Submitted:
22 July 2025
Posted:
22 July 2025
You are already at the latest version
Abstract
This study elaborates on amyotrophic lateral sclerosis (ALS) Cardiomyopathy from multiple dimensions. In the onset of ALS, from a genetic perspective, numerous disease-causing and related genetic variations have been identified, and there are also differences in genetic lineages across different regions. Genetic factors may have an impact on cardiac health. For instance, patients with certain mutations have an increased risk of developing cardiac complications, and the polymorphism of the TDP-43 gene is also related to cardiac susceptibility. In ALS cases with TDP-43 onset, factors directly associated with ALS cardiomyopathy can be identified, such as excessive phosphorylation and inflammatory factors.
In traditional Chinese medicine (TCM), ALS Cardiomyopathy is classified as "flaccidity syndrome",especially for the syndrome of heart deficiency.According to traditional Chinese medicine theory, the five elements interact in a cycle of generation and restriction. The occurrence of heart deficiency is related to the functions of the spleen, kidney and liver.
An innovative integrated Chinese-Western medicine model explores gene-syndrome associated diagnosis and treatment, and AI technology aids in identifying potential drug targets, demonstrating new therapeutic potential. This paper comprehensively presents the basic research, TCM theories, and therapeutic explorations related to ALS and its cardiac involvement.
Keywords:
ALS cardiomyopathy
; genetics
; TDP-43
; TCM treatment
Introduction:
ALS---Amyotrophic lateral sclerosis (ALS), commonly known as Lou Gehrig's disease, is a chronic progressive neurodegenerative disease. The pathogenesis of hereditary ALS is complex.[1]. ALS patients have a short survival period. Currently, there are no effective drugs available, and the side effects of the drugs are severe while the prices are high. [2].
The causes of ALS are mostly related to genes, such as SOD1, etc. Among them, TDP-43 is the factor most closely associated with ALS cardiomyopathy.
In traditional Chinese medicine theory, ALS is classified as a type of "wei bi" syndrome, which is closely related to genetic factors and dysfunction of the spleen and kidney systems. According to the principles of the interrelationships among the five elements—specifically their cycles of generation and restraint—when the disease affects the heart muscle, leading to symptoms such as cardiac weakness, chest tightness, and shortness of breath, it is categorized under the syndromes of "heart wei" or "heart bi." This reflects a complex pathological mechanism involving the interaction of "weibi," "bi," and "heart" syndromes.
Result
Genetic Basis: Molecular Genetic Framework of Cardiac Involvement in ALS
To date, over 50 pathogenic genes for ALS and more than 100 related gene variants (which increase disease susceptibility or influence clinical phenotypes) have been reported [17]. Statistics indicate that approximately 20% of hereditary ALS cases are caused by SOD1 gene mutations [3]. Hexanucleotide (G4C2) repeat expansions in the non-coding region of the C9orf72 gene are the most common pathogenic factor in familial ALS (fALS) patients in Europe. Patients carrying these mutations have a relatively higher risk of cardiac complications. Approximately half of familial ALS patients harbor this pathogenic G4C2 repeat expansion, which also occurs in 5%-10% of sporadic cases [12]. Carriers of C9orf72 variants typically have an earlier onset and milder manifestations; they often present with cognitive impairment or behavioral deficits, predominantly bulbar onset, a family history, and poor prognosis [16]. Due to differences in genetic backgrounds, the spectrum of ALS pathogenic genes varies across regions. In Europe, the most common pathogenic gene is C9orf72, followed by SOD1, TARDBP, and FUS [18], whereas C9orf72 variants are less frequent in Asian patients, particularly in Chinese populations [19]. Other genes associated with rapid disease progression include CAMTA1961, CX3CRI⁹⁷¹, COL19A1⁹⁸, ZNF512B⁹⁹, SOD1 A4V [13], and FUS P525L [14]. In China, the C9 genotype is rare, accounting for only ~0.3% of sporadic cases [15]. In Asia, the most common pathogenic gene is SOD1, followed by FUS, C9orf72, and TARDBP [18]; in China, SOD1 also has the highest mutation rate, accounting for ~25.60% of familial ALS and 1.60% of sporadic ALS [19].
For sporadic ALS (sALS), despite its more complex pathogenesis, genetic factors are non-negligible. Studies have found that variations in the 9p21 chromosomal region are associated with myocardial fibrosis, suggesting that genetic susceptibility loci in sALS may impact cardiac health [4].
To explore the relationship between ALS and myocardial fibrosis, we included a study on cardiomyopathy. Cardiomyopathy is a type of disease characterized by abnormal structure and function of the heart muscle, typically manifested as heart hypertrophy, dilation, or fibrosis, ultimately leading to heart failure, arrhythmia, and even sudden death. Based on the cause, cardiomyopathy can be classified as hereditary and acquired. In recent years, it has been discovered that certain neurodegenerative diseases (such as ALS) especially sALS may also be accompanied by myocardial damage.
In patients with amyotrophic lateral sclerosis (ALS), in addition to the typical degeneration of motor neurons, some cases also show cardiac dysfunction, such as arrhythmia, decreased myocardial contractility, and even heart failure. This phenomenon may be related to the abnormal aggregation of the TDP-43 protein pathology (the key pathological marker of ALS) in myocardial cells (Figure 1). TDP-43 not only affects the RNA metabolism and mitochondrial function of neurons, but may also damage the energy supply and contractile ability of myocardial cells through similar mechanisms[44], thereby inducing "ALS cardiomyopathy".
Regarding the TDP-43 gene (TARDBP), its polymorphisms play a key role in cardiac susceptibility. From the perspective of TDP-43’s genetic regulation and cardiac expression, transcriptional regulation of the TARDBP gene is complex; methylation of the SP1 binding site in the promoter region can affect TDP-43 expression levels in cardiomyocytes [5]. A typical pathological feature in ALS patients is the mislocalization of TDP-43 from the nucleus to the cytoplasm, where it forms ubiquitinated aggregates [30]. These aggregates are a hallmark of ALS and are present in most cases, regardless of genetic mutations [31]. The exact mechanisms underlying TDP-43 mislocalization and aggregation remain under investigation. However, recent studies indicate that post-translational modifications—such as phosphorylation, ubiquitination, and cleavage—play important roles. For example, hyperphosphorylation of TDP-43 at specific serine residues (e.g., S409/S410) promotes its cytoplasmic localization and aggregation [32].
Additionally, mutations in the TARDBP gene (which encodes TDP-43) can cause abnormal protein folding and aggregation. The A315T mutation—one of the most studied TARDBP mutations in ALS—disrupts TDP-43’s normal interactions with RNA and other proteins, leading to increased aggregation and toxicity [33]. TDP-43’s role in regulating cardiac gene expression is disrupted in ALS. In cardiomyocytes, mislocalized and aggregated TDP-43 fails to perform its normal transcriptional and post-transcriptional regulatory functions, leading to dysregulated expression of genes critical for cardiac function. For instance, genes encoding proteins involved in cardiac contraction (e.g., troponin and myosin heavy chain) have been shown to be abnormally expressed in cardiomyocytes with TDP-43 abnormalities [34]. A recent transcriptomic analysis of cardiac tissue from ALS patients with cardiomyopathy revealed significantly downregulated expression of genes related to calcium handling—essential for normal myocardial contraction and relaxation [35]. Such gene dysregulation can ultimately impair cardiac contractility and contribute to cardiomyopathy development. The presence of abnormal TDP-43 in cardiac tissue triggers an inflammatory response. In the hearts of ALS patients with cardiomyopathy, levels of proinflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) are elevated [36]. TDP-43 aggregates can activate innate immune pathways in cardiomyocytes and cardiac macrophages. For example, the NLRP3 inflammasome—a key component of the innate immune system—has been shown to be activated by TDP-43 aggregates in cardiac cells [37]. The resulting chronic inflammation further damages cardiac tissue, impairs normal cardiac function, and promotes cardiomyopathy progression.
TCM Theories on Hereditary Cardiomyopathy in ALS
Based on clinical symptoms, ALS is classified under "flaccidity syndrome" in TCM. Early manifestations include local muscle weakness or atrophy, with rapid progression from onset to death. The London staging system—a simple and practical method for ALS staging [6]—divides the disease course into 5 stages based on patients’ milestone clinical symptoms [7]. Its criteria reflect the expansion of ALS lesions, which correlates with the evolution of disease location and progression in TCM. Studies have shown that spleen-kidney deficiency is the primary syndrome, present throughout ALS pathogenesis [8]; liver-kidney deficiency is more common in stages 2-4, while insufficient pectoral qi is typical in stage 4b or 5 [9].
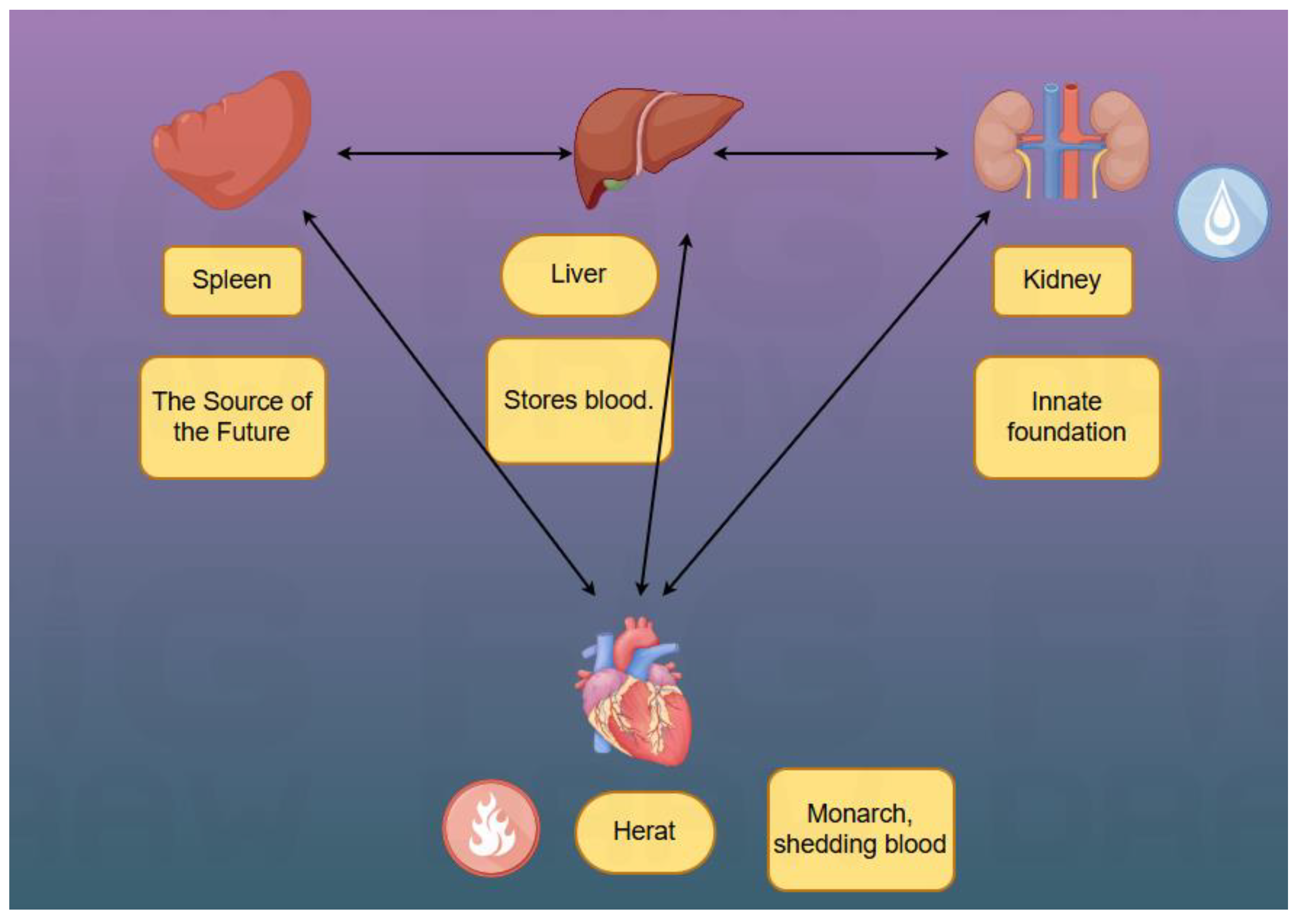
In TCM theory, the kidney is the "congenital foundation," and the spleen is the "acquired foundation." The "hereditary" nature of the disease is attributed to "congenital endowment deficiency"—i.e., deficient parental essence or inadequate fetal nourishment leads to insufficient congenital kidney essence and weak visceral function in offspring, forming the internal basis for disease onset. Su Wen · Jing Mai Bie Lun (Canon of Medicine: Treatise on Divergent Meridians) states: "Food qi enters the stomach; turbid qi returns to the heart, and nutrient essence flows into the vessels" and "the spleen governs transportation and transformation"—responsible for converting cereal essence into qi and blood, serving as the source of qi and blood production. "The heart governs the blood vessels" and relies on sufficient qi and blood for normal circulation and mental activity. If spleen deficiency impairs transportation, qi and blood production decreases, depriving the heart vessels of nourishment, potentially causing heart qi or blood deficiency, manifested as palpitations. Symptoms such as "palpitations", "chest obstruction", "breathing disorders" and "edema" are precisely the typical manifestations of cardiomyopathy in traditional Chinese medicine. Pi Wei Lun (Treatise on the Spleen and Stomach) notes: "Spleen-stomach deficiency leads to obstruction of the nine orifices and inability to move the limbs." The spleen governs muscles; spleen deficiency can indirectly cause poor circulation in heart vessels (Figure 2).
The kidney belongs to "water" and the heart to "fire"—"heart-kidney interaction maintains balance between water and fire." Additionally, the kidney stores essence, which can transform into blood ("essence and blood share the same origin"). Deficient kidney essence reduces essence and blood production, depriving the heart of nourishment, leading to heart blood deficiency—manifested as palpitations, dizziness, and amnesia.
"The liver stores blood, and the heart circulates blood"; "the liver governs dispersion and regulates mental activity." Liver deficiency can affect the heart. Lin Zheng Zhi Nan Yi An (Guide to Clinical Practice) proposes: "The liver and kidney share the same origin and should be treated together," emphasizing the importance of regulating both. Liver-kidney yin deficiency generates internal deficient fire, burning blood vessels and causing heart blood stasis—manifested as palpitations, chest pain, and dark red tongue. Concurrent liver-kidney deficiency leads to disordered liver dispersion and impaired kidney qi reception, disrupting qi movement and further impairing the heart’s vessel-governing function—manifested as chest tightness, shortness of breath, and palpitations. The Jueyin Liver Meridian "runs behind the throat and enters the pharynx," so liver-kidney impairment may also cause speech difficulties and dysphagia. Key manifestations of liver-kidney deficiency syndrome include marked muscle disuse/atrophy, fasciculations, flaccid tendons, insomnia with dreams, emotional depression, red tongue with scanty coating, and thready rapid pulse [10].
Su Wen · Wei Lun (Canon of Medicine: Treatise on Flaccidity) mentions "flaccid feet" and "tendon flaccidity," emphasizing their association with "deficiency of the five zang-organs." Cardiomyopathy falls under "palpitations" and "chest impediment" in TCM, with "disharmony of heart vessels" as the core. Despite different disease locations, "congenital endowment deficiency" causes "kidney-spleen-liver-heart" dysfunction, forming a complex syndrome of "deficiency (of essence, qi, blood, yin, yang) + stasis (qi stagnation and blood stasis)"—deficiency as the root and stasis as the branch—ultimately manifesting as concurrent "flaccidity syndrome" and "palpitations," consistent with the multi-system damage in "ALS hereditary cardiomyopathy."
A study on 77 ALS patients using EMG and TCM syndrome analysis found widespread neurogenic damage in all patients: 41 cases in the medullary segment, 77 in the cervical segment, 29 in the thoracic segment, and 64 in the lumbosacral segment. Sensory and nerve conduction velocities were roughly normal, with reduced compound muscle action potential amplitude as a common finding. Stratified by involved segments, syndromes were predominantly liver-kidney deficiency, spleen-stomach weakness, and collateral stasis. Among patients with thoracic segment neurogenic damage, liver-kidney deficiency (48.3%) and collateral stasis (27.6%) were primary; among those without, spleen-stomach weakness (39.6%) and liver-kidney deficiency (31.3%) predominated [11].
Exploring Treatments for ALS Cardiomyopathy: Integrated Chinese-Western Medicine Strategies
Heart failure, as a major cause of death in cardiomyopathy, is usually the focus of treatment and prevention for heart-related diseases. The drug treatment for symptoms of heart failure mainly falls into the following two aspects: To improve and alleviate symptoms such as palpitations and chest tightness, clinical treatment usually employs diuretics (such as furosemide, spironolactone, etc.) and vasodilators (such as nitroglycerin) to alleviate symptoms and hemodynamics by reducing the cardiac volume load and preload [45]. Oxidative stress can activate multiple signaling pathways and lead to organ fibrosis. Therefore, a class of antioxidants with anti-oxidative stress effects (such as N-acetylcysteine) is also often used as a potential drug. Animal experiments on hypertrophic cardiomyopathy have shown that N-acetylcysteine has the effect of reversing myocardial hypertrophy, myocardial fibrosis, and disordered cell arrangement, and preventing heart failure [46]. The cornerstone drugs for improving the long-term prognosis of heart failure symptoms include renin-angiotensin system inhibitors, beta-blockers, and new SGLT2 inhibitors. When ALS patients have a rapid progression of the disease and develop life-threatening symptoms related to heart failure, these drugs may offer a glimmer of hope for the patients.
However, long-term use of diuretics may lead to electrolyte imbalance. Therefore, traditional Chinese medicine's syndrome differentiation and adjustment therapy holds significant importance for patients with stable-stage cardiomyopathy[47]. In traditional Chinese medicine theory, the pathogenesis of cardiomyopathy is complex and involves both deficiency and excess. During clinical diagnosis and treatment, different treatments are given based on the different diagnostic conditions. The "Discourse on Regulating the Meridians" in "The Inner Classic" states: "When qi and blood are out of balance, various diseases will arise." The blood stasis caused by the depletion of heart qi is one of the main causes of cardiomyopathy. The "Difficult Classic" mentions: "Qi is the foundation of the human body." When qi is deficient, it is unable to carry blood, and blood stasis subsequently occurs; at the same time, the functions of qi and blood in protecting the human body are lost, and vitality is difficult to maintain. Therefore, from a traditional Chinese medicine perspective, the treatment of cardiomyopathy mainly focuses on nourishing qi and yin, promoting blood circulation, and relaxing meridians[48].
In exploring treatments for ALS-related cardiac lesions, Western medicine and TCM-guided interventions exhibit distinct characteristics and synergistic potential. Current ALS treatments include medication [39], targeted therapy, gene therapy, TCM herbal therapy, and acupuncture [38]. FDA-approved drugs for ALS include riluzole, edaravone, dextromethorphan hydrobromide, and quinidine sulfate, which delay disease progression and extend survival. However, these drugs often have side effects and are costly [20]. Western gene therapy focuses on key pathogenic mechanisms; gene silencing in such strategies inhibits harmful gene expression using antisense oligonucleotides (ASOs) or RNA interference [21]. The first ASO approved for ALS marks a new era in treatment [22]. ASO-based gene therapies for ALS target 3 specific gene mutations (SOD1, C9orf72, FUS) and 1 potential modifier of TDP-43 (ATXN2) [23].
There is a new development: a combined cellular-gene therapy for ALS has been adopted.NurOwn is the first cell therapy for ALS. It uses adult stem cells from the patient's own bone marrow, which are expanded and subjected to exogenous intervention. These cells can secrete various neurotrophic factors (NTFs) in vitro. Then, they are injected intrathecally back into the patient's body to exert neuroprotective effects. It can also stimulate the growth of motor neurons and promote the re-distribution of nerve-muscle junction nerves. [42] In a phase III clinical trial involving 196 patients, the safety and efficacy of repeated use of NurOwn in ALS patients were evaluated. The results showed that neither the primary nor the secondary endpoints reached statistical significance. However, in the cerebrospinal fluid of patients who received this treatment, there were significant improvements in markers related to neuroinflammation, neurodegeneration, and neuroprotection, and the levels of NTFs also increased. Moreover, the treatment was well tolerated [43].
In TCM treatment of ALS, most herbs are warm, neutral, or slightly warm in nature, with sweet, bitter, and pungent flavors predominating. Su Wen · Xuan Ming Wu Qi (Canon of Medicine: Manifestations of the Five Qi) states: "Sour enters the liver, pungent enters the lung, bitter enters the heart, salty enters the kidney, sweet enters the spleen." These three flavors primarily act on the heart, spleen, and lung: sweet tonifies, harmonizes, and relieves; bitter purges and dries; pungent disperses and promotes circulation. Thus, ancient formulas for flaccidity syndrome focus on tonifying deficiency, clearing heat, promoting qi, and activating blood. In terms of meridian tropism, they mainly act on the liver, spleen, and kidney meridians: the liver governs tendons (liver heat causes tendon spasm; deficient nourishment leads to flaccidity); the Taiyin Spleen Meridian, rich in qi and blood, nourishes muscles/limbs (spleen deficiency reduces qi/blood, causing muscle atrophy); the kidney, the congenital foundation, governs bones and generates marrow (kidney deficiency leads to bone withering and marrow depletion, causing bone flaccidity). Ancient TCM formulas for flaccidity syndrome primarily use warm/neutral tonics, supplemented by cold herbs to eliminate pathogens, focusing on tonifying the liver, spleen, and kidney, clearing lung heat, and dispelling wind, cold, and dampness [24]. Representative formulas include Si Junzi Decoction [26], Buzhong Yiqi Decoction [25], and Dihuang Yinzi (Rehmannia Decoction) [27], which have shown clinical efficacy. In exploring the association between ALS and cardiac lesions, clinical manifestations of cardiac dysfunction and related assessment methods are critical. Diastolic dysfunction—an early detectable cardiac functional change—exhibits unique characteristics in ALS patients. The innovative integrated Chinese-Western medicine model aims to integrate Western precision gene therapy with TCM syndrome differentiation. By establishing a "gene-syndrome associated diagnosis and treatment" framework, it correlates mutations (e.g., TARDBP) with TCM syndromes. For example, patients with abnormal TDP-43 deposition due to specific gene mutations, presenting with "phlegm-stasis intertwinement," may receive gene editing or ASO therapy combined with phlegm-resolving and stasis-dispersing herbal formulas or monomers, achieving multi-level intervention from gene to systemic regulation, and providing more comprehensive, personalized solutions for ALS-related cardiac lesions. Additionally, with technological advancements, AI has entered ALS treatment. Researchers such as Pun FW utilized PandaOmics—a cloud-based platform integrating deep learning and AI—to analyze transcriptomic and proteomic data from central nervous system samples in public datasets, as well as direct iPSC-derived motor neurons (diMNs) from the Answer ALS project, identifying potential drug targets and predicting druggability [29]. The study identified 17 high-confidence therapeutic targets for ALS, including ADRA2B, CYBB, and FLT1. Furthermore, in a c9ALS Drosophila model, 8 previously unreported genes (KCNB2, KCNS3, ADRA2B, NR3C1, P2RY14, PPP3CB, PTPRC, RARA) were validated; their inhibition significantly alleviated neurodegeneration, demonstrating AI’s potential to accelerate the discovery of new therapeutic targets [28]. Conclusion
The genetic aspects of ALS cardiomyopathy have received relatively less research at present. The cause of cardiomyopathy due to genetic inheritance or mutation of the ALS gene still requires further exploration.ALS cardiomyopathy is closely related to TDP-43, and the underlying mechanism still needs to be explored..
TCM, starting from "flaccidity syndrome," has established a theoretical system based on visceral interactions.Among them, deficiency of yang in the spleen and kidney, deficiency of yin in the liver and kidney, and insufficiency of qi are the causes leading to ALS cardiomyopathy. All of these can lead to a deficiency of heart qi, resulting in chest tightness, palpitations and heart palpitations. And the yang energy gradually accumulates, eventually leading to a deficiency of yang in the heart, resulting in symptoms such as feeling cold and palpitations. The progression of ALS cardiomyopathy can lead to heart failure. Clinical studies have confirmed correlations between syndrome distribution and neurogenic damage segments, providing a basis for syndrome differentiation.
In treatment, Western medicine has advanced in drugs, supportive care, and gene therapy but faces challenges like side effects and high costs. The integrated Chinese-Western medicine model, by correlating genes with syndromes, holds promise for personalized, multi-level intervention. AI technology accelerates target discovery, opening new avenues for drug development. Future research should deepen genetic mechanism studies, optimize integrated treatment protocols, and advance AI applications to improve ALS diagnosis/treatment, enhance prognosis, overcome current bottlenecks, and provide more effective strategies for managing ALS and its complex manifestations like cardiac involvement.
Funding
1.2023 Research and Cultivation Fund of Capital Medical University—Study on the correlation between intestinal flora and neurofilament light chain in mice with amyotrophic lateral sclerosis induced by acupuncture (PYZ23032). 2.R&D Program of Beijing Municipal Education Commission 2024: Study on the improvement of clinical symptoms and mechanism of acupuncture in amyotrophic lateral sclerosis (KM202410025018). 3.This study was supported by the China National Natural Science Foundation of youth project (No. 82405557). 4.This study was supported by 2024-2026 Chinese Association of Chinese Medicine young Talent lifting project (2024-QNRC2-B08).
References
- Meyer, T. Amyotrophe Lateralsklerose (ALS) – Diagnose, Verlauf und neue Behandlungsoptionen [Amyotrophic lateral sclerosis (ALS) - diagnosis, course of disease and treatment options].Dtsch Med Wochenschr. 2021;146(24-25):1613-1618.
- Wijesekera LC, Leigh PN. Amyotrophic lateral sclerosis.Orphanet J Rare Dis. 2009;4(1):3.
- Meijboom KE, Brown RH. Approaches to Gene Modulation Therapy for ALS. Neurotherapeutics. 2022;19(4):1159-1179.
- Meijboom KE, Brown RH. Approaches to Gene Modulation Therapy for ALS. Neurotherapeutics. 2022;19(4):1159-1179.
- Gendron T F, Rademakers R, Petrucelli L.TARDBP mutation analysis in TDP-43 proteinopathies and deciphering the toxicity of mutant TDP-43[J].Journal of Alzheimer's disease: JAD, 2013, 33(Suppl 1).
- BALENDRA R, AL KHLEIFAT A, FANG, T,; et al. A standard operating procedure for King's ALS clinical staging[J]. Amyotroph Lateral Scler Frontotemporal Degener, 2019,20(3-4):159-164.
- ROCHE J C, ROJAS-GARCIA R, SCOTT K, M,; et al. A proposed staging system for amyotrophic lateral sclerosis[J]. Brain,2012, 135(Pt 3):847-852.
- WANG M Z, GONG F, ZHANG J, S,; et al. Study on TCM syndrome characteristics of amyotrophic lateral sclerosis patients with different clinical types and stages[J]. Academic Journal of Shanghai University of Traditional Chinese Medicine,2022,36 (2):9-12.
- SONG Y B, RUI Y F, HAN Y, et al. Correlation between disease locations of traditional Chinese medicine and King's staging in 240 cases of amyotrophic lateral sclerosis [J]. World Chinese Medicine,2020,15(19):2988-2994.
- Shan Yuetong, Wu Feifei, Liang Xingwang, et al. Staged Differentiation and Treatment of Amyotrophic Lateral Sclerosis Based on Zangfu Theory [J]. Journal of Shanghai University of Traditional Chinese Medicine, 2025, 39(02): 63-67.
- Zhang Ren, Gao Tian, Han Lizhen, et al. Research on the Relationship between Electrophysiology, Pathology of Amyotrophic Lateral Sclerosis and TCM Syndrome Types [J]. Journal of Clinical Chinese Medicine, 2025, 37(04): 745-751.
- VAN DYKE J M, SMIT - OISTAD I M, MACRANDER C, et al. Macrophage - mediated inflammation and glial response in the skeletal muscle of a rat model of familial amyotrophic lateral sclerosis (ALS)[J]. Exp Neurol, 2016, 277:275 - 282.
- CHIOA,LOGROSCINOG,HARDIMANO,et al.Prognostic factors in ALS:A criticalreview[J/OL].Amyotrophic Lateral Sclerosis:Official Publication of the World Federationof Neurology Research Group on Motor Neuron Diseases,2009,10(5-6):310-323.
- LEBLOND CS,WEBBER A,GAN-OR Z,et al.De novo FUS P525L mutation inJuvenile amyotrophic lateral sclerosis with dysphonia and diplopia[J/OL].NeurologyGenetics, 2016, 2(2)[2023-03-25].
- HE J,TANG L,BENYAMIN B,et al.C9orf72 hexanucleotide repeat expansions inChinese sporadic amyotrophic lateral sclerosis[J/OL].Neurobiology of Aging,2015,36(9):2660.e1-8.
- BYRNES,ELAMINM,BEDEP,et al.Cognitive and clinical characteristics of patientswith amyotrophic lateral sclerosis carrying a C9orf72 repeat expansion:a population-basedcohort study[J/OL].The Lancet Neurology.2012,11(3):232-240.
- Yousefian - Jazi A, Seol Y, Kim J, Ryu HL, Lee J, Ryu H. Pathogenic genome signatures that damage motor neurons in amyotrophic lateral sclerosis[J]. Cells, 2020, 9:2687.
- Mejzini R, Flynn LL, Pitout IL, Fletcher S, Wilton SD, Akkari PA. ALS genetics, mechanisms, and therapeutics: where are we now[J].Front Neurosci, 2019, 13:1310.
- Wei Q, Chen X, Chen Y, Ou R, Cao B, Hou Y, Zhang L, Shang HF. Unique characteristics of the genetics epidemiology of amyotrophic lateral sclerosis in China [J]. Sci China Life Sci, 2019, 62:517 - 525.
- Gupta D, Vagha S, Dhingra H, Shirsath H. Advances in Understanding and Treating Amyotrophic Lateral Sclerosis (ALS): A Comprehensive Review. Cureus. 2023;15(11):e48691.
- TANG R, XU Z. Gene therapy: a double - edged sword with great powers [J]. Mol Cell Biochem, 2020, 474 (1/2): 73 - 81.
- VAN DA ELE S H, MASRORI P, VAN DAMME P, et al. The sense of antisense therapies in ALS[J]. Trends Mol Med, 2024,30(3):252-262.
- Wang Jie, Du Ailian. Advances in Diagnosis and Treatment of Amyotrophic Lateral Sclerosis [J]. Practical Geriatrics, 2025, 39(02): 127-133.
- Cao Tianyu. Research on the Prescription Medication Characteristics of Paralysis Syndromes and the Relationship between Traditional Chinese Medicine Syndromes and Prognosis of Amyotrophic Lateral Sclerosis [D]. Beijing University of Chinese Medicine, 2023.
- Li Kun, Liu Lin, Cai Shuling, et al. Mechanism of Buzhong Yiqi Decoction in the treatment of amyotrophic lateral sclerosis based on network pharmacology[J]. Henan Journal of Traditional Chinese Medicine, 2025, 45(07):1064-1072.
- Huang Yichen. Clinical Research on Modified Four Gentlemen Decoction Combined with Acupuncture in the Treatment of Amyotrophic Lateral Sclerosis [D]. Shanghai University of Traditional Chinese Medicine, 2021.
- He Pengfei. Research on the Medication Patterns and Drug Mechanisms of Ancient Paralysis Syndromes and Modern Amyotrophic Lateral Sclerosis [D]. Beijing University of Chinese Medicine, 2021.
- Gu Sichun, Qin Ruoyun, Ye Qing. Application of Artificial Intelligence in the Research of Amyotrophic Lateral Sclerosis: A Comprehensive Review [C]// Guangxi TCM Society, Shanghai Immunology Society, Ningxia TCM Society, Shaanxi Society of Integrated Traditional Chinese and Western Medicine. The 7th Shanghai and Western Regions Integrated Traditional Chinese and Western Medicine Brain Disease Forum Proceedings. Shanghai University of TCM Affiliated Longhua Hospital; 2024: 91-98.
- Pun FW, Liu BHM, Long X, Leung HW, Leung GHD, Mewborne QT, et al. Identification of Therapeutic Targets for Amyotrophic Lateral Sclerosis Using PandaOmics - An AI-Enabled Biological Target Discovery Platform. Front Aging Neurosci. 2022 Jun 28;14:914017.
- Neumann M, Sampathu DM, Kwong LK, et al. Ubiquitinated TDP - 43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Science. 2006;314 (5796):130 - 133.
- Mackenzie IR, Neumann M, Bigio EH, et al. Nomenclature and nosology for neuropathologic subtypes of frontotemporal lobar degeneration: an update. Acta Neuropathol. 2010;119 (1):1 - 4.
- Guo J, Li Y, Zhang Y, et al. Hyperphosphorylation of TDP - 43 at S409/S410 promotes its cytoplasmic localization and aggregation. J Biol Chem. 2013;288 (38):27561 - 27573.
- Gendron TF, Petrucelli L. TDP - 43 in neurodegeneration: emerging mechanisms and therapeutic targets. Nat Rev Drug Discov. 2015;14 (2):110 - 123.
- Liu X, Zhang X, Wang Y, et al. Dysregulation of cardiac contractility - related genes in ALS - associated cardiomyopathy due to TDP - 43 abnormalities. Int J Cardiol. 2021;336:18 - 26.
- Wang Z, Li Y, Zhang H, et al. Transcriptomic analysis reveals dysregulation of calcium - handling genes in cardiac tissue from ALS patients with cardiomyopathy. J Mol Cell Cardiol. 2023;178:1 - 12.
- Yang Y, Zhang X, Liu X, et al. Up - regulation of inflammatory cytokines in the hearts of ALS patients with cardiomyopathy. Inflamm Res. 2022;71 (12):1427 - 1438.
- Wang Y, Yang Y, Liu X, et al. TDP - 43 aggregates activate the NLRP3 inflammasome in cardiac cells. J Mol Cell Cardiol. 2023;174:80 - 91.
- Li Yingying, Sun Yuanzheng, Wang Shilin, et al. Research Progress on Acupuncture Treatment for Amyotrophic Lateral Sclerosis [J]. Journal of Traditional Chinese Medicine,2024,39(08):1701-1706.
- Zhou Yujun, Chen Qiuyu, Sun Zhuo, et al. Research Progress on the Pathogenesis and Drugs of Amyotrophic Lateral Sclerosis [J]. Chinese Journal of Pharmacology,2024,40(02):201-207.
- Mercuri Eugenio,Pichiecchio Anna,Allsop Joanna,et al. Muscle MRI in inherited neuromuscular disorders:past, present,and future.[J]. Journal of magnetic resonance imaging : JMRI,2007,25(2):433-40.
- Zou Yi, Liu Ying, Li Surenong, et al. Analysis of clinical and neuroelectrophysiological characteristics of patients with amyotrophic lateral sclerosis [J]. Epilepsy and Neuroelectrophysiology Journal, 2014, 23(1): 29-31 + 40.
- BERRY J D, CUDKOWICZ M E, WINDEBANK A J, et al. NurOwn, phase 2, randomized, clinical trial in patients with ALS: safety, clinical, and biomarker results [J]. Neurology, 2019, 93(24): e2294-e2305.
- CUDKOWICZ M E, LINDBORG S R, GOYAL N A, et al. A randomized placebo-controlled phase 3 study of mesenchymal stem cells induced to secrete high levels of neurotrophic factors in amyotrophic lateral sclerosis [J]. Muscle Nerve, 2022, 65(3): 291-302.
- Yue Jiao, Gong Mei-Ting, et al. Effect and mechanism of TDP-43 on oxygen-glucose deprivation-induced apoptosis in mouse HL-1 atrial myocytes cells[J]. Med J Chin PLA, 2023, 48(11): 1305-1313.
- Dai Wei, Kang Lianming. New Advances in the Treatment of Cardiomyopathy [J]. Chinese Journal of Cardiovascular Diseases, 2020, 04(1) : 1-10.
- WilderT, RybaDM, WieczorekDF, et al. N-acetylcysteine reverses diastolic dysfunction and hypertrophy in familial hypertrophic cardiomyopathy[J]. Am J Physiol Heart Circ Physiol, 2015,309(10):H1720-1730.
- Wang Zhentao. Current Status and Thoughts on Chinese Medicine Treatment of Dilated Cardiomyopathy[J]. ACTA Chinese Medicine, 2025,40(323):679-687.
- XU Yuqian. Professor Wang Zhentao's Experience in Differentiating and Treating Dilated Cardiomyopathy from "Sunken Thoracic Qi"[J]. Western Journal of Traditional Chinese Medicine,2023,36(7):60-64.
Figure 1.
Genes and mechanisms related to the pathogenesis of ALS.
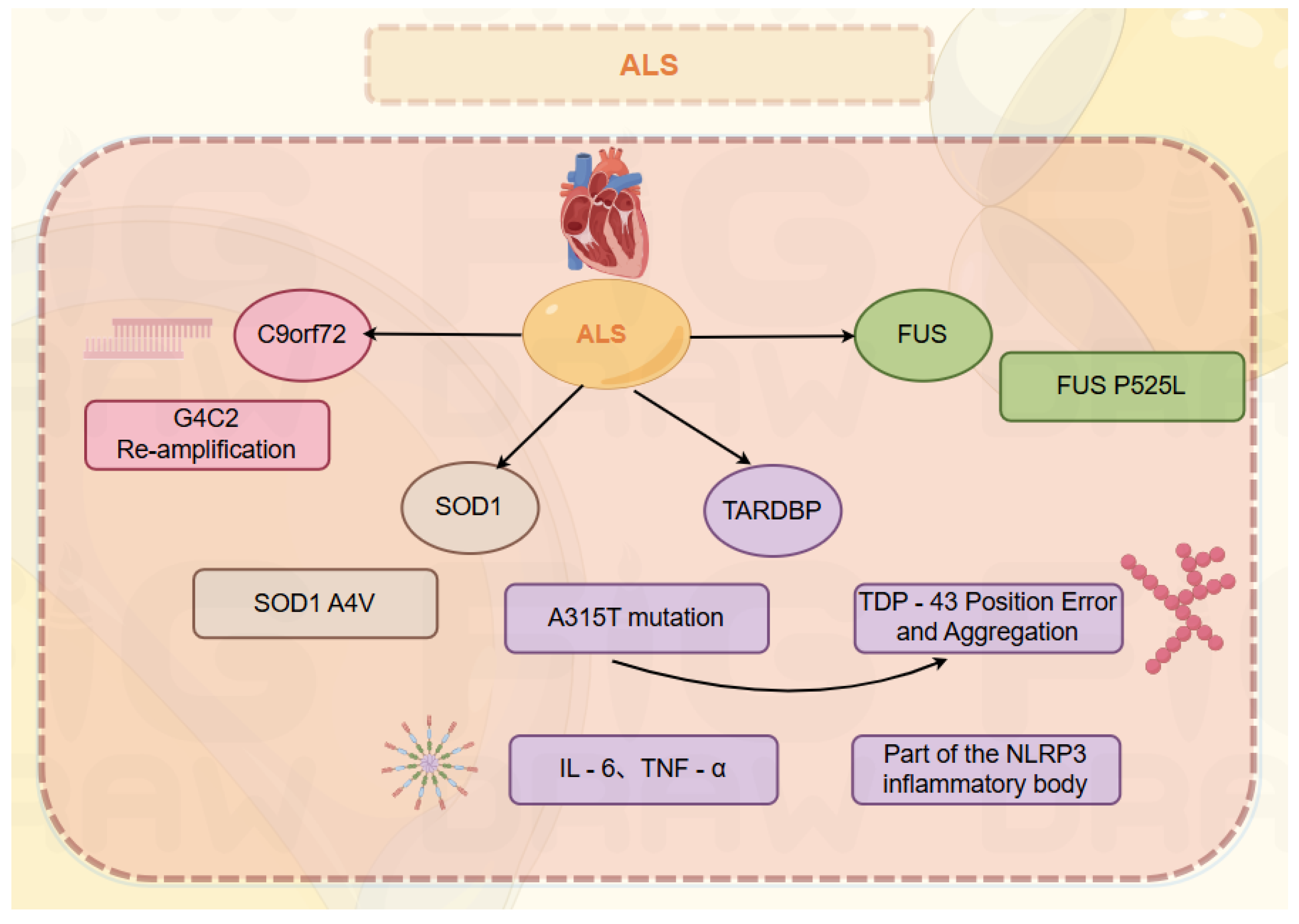
Figure 2.
The physiological functions of the liver, heart, spleen and kidney in traditional Chinese medicine.
Figure 2.
The physiological functions of the liver, heart, spleen and kidney in traditional Chinese medicine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



