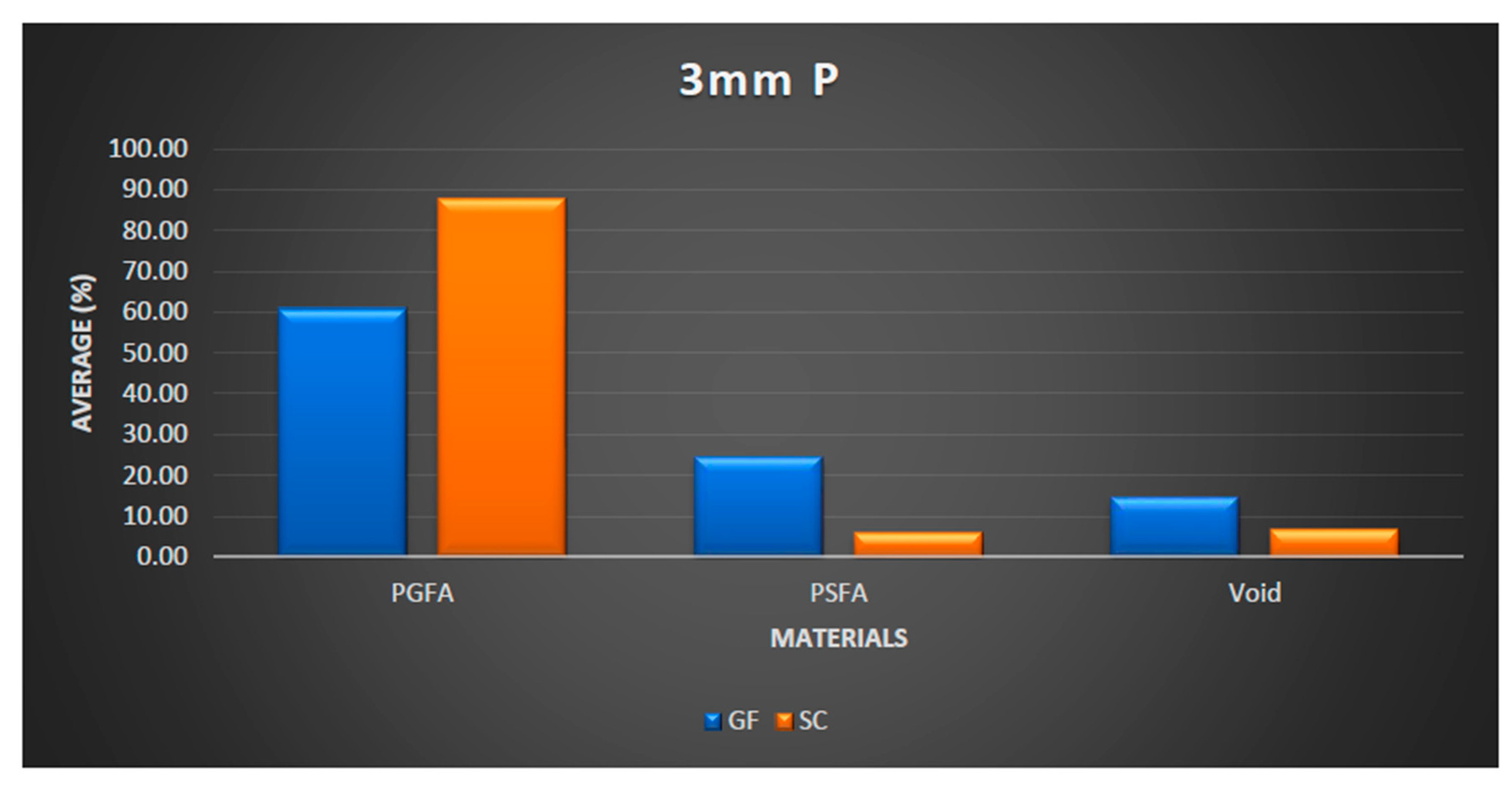
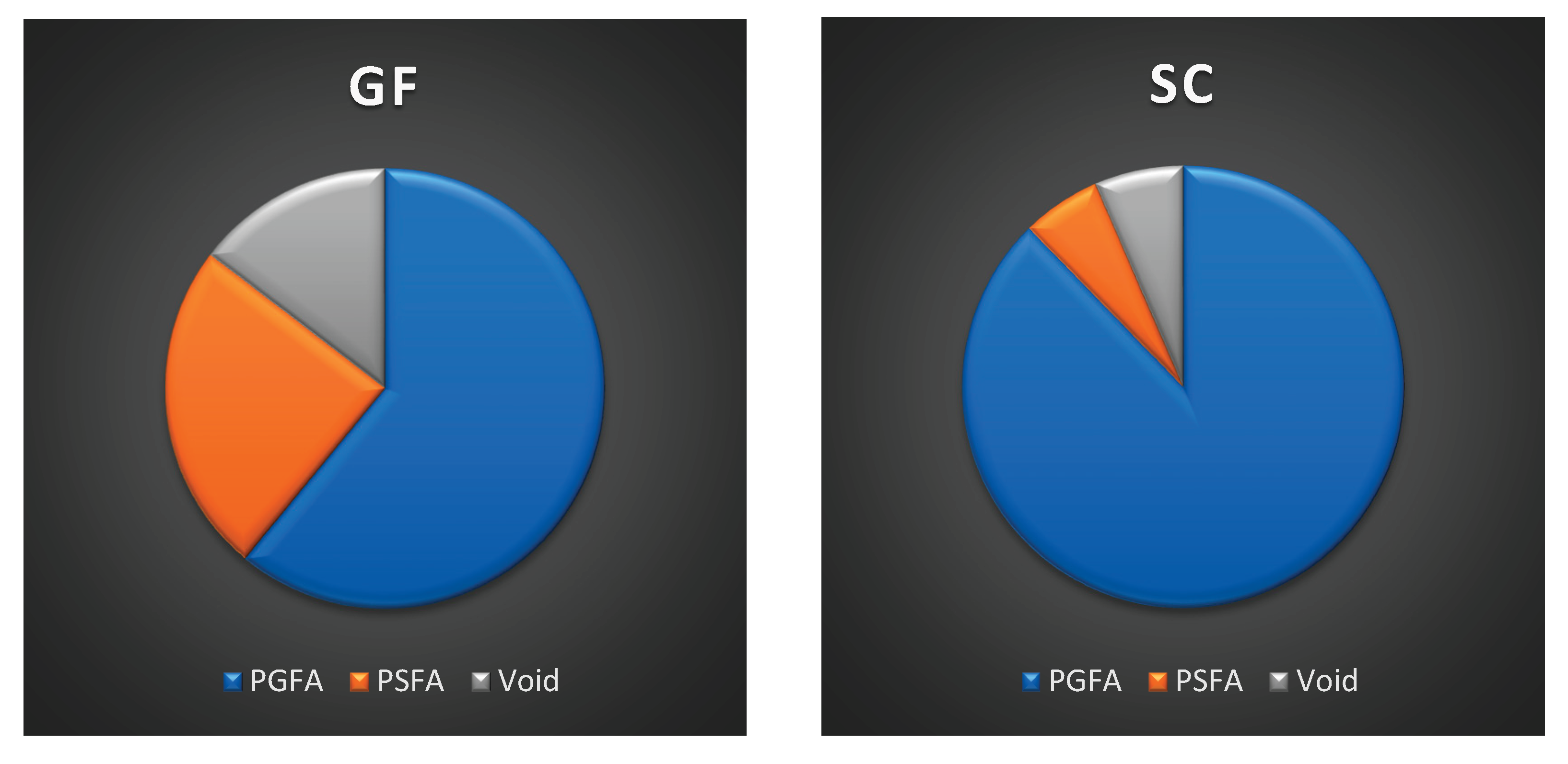
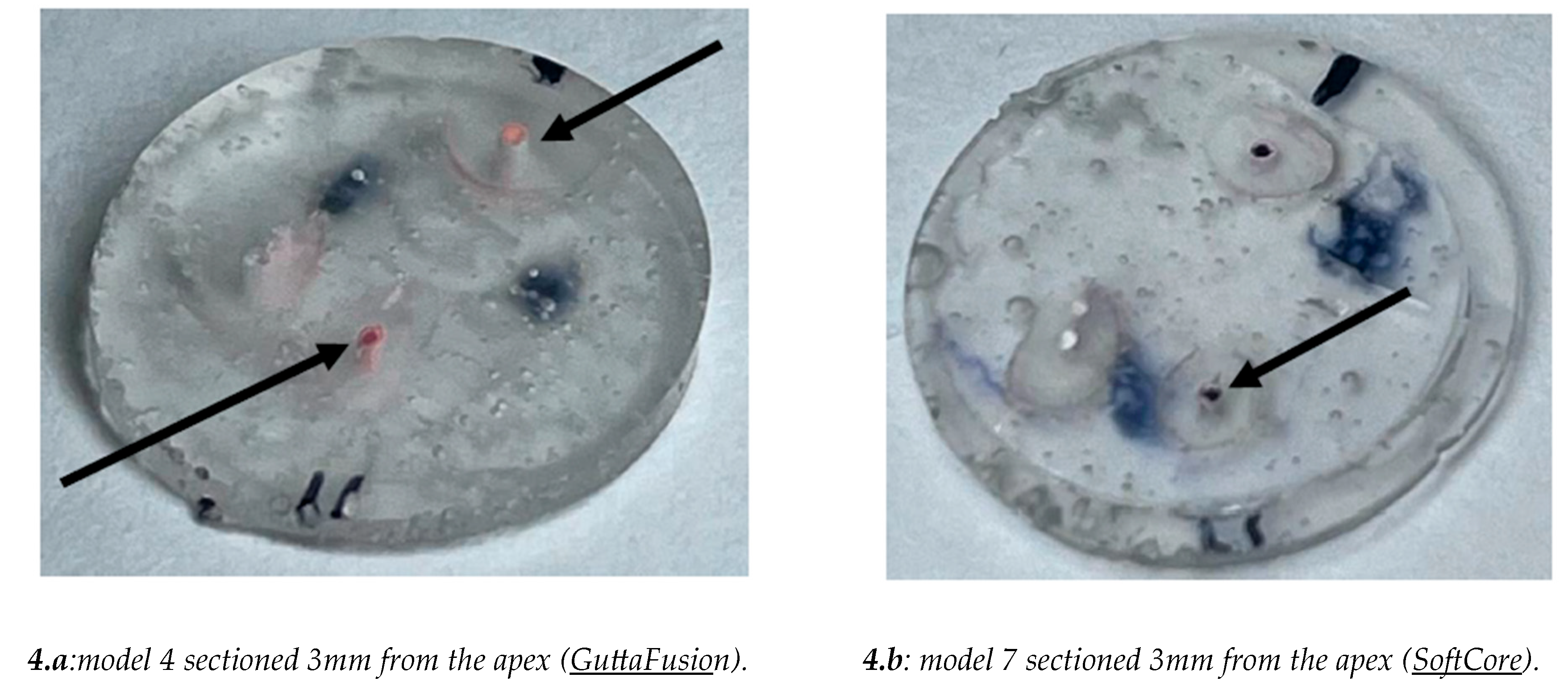
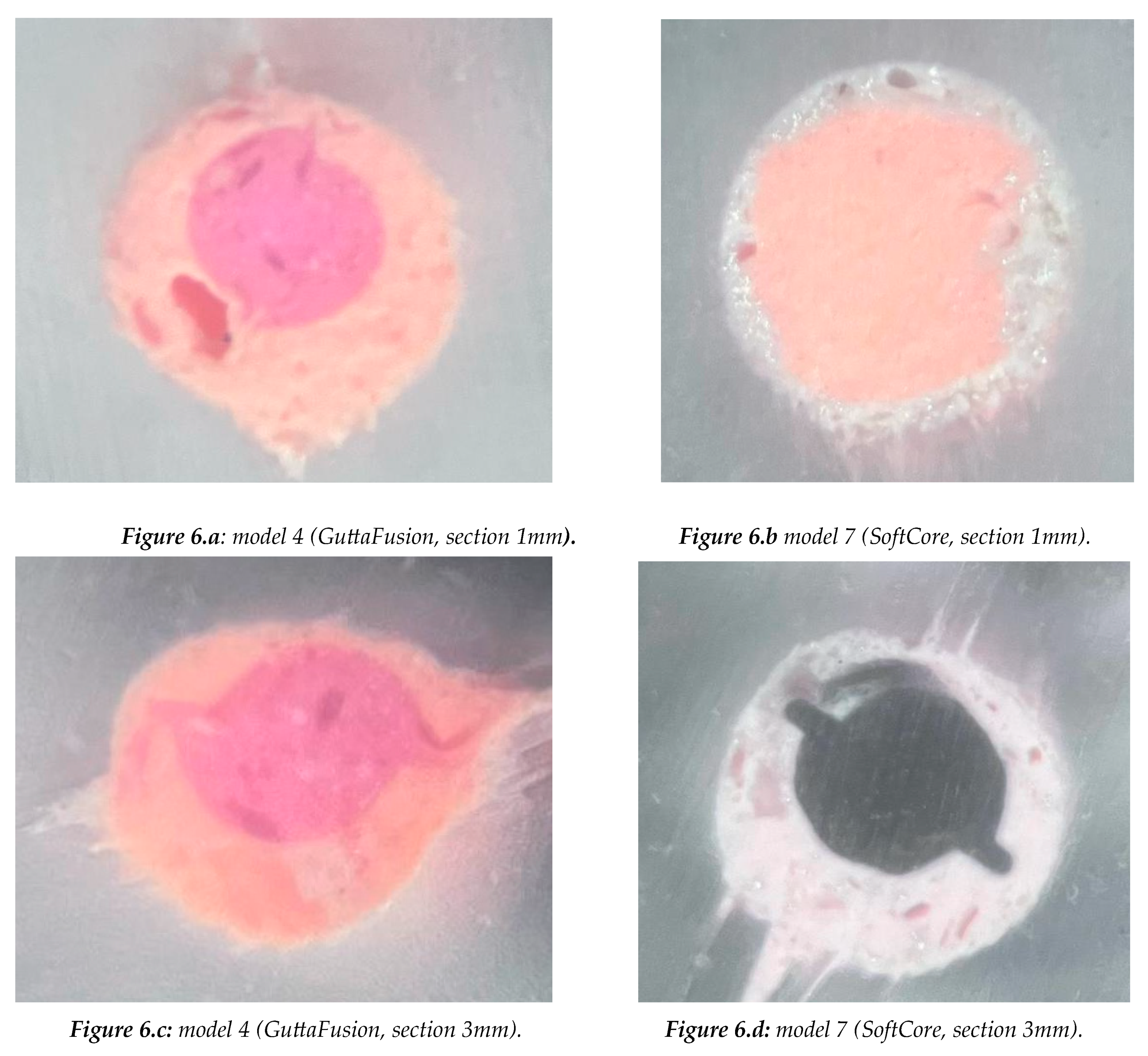
The aim of the study was to compare the sealing of two different core techniques (SoftCore and Guttafusion) associated to a bioceramic sealer (NeoSealer Flo). Eight tooth models (upper first molar) with simulated canals were used in this study. The models were divided into two groups: Group 1 (samples 1 to 4): Root canals were obturated with GuttaFusion. Group 2 (samples 5 to 8): Root canals were obturated with SoftCore. Both groups were filled with NeoSealer Flo sealer. Only the P and DV canals were obturated for each model. The models were sectioned at 1mm and 3mm from the apex. The total area of each canal segment was measured, and the areas were converted into the percentage of “Gutta-percha-filled areas”, ” Cement-filled areas”, “Void areas”. At 1mm from the apex GuttaFusion (GF) produced a higher PGFA and a lower PSFA value compared to SoftCore (SC). Additionally, SC produces a higher PGVA compared to GF. The values of PGFA, PSFA, and PVA are also comparable in the sections taken at 3mm from the apex. Comparing the two different techinques, a higher PGFA in GuttaFusion (GF) and a higher PSFA in SoftCore (SC) were found, while the VA was greater but comparable in both techniques, with a slight increase in percentage in the SC technique. At 3 mm, a higher PGFA was found compared to the PGFA at 1 mm.
Keywords:
1. Introduction
2. Materials and Methods
- GuttaFusion (samples 1 to 4)
- SoftCore (samples 5 to 8).
- Gutta-percha area
- Cement area
- Void area
2. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schilder, H. Filling root canals in three dimensions. J. Endod. 1967, 23, 732–740. [Google Scholar] [CrossRef]
- Tomson, R.M.; Polycarpou, N.; Tomson, P.I. Contemporary obturation of the root canal system. Br. Dent. J. 2014, 216, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Whithworth, J. Methods of filling root canals: principles and practice. Endod. Topics 2005, 12, 2–24. [Google Scholar] [CrossRef]
- Gallusi, G.; Campanella, V.; Montemurro, E.; Di Taranto, V.; Libonati, A. Antibacterial activity of first and latest generation bioceramic sealers on the elimination of Enterococcus faecalis: an in vitro study. J. Biol. Regul. Homeost. Agents 2020, 34 (3 Suppl. 1), 73–79. [Google Scholar]
- Ciani, L.; Libonati, A.; Dri, M.; Pomella, S.; Campanella, V.; Barillari, G. About a possible impact of endodontic infections by Fusobacterium nucleatum or Porphyromonas gingivalis on oral carcinogenesis: a literature overview. Int. J. Mol. Sci. 2024, 25, 5083. [Google Scholar] [CrossRef]
- Skinner, R.; Van Himel, T. The sealing ability of injection-molded thermoplasticized gutta-percha with and without the use of sealers. J. Endod. 1987, 13, 315–317. [Google Scholar] [CrossRef]
- Wu, M.K.; Ozok, A.R.; Wesselink, P.R. Sealer distribution in root canals obturated by three techniques. Int. Endod. J. 2000, 33, 340–345. [Google Scholar] [CrossRef]
- Kontakiotis, E.G.; Wu, M.K.; Wesselink, P.R. Effect of sealer thickness on long-term sealing ability: a two-year follow-up study. Int. Endod. J. 1997, 30, 307–312. [Google Scholar]
- Peters, D.D. Two-year in vivo solubility evaluation of four gutta-percha sealer obturation techniques. J. Endod. 1986, 12, 139–145. [Google Scholar] [CrossRef]
- Souza, E.M.; Wu, M.K.; Van Der Sluis, L.W. Effect of filling techniques and root canal area on the percentage of gutta-percha in laterally compacted root fillings. Int. Endod. J. 2009, 42, 719–726. [Google Scholar] [CrossRef]
- Jarrett IS, Marx D, Covey D, Karmazin M, Lavin M, Gound T. Percentage of canals filled in apical cross sections - an in vitro study of seven obturation techniques. Int Endod J. 2004 Jun;37(6):392-8.
- Johnson, W.B. A new gutta-percha technique. J. Endod. 1978, 4, 184–188. [Google Scholar] [CrossRef]
- Soft Core Manual. Soft Core Dental Production, Copenhagen, Denmark.
- Mark, J.E. Physical Properties of Polymers Handbook. Springer, 2007.
- Eguchi, D.E.; Peters, D.D.; Hollinger, J.O.; Lorton, L.A. Comparison of the area of the canal space occupied by gutta-percha following four gutta-percha obturation techniques using ProConsol sealer. J. Endod. 1985, 11, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Silver, G.K.; Love, R.M.; Purton, D.G. Comparison of two vertical condensation obturation techniques: Touch and Heat modified and System B. Int. Endod. J. 1999, 32, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Gencoglu, N.; Garip, Y.; Bas, M.; Samani, S. Comparison of different gutta-percha root filling techniques: Thermafil, Quick-Fill, System B, and lateral condensation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 333–336. [Google Scholar] [CrossRef] [PubMed]
- De Deus, G.; Gurgel-Filho, E.D.; Magalhães, K.M.; Coutinho-Filho, T. A laboratory analysis of gutta-percha-filled area obtained using Thermafil, System B and lateral condensation. Int. Endod. J. 2006, 39, 378–383. [Google Scholar] [CrossRef]
- Ishley, D.J.; ElDeeb, M.E. In vitro assessment of the quality of apical seal of thermomechanically obturated canals with and without sealer. J. Endod. 1986, 9, 242–246. [Google Scholar] [CrossRef]
- ElDeeb, M.E. The sealing ability of injection-molded thermoplasticized gutta-percha. J. Endod. 1985, 11, 84–86. [Google Scholar] [CrossRef]
- Natural GP Soft-Core: A 3rd Generation Endodontic Obturator Manual. Dental Production Aps, Copenhagen, 2001.
- Zamparini, F.; Prati, C.; Taddei, P.; Spinelli, A.; Di Foggia, M.; Gandolfi, M.G. Chemical-physical properties and bioactivity of new premixed calcium silicate–bioceramic root canal sealers. Int. J. Mol. Sci. 2022, 23, 13914. [Google Scholar] [CrossRef]
- Sanz, J.L.; López-García, S.; Rodríguez-Lozano, F.J.; Melo, M.; Lozano, A.; Llena, C.; Forner, L. Cytocompatibility and bioactive potential of AH Plus Bioceramic sealer: an in vitro study. Int. Endod. J. 2022, 55, 1066–1080. [Google Scholar] [CrossRef]
- Libonati, A.; Gallusi, G.; Angotti, V.; Di Taranto, V. The effect of different polishing systems on the surface roughness of two restorative dental materials. Oral Implantol. 2018, 11, 185–190. [Google Scholar]
- Gençoğlu, N. Comparison of six different gutta-percha techniques (Part II): Thermafil, JS Quick-Fill, Soft-Core, Microseal, System B and lateral condensation. [Journal not specified].
- Wu, M.K.; Van Der Sluis, L.W.; Wesselink, P.R. A preliminary study of the percentage of gutta-percha–filled areas in the apical canal filled with vertically compacted warm gutta-percha. Int. Endod. J. 2002, 35, 527–535. [Google Scholar] [CrossRef]
- Rubach, W.C.; Mitchell, D.F. Periodontal disease, accessory canals and pulp pathosis. J. Periodontol. 1965, 36, 34–38. [Google Scholar] [CrossRef] [PubMed]
- De Deus, Q.D. Frequency, location, and direction of lateral, secondary and accessory canals. J. Endod. 1975, 20, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Nica, L.M.; Didilescu, A.; Rusu, D.; et al. Photomicrographic evaluation of the apical sealing capacity of three types of gutta-percha master cones: an in vitro study. Odontology 2012, 100, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Libonati, A.; Montemurro, E.; Nardi, R.; Campanella, V. Percentage of gutta-percha–filled areas in canals obturated by three different techniques with and without the use of endodontic sealer. J. Endod. 2017, 1–4. [Google Scholar]



| SAMPLES | P ROOT CANAL |
DB ROOT CANAL |
MB2 ROOT CANAL |
MB1 ROOT CANAL |
| 1-8 | WL: 22.5mm Ref: MP cuspid Apex: K-file (30) |
WL: 20.5 mm Ref: DV cuspid Apex: K-file (30) |
WL: 22 mm Ref: MP cuspid Apex: K-file (30) |
WL: 22 mm Ref: MV cuspid Apex: K-file (30) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



