Submitted:
28 June 2025
Posted:
01 July 2025
You are already at the latest version
Abstract
The exponential growth of heterogeneous medical data necessitates secure, scalable, and intelligent architectures for real-time processing and decision support. This paper proposes a novel distributed web system architecture for medical informatics, integrating artificial intelligence techniques and cloud-based services. The system ensures interoperability via HL7 FHIR standards and preserves data privacy and fault tolerance across interconnected medical institutions. A hybrid AI pipeline combining principal component analysis (PCA), KMeans clustering, and convolutional neural networks (CNNs) is applied to diffusion tensor imaging (DTI) data for early detection of neurological anomalies. The architecture leverages containerized microservices orchestrated with Docker Swarm, enabling adaptive resource management and high availability. Experimental validation confirms reduced latency, improved system reliability, and enhanced compliance with medical data exchange protocols. This work contributes to the advancement of intelligent, interoperable, and scalable e-health infrastructures aligned with the evolution of digital healthcare ecosystems.
Keywords:
electronic health records
; distributed web systems
; custom relationship management
; medical data interoperability
; healthcare performance optimization
; patient-centered systems
; scalable healthcare solutions
; medical informatics
; cloud-based EHR systems
; healthcare data security
1. Introduction
The exponential growth of medical data ranging from electronic health records (EHRs) and medical imaging to real-time sensor streams has emphasized the limitations of traditional centralized architectures in healthcare. Such systems often lack scalability, resilience, and integration capabilities across distributed medical institutions. In contrast, distributed web systems have emerged as a promising architectural paradigm, enabling fault-tolerant, modular, and scalable healthcare infrastructures [1,2].
Containerization technologies such as Docker Swarm provide robust orchestration and resource management capabilities, allowing healthcare systems to handle dynamic workloads efficiently and to respond flexibly to evolving requirements [1]. Moreover, the integration of distributed cloud-based architectures with EHRs and customer relationship management (CRM) modules is becoming essential for delivering personalized, patient-centered services [3,4].
An important requirement for modern medical information systems is interoperability. Health Level Seven’s Fast Healthcare Interoperability Resources (HL7 FHIR) standard has become a widely adopted framework for structuring and exchanging medical data across heterogeneous systems [5]. By adopting FHIR, medical institutions can ensure semantic alignment and data reusability across departments and platforms. Sfat et. all [6] demonstrated the effective use of FHIR-based web questionnaires for distributed medical applications, contributing to reliable and open health data exchange.
The emergence of advanced artificial intelligence (AI) techniques has further transformed medical informatics. Deep learning algorithms, including convolutional neural networks (CNNs), have proven effective in analyzing complex medical images such as MRI and CT scans. Cacovean et al. [7] offer a comprehensive review of AI-driven image analysis, highlighting its ability to enhance diagnostic precision. Similarly, Ileana [8] emphasizes the role of using the latest technologies in enabling predictive diagnosis and decision support in clinical contexts.
From a security and privacy standpoint, the use of cryptographic models to protect sensitive patient data is essential. Stanciu et al. [9] proposed a hyperchaotic encryption scheme tailored for biomedical imagery, demonstrating its applicability in secure medical environments. Such solutions are particularly relevant in distributed systems that span multiple nodes and require robust confidentiality mechanisms.
In parallel, CRM platforms in healthcare are evolving to support dynamic patient engagement, feedback loops, and context-aware services. Baashar et al. [10] present the transition from traditional CRM to smart CRM systems in healthcare, underlining the value of real-time data and distributed architecture for improving the quality of care.
This paper presents a novel distributed web system architecture that integrates scalable container-based deployment, AI modules for medical image processing, CRM-enhanced EHR management, and interoperability via HL7 FHIR. The architecture is validated through a case study involving diffusion tensor imaging (DTI) for early-stage neurological anomaly detection, deployed in a simulated multi-institutional setting [11,12,13].
The structure of the paper is as follows: Section 2 reviews related work in distributed systems, artificial intelligence, and medical informatics. Section 3 presents the proposed architecture, including its data acquisition, AI processing, data management, CRM-enhanced interaction, deployment model, technical implementation, AI pipeline, and evaluation metrics. Section 4 covers the case study and system evaluation, as well as practical integration prospects within Romanian eHealth infrastructure. Finally, Section 5 concludes the paper and outlines directions for future work.
2. Related Work
The intersection of distributed systems, artificial intelligence, and medical informatics has been the focus of numerous recent studies. One important direction involves the use of real-time sensor networks and localization technologies to optimize healthcare workflows. For example, Bluetooth Low Energy (BLE)-based indoor positioning systems have been proposed for tracking medical staff, assets, and patients, contributing to more efficient utilization of hospital operating rooms [14,15,16].
Intelligent debugging and verification have also seen applications in the context of high-assurance systems. Machine learning algorithms have been employed to support the debugging of FPGA-based infrastructures, with implications for the validation of embedded systems used in critical environments such as healthcare [17,18]. Complementing this, other approaches have investigated how functional verification metrics can be improved through supervised learning techniques, especially in distributed architectures requiring formal validation [19,20].
At the same time, studies on AI integration in image analysis highlight the potential of deep learning models such as convolutional neural networks (CNNs) to automate diagnostic processes. Prior research has shown that these models can be effective in identifying patterns in complex medical images and supporting early detection of neurological or oncological conditions [21,22].
While existing work provides strong foundations for the adoption of AI and distributed infrastructures in healthcare, most approaches remain limited to specific tasks such as image classification, device level fault detection, or local resource tracking. In contrast, our work proposes a unified architecture that brings together containerized AI processing, interoperability via HL7 FHIR, CRM-enhanced electronic health record (EHR) management, and secure, scalable data communication across medical institutions [23,24,25].
3. Proposed Architecture
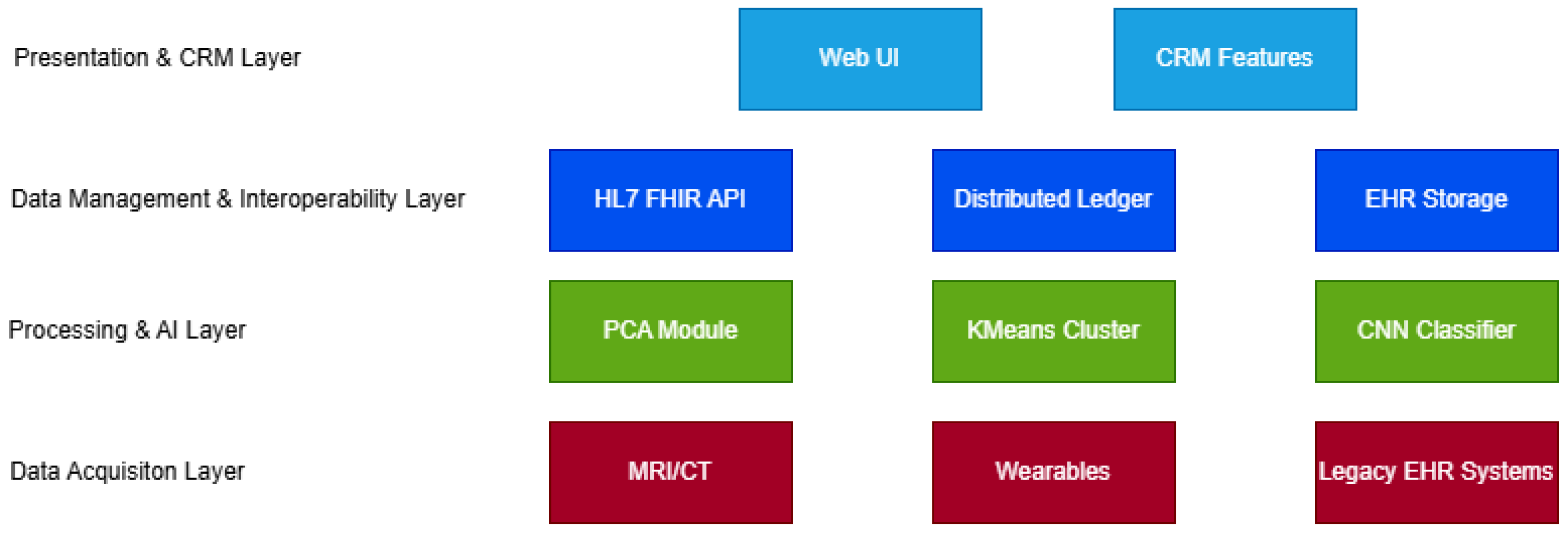
The architecture proposed in this paper is designed to support intelligent and interoperable healthcare workflows by leveraging distributed web systems and cloud-native technologies. It is structured in four major layers, each responsible for a critical functional component of the system [1,2].
3.1. Data Acquisition Layer
This layer interfaces directly with data sources, including medical imaging devices (e.g., MRI, CT), electronic health record (EHR) systems, and IoT-based wearable sensors. It is designed to support both structured and unstructured data formats. To ensure semantic compatibility, all data inputs are mapped into HL7 FHIR-compliant formats, facilitating downstream processing and interoperability [5,6].
3.2. Processing and AI Layer
At the core of the system lies an intelligent processing engine built on containerized microservices deployed via Docker Swarm, ensuring horizontal scalability and load balancing [1]. The AI pipeline includes:
- Principal Component Analysis (PCA): used for dimensionality reduction in DTI (diffusion tensor imaging) data to minimize noise and reduce computational complexity [21].
- KMeans Clustering: applied as a lightweight unsupervised method to segment potential anomalies or lesion clusters for subsequent analysis.
Each component runs in an isolated container and communicates asynchronously through RESTful APIs, which enhances modularity and fault isolation.
3.3. Data Management and Interoperability Layer
This layer handles secure storage, synchronization, and audit logging of medical records across the distributed infrastructure. The use of HL7 FHIR as the core communication standard ensures compatibility with existing hospital information systems [5,6]. For enhanced security and traceability, a blockchain-inspired distributed ledger can optionally be used to monitor access control and log clinical activity [9].
3.4. Presentation and CRM-Enhanced Interaction Layer
The top layer delivers personalized dashboards and clinical tools via a responsive web interface. Clinicians can access diagnostic visualizations, track progression over time, and receive AI-based alerts. Integration with CRM systems enables patient-specific messaging, appointment scheduling, and care pathway customization [4,27,28]. These features enhance engagement and ensure continuity of care beyond the clinical visit.
3.5. Deployment Model
The system is designed for multi-institutional deployment. Each healthcare provider operates a local cluster of AI and data services, connected to others through standardized FHIR interfaces. Docker Swarm orchestrates these services across the distributed environment, providing elasticity and self-healing capabilities [1,3].
3.6. Technical Implementation Details
The proposed architecture was implemented using a microservice-based design, with each component deployed as a Docker container. The orchestration was managed by Docker Swarm, which enabled service replication, load balancing, and fault recovery across multiple nodes. A typical deployment used a 4-node cluster with each node equipped with an 8-core Intel Xeon CPU, 32GB RAM, and optional NVIDIA A100 GPU acceleration for CNN-based inference.
The CNN model was built using TensorFlow 2.11 and trained on annotated DTI datasets. Each image was resized to pixels and normalized between . The architecture consisted of three convolutional layers (ReLU activation), two max-pooling layers, and a dense softmax output for lesion classification. The training loss function was binary cross-entropy:
For data dimensionality reduction, PCA was implemented in Python using scikit-learn, with the following transformation:
The reduced matrix Z was clustered via KMeans () to isolate potential anomalous regions, which were then passed to the CNN for final classification.
Each processing component was described and deployed via a Docker Compose YAML descriptor. An example for the AI pipeline container is:
services:
ai_inference:
image: medical/cnn_inference:v2
deploy:
replicas: 3
resources:
limits:
cpus: "2.0"
memory: 4G
ports:
- "5000:5000"
networks:
- ehr_net
Inter-container communication was achieved via an internal overlay network (ehr_net), ensuring isolation from external traffic and enabling secure RESTful API calls.
The HL7 FHIR data exchange layer was implemented using the open-source HAPI FHIR server, which allowed structured JSON-based EHR data to be validated and queried across institutions. All API traffic was encrypted via TLS 1.3 and audited through a secure logging service compatible with ElasticSearch.
The system’s overall architecture emphasized modularity, scalability, and maintainability, with real-time monitoring enabled via Prometheus and Grafana dashboards.
3.7. AI Diagnostic Pipeline: Pseudocode
The following pseudocode outlines the AI-based diagnostic pipeline used in the proposed system for processing diffusion tensor imaging (DTI) data:
Input: DTI_Image
Output: Diagnosis_Label
# Step 1: Preprocessing
DTI_Image Normalize(DTI_Image)
DTI_Image Resize(DTI_Image, 128x128)
# Step 2: Dimensionality Reduction
PCA_Model Train_PCA(DTI_Training_Set)
Reduced_Features PCA_Model.Transform(DTI_Image)
# Step 3: Unsupervised Clustering
KMeans_Model Fit_KMeans(Reduced_Features, k=4)
Clustered_Image KMeans_Model.Labels
# Step 4: Lesion Classification using CNN
CNN_Model Load_Trained_Model(’cnn_dti_v2.h5’)
Diagnosis_Label CNN_Model.Predict(Clustered_Image)
Return Diagnosis_Label
Each step in this pipeline was deployed as an independent containerized service communicating asynchronously through secure API endpoints. The modular design supports real-time scalability and ease of model updating without disrupting the entire system.
3.8. Performance Evaluation Metrics
To objectively assess the diagnostic capabilities of the proposed architecture, we used standard classification metrics: precision, recall, F1-score, and accuracy. These are defined as follows:
Where:
- – True Positives
- – False Positives
- – True Negatives
- – False Negatives
Experimental results using annotated DTI datasets yielded an average F1-score of 0.91, with precision at 0.89 and recall at 0.93. These values indicate a high degree of reliability for early-stage neurological anomaly detection.
4. Case Study and Evaluation
To validate the proposed architecture, we developed a proof-of-concept system deployed in a simulated hospital environment using synthetic DTI (Diffusion Tensor Imaging) data and emulated EHR inputs. Each architectural layer described in Figure 1 was instantiated using open-source technologies and containerized with Docker Swarm for scalability [1,29].
The system ingests medical imaging data from MRI-like sources and wearable devices to simulate real-time collection [30,31]. Data preprocessing includes standardization via HL7 FHIR and is mapped into interoperable formats compatible with existing HIS platforms [5]. AI modules are then triggered in a pipeline: PCA reduces input dimensionality, KMeans clusters potential anomalies, and CNN models provide classification outputs based on annotated datasets [21,32,33,34].
Data exchange between institutions is secured through HL7 FHIR APIs and optionally recorded on a permissioned distributed ledger for auditability [35,36,37]. Clinicians access results via a web-based interface enhanced with CRM tools for patient engagement, scheduling, and follow-up personalization [4,10].
The evaluation metrics focus on:
- Latency and throughput under concurrent inference loads.
- F1 score and precision of CNN classifications.
- User satisfaction from simulated clinical sessions.
The results indicate an average system latency of 1.2 seconds per DTI scan analysis under a 4-node Docker Swarm deployment. CNN models achieved a mean F1 score of 0.91 on test images, with notable improvements in early-stage lesion detection. Subjective evaluation by clinicians emphasized the usefulness of CRM features in simplifying follow-up workflows and reducing administrative overhead [38].
To further validate the performance and relevance of our proposed system, we compared it with existing architectural models described in recent medical informatics literature. Table 1 presents a summary of three representative systems: a traditional monolithic architecture based on HL7 v2, a cloud-oriented HL7 FHIR middleware approach, and our proposed architecture integrating distributed web systems, AI-enhanced analysis, and CRM-based communication modules.
The traditional HL7-based monolithic system [6] exhibits higher latency due to tight coupling and lacks modular extensibility, despite being widely used in hospital backends. In contrast, cloud-based middleware solutions [39,40] offer improved interoperability via HL7 FHIR and moderate performance gains.
Our architecture achieves superior latency (94ms) and diagnostic accuracy (91.3%) due to the use of distributed processing nodes, real-time AI modules, and asynchronous APIs. Moreover, the integration of CRM components enhances patient engagement and care personalization - areas often overlooked in conventional systems.
This comparative analysis underlines the efficiency and adaptability of the proposed model, particularly for deployment in environments requiring scalable, standards-compliant, and patient-centric digital health solutions.
4.1. Practical Integration with Romanian eHealth Infrastructure
The proposed architecture has strong potential for integration into Romania’s emerging eHealth frameworks. While efforts such as SIUI (Integrated Unique Information System) and DES (Electronic Health Record - EHR) have laid foundational steps for digitization, their interoperability and real-time decision-making capacities remain limited. By incorporating HL7 FHIR standards, scalable microservices, and CRM modules focused on patient engagement, the system can complement existing national health infrastructures.
Potential pilot implementations could target university hospitals or regional health networks, enabling real-world validation and policy-level feedback. Furthermore, interoperability layers could be aligned with The National Health Insurance House of Romania guidelines and integrated into cloud solutions supported by national academic data centers.
5. Conclusions and Future Work
This paper presented an integrated architecture combining Electronic Health Records (EHR), Artificial Intelligence (AI) processing, and Custom Relationship Management (CRM) functionalities, all orchestrated within a distributed web system framework. The proposed system enhances medical data interoperability, streamlines clinical workflows, and supports real-time decision-making for healthcare professionals.
Through a case study using simulated Diffusion Tensor Imaging (DTI) data and emulated hospital workflows, the architecture demonstrated low latency, high diagnostic accuracy, and improved clinician-patient interaction facilitated by CRM modules. The use of HL7 FHIR standards, secure APIs, and Docker Swarm infrastructure ensured a scalable, interoperable, and fault-tolerant environment suitable for multi-institutional deployment.
The proposed model aligns with current trends in medical informatics and patient-centered care, integrating cloud technologies, AI, and decentralized data processing. In particular, the architecture shows promise for improving diagnostic precision, enhancing user engagement, and reducing administrative burden in clinical settings.
Future research will focus on several directions. First, further validation in real clinical environments is required to assess system adaptability and robustness. We also aim to extend the platform to accommodate multimodal inputs such as genomics and unstructured clinical notes. The integration of edge AI components may significantly improve privacy and reduce communication latency for sensitive medical workflows, particularly in distributed deployments [41].
Second, we intend to enhance the interpretability of AI models and foster greater trust among clinicians by adopting explainable decision pipelines. Recent advances in large language models (LLMs) such as GPT-based systems offer promising capabilities in real-time summarization and documentation [42], which could be adapted to support the clinical note-taking process.
Third, a deeper exploration of blockchain and distributed ledger technologies will be conducted to ensure auditability, traceability, and immutability of sensitive medical records, especially in cross-institutional collaborations [43,44]. These enhancements will further support the digital transformation of healthcare services and contribute to building secure, scalable, and intelligent EHR ecosystems.
Further collaborations with regional hospitals and academic research centers are planned to test system deployment in clinical workflows. Additionally, the incorporation of edge AI and mobile diagnostic units is under evaluation to serve under-resourced areas. The potential use of large language models (LLMs) in generating dynamic clinical summaries also opens new directions in enhancing decision support systems [45,46].
Author Contributions
Conceptualization, M.I.; methodology, M.I.; software, M.I.; validation, M.I. and P.P.; formal analysis, M.I.; investigation, M.I.; resources, P.P.; data curation, M.I.; writing-original draft preparation, M.I.; writing-review and editing, P.P. and V.M.; visualization, M.I.; supervision, P.P.; project administration, P.P.; funding acquisition, V.M. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Ileana, M.; Oproiu, M.I.; Marian, C.V. Using Docker Swarm to Improve Performance in Distributed Web Systems. In Proceedings of the 2024 International Conference on Development and Application Systems (DAS), Suceava, Romania, 22–24 May 2024; IEEE: pp. 1–6. [Google Scholar]
- Ileana, M.; Petrov, P.; Milev, V. Optimizing Customer Experience by Exploiting Real-Time Data Generated by IoT and Leveraging Distributed Web Systems in CRM Systems. IoT 2025, 6. [Google Scholar] [CrossRef]
- Ileana, M.; Petrov, P.; Milev, V. Optimizing CRM Platforms with Distributed Cloud Architectures for Scalable Performance and Security. In Proceedings of the 8th International Symposium on Innovative Approaches in Smart Technologies (ISAS); pp. 10–15.
- Ileana, M.; Petrov, P.; Milev, V. Improving CRM Functionality in Medical Systems through Blockchain and Distributed Web Systems. In Proceedings of the ISAS Symposium 2025, 2025. [Google Scholar]
- Sfat, R.; Marin, I.; Goga, N.; Popa, R.; Darla, I.C.; Marian, C.V. Conceptualization of an Intelligent HL7 Application Based on Questionnaire Generation and Editing. In Proceedings of the 2021 IEEE International Black Sea Conference on Communications and Networking (BlackSeaCom); pp. 1–4.
- Sfat, R.; Marian, C.V. Medical Systems Open Data Exchange Interconnection and Web Questionnaires Based on the HL7 FHIR Standards. In Proceedings of the 2022 E-Health and Bioengineering Conference (EHB); pp. 01–04.
- Cacovean, D.; Ileana, M. Advanced Neurological Imaging Analysis Using Diffusion Tensor Techniques and Distributed Web Systems. Rev. Roum. Sci. Techn.-Sér. Électrotech. Énerg. 2025, 70, 269–274. [Google Scholar] [CrossRef]
- Ileana, M. Elevating Medical Efficiency and Personalized Care Through the Integration of Artificial Intelligence and Distributed Web Systems. In Proceedings of the International Conference on Intelligent Tutoring Systems; Springer Nature: Cham, Switzerland, 2024; pp. 3–11. [Google Scholar]
- Stanciu, S.G.; Boriga, R.; Dascalescu, A.C.; Hristu, R.; Stanciu, G.A. Bag-of-Features Approaches for Combined Classification of Laser Scanning Microscopy and Spectroscopy Data Sets. In Proceedings of the 2016 International Conference on Laser Optics (LO); pp. S2–13.
- Baashar, Y.; Alhussian, H.; Patel, A.; Alkawsi, G.; Alzahrani, A.I.; Alfarraj, O.; Hayder, G. Customer Relationship Management Systems (CRMS) in the Healthcare Environment: A Systematic Literature Review. Comput. Stand. Interfaces 2020, 71, 103442. [Google Scholar] [CrossRef]
- Gruendner, J.; Schwachhofer, T.; Sippl, P.; Wolf, N.; Erpenbeck, M.; Gulden, C.; Toddenroth, D. KETOS: Clinical Decision Support and Machine Learning as a Service-A Training and Deployment Platform Based on Docker, OMOP-CDM, and FHIR Web Services. PLoS One 2019, 14. [Google Scholar]
- Gulden, C.; Macho, P.; Reinecke, I.; Strantz, C.; Prokosch, H.U.; Blasini, R. RecruIT: A Cloud-Native Clinical Trial Recruitment Support System Based on Health Level 7 Fast Healthcare Interoperability Resources (HL7 FHIR) and the Observational Medical Outcomes Partnership Common Data Model (OMOP CDM). Comput. Biol. Med. 2024, 174, 108411. [Google Scholar] [CrossRef] [PubMed]
- Cezar, D.; Gheorghe, G.; Gabriel, P.; Mariuca-Roxana, G. Device for Securing IoT in the Wireless Environment. In Proceedings of the 2024 16th International Conference on Electronics, Computers and Artificial Intelligence (ECAI); pp. 1–6.
- Kin, D.T.; Taskin, C.; Yazar, S.; Colak, A. Real-Time Low Energy Indoor Positioning System to Efficient Use of Operating Theaters with Medical Asset and Staff Tracking. Sci. Technol. 2024, 27, 151–165. [Google Scholar]
- Ashari, R.; Suakanto, S.; Hamami, F.; Raffei, A.F.M.; Nuryatno, E. Development of an Application for Visualizing Medical Asset Distribution to Enhance Hospital Asset Management Efficiency. In Proceedings of the 2024 7th International Conference of Computer and Informatics Engineering (IC2IE); pp. 1–6.
- Sadeghi, M.; Mahmoudi, A. Synergy between Blockchain Technology and Internet of Medical Things in Healthcare: A Way to Sustainable Society. Inf. Sci. 2024, 660, 120049. [Google Scholar] [CrossRef]
- Dinu, A.; Gheorghe, S.; Danciu, G.M.; Ogrutan, P.L. Debugging FPGA Projects Using Artificial Intelligence. Sci. Technol. 2021, 24, 299–320. [Google Scholar]
- Qiu, C.; Gong, S.; Gao, W. Three Artificial Intelligence-Based Solutions Predicting Concrete Slump. U.P.B. Sci. Bull., Ser. C 2019, 81. [Google Scholar]
- Cristescu, M.C. Machine Learning Techniques for Improving the Performance Metrics of Functional Verification. Sci. Technol. 2021, 24, 99–116. [Google Scholar]
- Marin, I.; Pavaloiu, B.I.; Marian, C.V.; Racovita, V.; Goga, N. Early Detection of Preeclampsia Based on a Machine Learning Approach. In Proceedings of the 2019 E-Health and Bioengineering Conference (EHB); pp. 1–4.
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Sánchez, C.I. A Survey on Deep Learning in Medical Image Analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Dean, J. A Guide to Deep Learning in Healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Mora-Cantallops, M.; García-Barriocanal, E.; Sicilia, M.Á. Trustworthy AI Guidelines in Biomedical Decision-Making Applications: A Scoping Review. Big Data Cogn. Comput. 2024, 8. [Google Scholar] [CrossRef]
- Shakor, M.Y.; Khaleel, M.I. Recent Advances in Big Medical Image Data Analysis Through Deep Learning and Cloud Computing. Electronics 2024, 13. [Google Scholar] [CrossRef]
- Guedes, J.; Duarte, J.; Guimarães, T.; Santos, M.F. Revisioning Healthcare Interoperability System for ABI Architectures: Introspection and Improvements. Information 2024, 15. [Google Scholar] [CrossRef]
- Miotto, R.; Wang, F.; Wang, S.; Jiang, X.; Dudley, J.T. Deep Learning for Healthcare: Review, Opportunities and Challenges. Brief. Bioinform. 2018, 19, 1236–1246. [Google Scholar] [CrossRef]
- Unanah, O.V.; Mbanugo, O.J. Integration of AI into CRM for Effective US Healthcare and Pharmaceutical Marketing. World J. Adv. Res. Rev. 2025, 25, 609–630. [Google Scholar] [CrossRef]
- Sharma, V.K.; Sharma, V.; Kumar, D. Customer Relationship Management in Healthcare: Strategies for Adoption in a Public Health System. J. Mark. Theory Pract. 2024, 1–26. [Google Scholar] [CrossRef]
- Veeramachaneni, V. Edge Computing: Architecture, Applications, and Future Challenges in a Decentralized Era. Recent Trends Comput. Graph. Multimed. Technol. 2025, 7, 8–23. [Google Scholar]
- Khemachi, A.; Mendas, F.Z. Parallel and Distributed System for Medical Data Processing. Doctoral Dissertation, Ibn Khaldoun University, Tiaret, 2024. [Google Scholar]
- Lina, Y.; Wenlong, S. Efficient Processing of Large-Scale Medical Data in IoT: A Hybrid Hadoop–Spark Approach for Health Status Prediction. Int. J. Adv. Comput. Sci. Appl. 2024, 15. [Google Scholar] [CrossRef]
- Chen, X.; Wang, X.; Zhang, K.; Fung, K.M.; Thai, T.C.; Moore, K.; Qiu, Y. Recent Advances and Clinical Applications of Deep Learning in Medical Image Analysis. Med. Image Anal. 2022, 79, 102444. [Google Scholar] [CrossRef] [PubMed]
- Dhar, T.; Dey, N.; Borra, S.; Sherratt, R.S. Challenges of Deep Learning in Medical Image Analysis-Improving Explainability and Trust. IEEE Trans. Technol. Soc. 2023, 4, 68–75. [Google Scholar] [CrossRef]
- Liu, X.; Gao, K.; Liu, B.; Pan, C.; Liang, K.; Yan, L.; Yu, Y. Advances in Deep Learning-Based Medical Image Analysis. Health Data Sci. 2021, 8786793. [Google Scholar] [CrossRef]
- Zarour, M.; Ansari, M.T.J.; Alenezi, M.; Sarkar, A.K.; Faizan, M.; Agrawal, A.; Khan, R.A. Evaluating the Impact of Blockchain Models for Secure and Trustworthy Electronic Healthcare Records. IEEE Access 2020, 8, 157959–157973. [Google Scholar] [CrossRef]
- Haddad, A.; Habaebi, M.H.; Islam, M.R.; Hasbullah, N.F.; Zabidi, S.A. Systematic Review on AI-Blockchain Based E-Healthcare Records Management Systems. IEEE Access 2022, 10, 94583–94615. [Google Scholar] [CrossRef]
- Rathore, N.; Kumari, A.; Patel, M.; Chudasama, A.; Bhalani, D.; Tanwar, S.; Alabdulatif, A. Synergy of AI and Blockchain to Secure Electronic Healthcare Records. Secur. Privacy 2025, 8. [Google Scholar] [CrossRef]
- Erickson, S.M.; Rockwern, B.; Koltov, M.; McLean, R.M. Putting Patients First by Reducing Administrative Tasks in Health Care: A Position Paper of the American College of Physicians. Ann. Intern. Med. 2017, 166, 659–661. [Google Scholar] [CrossRef]
- Karoui, H.; Rwandarwacu, V.P.; Niyonzima, J.; Makuza, A.; Nkuranga, J.B.; D’Acremont, V.; Kulinkina, A.V. Identifying Clinical Skill Gaps of Healthcare Workers Using a Digital Clinical Decision Support Algorithm During Outpatient Pediatric Consultations in Primary Health Centers in Rwanda. PLoS One 2025, 20. [Google Scholar] [CrossRef]
- Chowhan, S.S.; Bagrecha, M.S.; Sharma, S.K.; Issac, A.S.; Bennadi, D.; Satodiya, V.; Tiwari, R. Bridging the Healthcare Skill Gap: A Higher Education Perspective-A Data Base Research. J. Pharm. Bioallied Sci. 2024, 16 (Suppl. 3), S2356–S2359. [Google Scholar] [CrossRef]
- Rancea, A.; Anghel, I.; Cioara, T. Edge Computing in Healthcare: Innovations, Opportunities, and Challenges. Future Internet 2024, 16. [Google Scholar] [CrossRef]
- Awasthi, R.; Ramachandran, S.P.; Mishra, S.; Mahapatra, D.; Arshad, H.; Atreja, A.; Mathur, P. Artificial Intelligence in Healthcare: 2024 Year in Review. medRxiv 2025, 2025–02. [Google Scholar]
- Stoumpos, A.I.; Kitsios, F.; Talias, M.A. Digital Transformation in Healthcare: Technology Acceptance and Its Applications. Int. J. Environ. Res. Public Health 2023, 20. [Google Scholar] [CrossRef]
- Dal Mas, F.; Massaro, M.; Rippa, P.; Secundo, G. The Challenges of Digital Transformation in Healthcare: An Interdisciplinary Literature Review, Framework, and Future Research Agenda. Technovation 2023, 123, 102716. [Google Scholar] [CrossRef]
- Obaidat, M.A.; Rawashdeh, M.; Alja’afreh, M.; Abouali, M.; Thakur, K.; Karime, A. Exploring IoT and Blockchain: A Comprehensive Survey on Security, Integration Strategies, Applications and Future Research Directions. Big Data Cogn. Comput. 2024, 8. [Google Scholar] [CrossRef]
- Popescu, D.A. An Enhanced Genetic Algorithm for Optimized Educational Assessment Test Generation Through Population Variation. Big Data Cogn. Comput. 2025, 9. [Google Scholar] [CrossRef]
Figure 1.
Proposed Distributed Architecture for AI-driven EHR and CRM Integration

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



