Submitted:
06 June 2025
Posted:
09 June 2025
You are already at the latest version
Abstract
Background: Aesthetic dentistry increasingly demands minimally invasive, predictable, and patient-centered solutions. Digital technologies and AI-driven planning tools are now integral to interdisciplinary treatments. Aim: To evaluate patients’ perception of smile aesthetics and oral function before and after receiving clear aligner therapy followed by minimally invasive ceramic veneers, using digital planning and pre-visualization tools. Materials and Methods: five adult patients underwent digital smile design, clear aligner therapy, and feldspathic veneer placement. Pre- and post-treatment perception of smile aesthetics and function were assessed using a structured questionnaire. AI-based simulation tools (2D and 4K TruSmile video previews) were incorporated. Paired t-tests were used to compare outcomes before and after treatment. Results: Mean pre-treatment scores were 4.8 for smile aesthetics and 6.6 for function. Post-treatment scores significantly improved to 9.8 (p = 0.001) and 9.4 (p = 0.002), respectively. Patients rated AI-generated smile previews more favorably than 2D designs and acknowledged the value of digital tools in understanding and accepting treatment. Conclusions : The integration of digital and AI-based tools in aesthetic dentistry enhances patient communication, improves predictability, and enables minimally invasive treatment. Patient satisfaction was high, underscoring the effectiveness of the combined orthodontic and prosthetic approach.
Keywords:
aesthetics
; veneers
; smile creator
; smile desgin
; aligners
; mock-up
1. Introduction
The concept of a “perfect smile” extends beyond mere dental alignment—it encompasses a balance of esthetic harmony, emotional expression, and functional stability. In contemporary society, an attractive smile is often perceived as a symbol of health, confidence, and social appeal. As a result, dental esthetics has become a major focus of both patient expectations and clinical practice. The modern demand for smile enhancement has shifted from purely functional restorations toward treatments that incorporate both beauty and subtlety, with patients increasingly seeking outcomes that appear naturally aesthetic rather than unnaturally white or artificial. Achieving a smile that is both visually appealing and natural remains a central challenge in restorative dentistry. The goal is to meet patients’ esthetic expectations while preserving dental tissues through minimally invasive procedures. In this context, ceramic laminate veneers—particularly those fabricated from feldspathic and glass-ceramic materials—are recognized for their excellent survival rates and minimal biological cost [1,2]. However, optimal esthetic and functional outcomes depend heavily on the position and alignment of the anterior teeth, which influence both the visual proportions of the smile and the occlusal balance. Pre-prosthetic orthodontics plays a crucial role in establishing ideal spatial conditions and proper tooth inclination for restorations, especially in cases where a confirmative prosthetic approach is desired [3]. Recent advances in clear aligner therapy offer a patient-friendly orthodontic alternative that supports this paradigm of minimally invasive, prosthetically guided treatment. Aligner systems can be used to achieve precise tooth movements aligned with the final restorative outcome, often improving both functional parameters and patient acceptance [3,4]. These systems are particularly valuable when employed as part of an interdisciplinary approach that integrates orthodontic and prosthetic planning from the outset. Digital technologies have revolutionized treatment planning and execution in esthetic dentistry. Tools such as Digital Smile Design (DSD) allow clinicians to evaluate the spatial relationships between teeth, gingiva, lips, and face using calibrated facial and intraoral imagery [5,6,7]. These tools enable dynamic communication among clinicians, technicians, and patients, promoting shared understanding and facilitating acceptance of the proposed treatment plan. Digital workflows also permit the creation of precise mock-ups and wax-ups that serve both diagnostic and motivational purposes [8,9]. Despite the technical precision and esthetic potential of such treatments, patient satisfaction is ultimately determined by individual perception. The subjective nature of beauty means that clinical success does not always translate to perceived satisfaction. Therefore, evaluating patient-reported outcomes is essential to understanding the effectiveness and acceptance of esthetic treatments [10]. The present study aimed to quantitatively assess patients’ perception of smile esthetics and function before and after receiving an interdisciplinary treatment that combines digital planning, clear aligners, and minimally invasive ceramic veneers. By means of a structured questionnaire, this study seeks to provide insight into how patients experience esthetic transformation and to what extent digital, orthodontic, and prosthetic integration meets their expectations.
2. Materials and Methods
Patients to be treated with aligners and feldspathic veneers, in a private clinic in Rome, Italy, as part of usual professional practice and with no adjunctive risks were enrolled in this study and asked to fill a questionnaire. The data were evaluated at the Department of Medicine, Surgery, and Pharmacy, University of Sassari, Italy. The 2013 Helsinki Declaration and the Good Medical Practice principles were adhered to. Medical data were anonymized so that patients could not be identified. All the patients signed an informed consent for the data acquisition and treatment execution. In addition, according to the European laws, patients also gave consent for photo and video recording, immediately before acquisition, for compliance with the General Data Protection Regulation (GDPR). Ethics committee approval was not requested due to the qualitative nature of the research.
2.1. Inclusion and Exclusion Criteria
Inclusion criteria were: patients in good health; aged at least 18 years; requiring a minimally invasive improvement of the esthetic smile with ceramic veneers in the anterior maxilla; with healthy teeth; and available to be treated with aligners. Exclusion criteria were: patient ASA 3 or 4; untreated periodontitis and/or poor oral hygiene and motivation; heavy smokers (more than 11 cigarettes/day); pregnancy or nursing; substance abusers; psychiatric problems or unrealistic expectations. At the first visit, digital impressions (Medit i700, Medit Corp., Seoul, South Korea), radiographs (orthopantomography), and intraoral and facial photos (Nikon 850, Nikon Corporation, Tokyo, Japan) were taken.
2.2. Standardized Protocol for Patient Photo Recording
Standardized digital images were obtained for each patient, including a full-smile image and a retracted intraoral image captured under consistent lighting and positioning. Buccal corridors were fully exposed using cheek retractors to ensure comprehensive visualization. Key anatomical reference points were manually placed on both the retracted and smiling images to facilitate accurate alignment within dedicated software (exocad Elefsina 3.2, Smile Creator, exocad GmbH, Darmstadt, Germany). Images were adjusted for scale and orientation as needed. A 3D facial scan could be imported to enhance spatial representation and ensure facial harmony in the design. The digital design process included outlining the lip line and other relevant facial reference lines. Esthetic guidelines and curvature lines (e.g., incisal, gingival, midline) were superimposed to guide restorative planning. Virtual modeling of the anterior teeth was performed to achieve the desired shape, proportion, and size, with consideration for natural morphology. Tooth shade and translucency parameters were digitally adjusted to simulate realistic esthetic outcomes. A 3D simulation of the proposed smile was generated to assess visual and functional harmony. A comprehensive smile report (exocad Elefsina 3.2, Smile Creator, exocad GmbH, Darmstadt, Germany) was created, documenting the proposed design along with before-and-after image comparisons. Digital wax-ups were generated to serve as diagnostic and communication tools for both clinical planning and patient education. The software’s automated eye-detection feature was used to enhance facial orientation. Additional design curves and symmetry lines were incorporated to refine esthetic precision. A detailed PDF report was exported to summarize the design process and outcomes. The digitally designed smile was presented to the patient using high-resolution visuals to facilitate understanding and feedback. The approved design served as the foundation for subsequent clinical steps, including mock-ups, provisional restorations, or definitive prosthetic interventions.
2.3. Standardized Protocol for Patient Video Recording
A standardized protocol was followed to ensure consistent and high-quality patient video documentation using a mobile phone (exocad Elefsina 3.2, TruSmile, exocad GmbH). The mobile phone camera (iPhone 13 Pro Max, Apple, Cupertino, USA) was set to 4K (4096p) resolution. The frame rate was set to 60 frames per second (FPS) for optimal balance between quality and file size, and the video was recorded in mov format. All recordings were made in portrait mode to ensure compatibility with final video formatting. No digital or optical zoom was used. Instead, the camera was physically positioned to achieve proper framing. Video duration was limited to 30 seconds. Longer recordings were trimmed using video editing software. The mobile phone was mounted on a tripod to ensure a steady and shake-free recording. A white background was used, avoiding patterns and varying colors. Optimal lighting conditions were ensured by using a ring light placed in front of the patient, aligned with the camera. The camera was positioned directly in front of the patient at the level of the smile, aimed toward the center of the nose. The patient’s head was placed in the upper part of the frame, with the teeth approximately in the center. The framing ensured that the head was neither too large nor too small within the image. A frontal, neutral camera angle was maintained, avoiding high, low, or oblique views. The patient was seated comfortably with hands resting on their lap. Head Position: the head was kept upright and directed straight toward the camera. The patient was instructed to speak naturally throughout the video, smile and laugh spontaneously, and clearly expose their teeth. The patient was also advised to avoid the following during the recording: rapid head or body movements, turning the head excessively such that both mouth corners were not visible, biting the lips or protruding the tongue, covering the mouth with the hands, and moving out of frame.
2.4. Digital Mock-Up
The created design and video were shown and discussed with the patient to assess the esthetic discrepancy between the current and ideal smile, and to evaluate the patient’s expectations. Based on the restorative strategy, orthodontic treatment with clear aligners was selected to reduce the need for aggressive tooth preparation, optimizing minimally invasive veneer preparation. The orthodontic phase was digitally planned using ClinCheck® software (Align Technology, Inc., San Jose, CA, USA), allowing for detailed visualization of the treatment, assessment of occlusion, dental arch asymmetries, and functional analysis. Targeted dental movements were programmed to align the teeth and optimize their position for conservative veneer preparation. Attachments were incorporated as needed to improve movement precision. The patient was instructed to wear upper and lower aligners for 22 hours per day, changing them weekly. The duration of aligner therapy ranged from six to twelve months, depending on initial conditions. Following orthodontic alignment, a digital wax-up of the ideal tooth morphology was created and tested using a mock-up (GC UNIFAST III, GC Europe, Leuven, Belgium). Guided no-prep or minimally invasive veneer preparations were then performed through the mock-up to preserve as much enamel as possible. A vertical finish line design was adopted to allow flexibility in the final cervical contours. Final impressions were taken using the double retraction cord technique and a polyvinyl siloxane material. Feldspathic veneers were fabricated and cemented using adhesive protocols. The enamel was conditioned via sandblasting with 50-μm aluminum oxide, followed by 37% phosphoric acid etching. The veneers were also sandblasted (50 μm, 0.2 MPa), treated with 9.5% buffered hydrofluoric acid, and cleaned with steam. A dedicated primer was applied (Clearfil Ceramic Primer, Kuraray Noritake, Hattersheim, Germany) and maintained for 30 seconds. Finally, the veneers were cemented using PANAVIA V5 Clear (Kuraray Noritake, Germany). Postoperative evaluations were scheduled at one week, one month, and six months to monitor integration of the restorations with soft tissues and assess functional performance. A removable retainer was delivered after one week to ensure long-term stability. An explanatory case is reported in
Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9, Figure 10, Figure 11 and Figure 12.
2.5. Primary Outcome
Patient satisfaction was evaluated using a short form questionnaire (16 questions).
Patient Questionnaire: Evaluation of Digital Smile Design and Treatment Outcomes
-
What were your main reasons for seeking treatment? (Select all that apply):☐ Aesthetics (shape/volume)☐ Function☐ Tooth color☐ Alignment
- On a scale from 0 to 10, how would you rate the aesthetics of your current smile?
- On a scale from 0 to 10, how would you rate the functionality of your current smile (e.g., chewing, speaking)?
-
Would you be willing to undergo orthodontic treatment with aligners to improve aesthetics and/or function?☐ Yes☐ No
-
Regarding tooth shape and appearance, which do you prefer?☐ A natural, harmonious smile☐ An idealized, “perfect” or flawless smile
-
Do you prefer:☐ A natural tooth color☐ A bright “super white” shade
- On a scale from 0 to 10, how would you rate the 2D digital aesthetic preview of your smile?
- On a scale from 0 to 10, how would you rate the 3D digital aesthetic preview of your smile?
-
Based on the previews, how satisfied are you with the proposed aesthetic outcome so far?☐ Very satisfied☐ Fairly satisfied☐ Slightly satisfied☐ Not at all satisfied
- After reviewing the mock-up, how well did the tooth shape meet your expectations? (0 = not at all, 10 = perfectly)
- How well did the tooth color match your expectations? (0 = not at all, 10 = perfectly)
-
Do you feel that the use of digital software improved communication between you and your dentist?☐ Yes☐ No
- On a scale from 0 to 10, how satisfied are you with the final aesthetic result?
- On a scale from 0 to 10, how satisfied are you with the final functional result?
-
To what extent did the final results meet your expectations?☐ Fully☐ Mostly☐ Partially☐ Not at all
- Overall, how much do you like your smile now? (0 = not at all, 10 = completely)
2.6. Statistical Analysis
Data were recorded in a Microsoft Excel spreadsheet. The mean and standard deviation were calculated for each variable. Differences between pre- and post-treatment values were assessed using a paired t-test, with each patient serving as the statistical unit. All statistical analyses were performed with a significance level set at 0.05.
3. Results
Five adult patients, previously treated with clear aligners (Invisalign, Align Technology) and feldspathic veneers, were asked to complete the questionnaire and were included in this study. The mean age was 26.6 years. Four out of five patients were female, and none of the patients were smokers. All required minimally invasive prosthetic treatment for esthetic reasons. In addition, following esthetic and functional evaluations, all patients agreed to undergo aligner therapy prior to prosthetic restorations. All interviewed patients expressed a desire for a natural-looking smile. Four out of five preferred a natural tooth color, while one female patient requested a brighter, whiter shade. When asked to rate their smile esthetics and function on a scale from 0 to 10 before treatment, the mean values were 4.8 (range: 4 to 6) and 6.6 (range: 5 to 8), respectively. After reviewing the pre-visualization of the newly designed smile in both 2D and 4K video formats, patients rated the esthetic outcomes with a mean score of 7.8 for the 2D preview and 9.2 for the 4K video. Following the digital pre-visualization, all patients declared complete satisfaction with the proposed result. Similarly, after mock-up application, the mean self-reported scores were 9.4 for tooth shape and 9.2 for color. All patients agreed that digital technologies were very helpful in understanding the upcoming treatment steps, and most reported that their initial expectations were completely met. The average total treatment time, including aligner therapy, was 11.6 months. When patients were asked again to rate their smile esthetics and function following the full treatment, the mean scores were 9.8 (range: 9 to 10) for esthetics and 9.4 (range: 8 to 10) for function. The improvements from baseline were statistically significant: 5.0 points for esthetics (P = 0.001) and 2.8 points for function (P = 0.002). All patients reported complete satisfaction with the outcome, with a mean overall satisfaction score of 9.8.
4. Discussion
This study aimed to evaluate patients’ perceptions of smile aesthetics and function before and after an interdisciplinary, digitally planned treatment involving clear aligners and minimally invasive ceramic veneers. The findings highlight a significant improvement in both self-perceived smile aesthetics and oral function, with patients reporting high satisfaction post-treatment. The use of pre-visualization tools, particularly AI-powered video previews, was considered instrumental in setting realistic expectations and improving patient understanding and acceptance of the treatment plan.
The digital tools employed—especially exocad’s Smile Creator and TruSmile—leveraged artificial intelligence to simulate a dynamic, realistic version of the patient’s future smile [11,12]. This 4K video-based preview allowed patients to visualize the functional and emotional expression of their anticipated outcome, enhancing confidence in the proposed treatment. Patients rated the AI-generated preview higher (mean: 9.2/10) than static 2D designs (mean: 7.8/10), reinforcing the added value of advanced simulation technologies in aesthetic dentistry. These tools enabled more accurate interdisciplinary planning and fostered improved communication between dentist and patient, consistent with previous findings by Coachman & Paravina [6] and Cervino & co-authors [8].
Statistically significant improvements were observed in both aesthetic (mean difference: +5.0, p = 0.001) and functional outcomes (mean difference: +2.8, p = 0.002). These results support the role of clear aligner therapy not only in orthodontic correction but also in optimizing the pre-prosthetic condition of teeth. Pre-restorative orthodontic movements created space and alignment that allowed for conservative tooth preparation—an outcome aligned with recent studies emphasizing minimally invasive protocols [4,9].
All patients received feldspathic veneers following orthodontic alignment. This sequence enabled guided no-prep or minimally invasive preparations based on mock-ups derived from the digital design. Such an approach helps preserve enamel and soft tissue integrity, enhancing long-term prosthetic success [1,2]. Venezia et al. [3] also highlighted the advantages of prosthetically guided orthodontics in achieving esthetic harmony, a strategy mirrored in this study.
Importantly, all patients preferred a natural smile over a hyper-aesthetic one, echoing a broader cultural shift toward subtle enhancements [13]. Most participants indicated that the digital mock-ups and AI previews were crucial to understanding the process and visualizing the outcome, which they found to be realistic and encouraging.
This study underscored the value of integrating AI-driven visualization tools with aligner orthodontics and modern veneer techniques. As digital technology becomes increasingly precise, the ability to personalize smile designs, enhance communication, and deliver predictable esthetic and functional outcomes will define the future of aesthetic dentistry.
5. Conclusions
Patients undergoing a digitally planned, interdisciplinary approach involving clear aligners and feldspathic veneers reported high satisfaction with the final aesthetic and functional results. AI-based pre-visualization tools significantly contributed to treatment understanding and acceptance. The combination of clear aligner therapy and mock-up-guided veneer preparation allowed for minimally invasive, tissue-preserving procedures, offering predictable and natural-looking outcomes.
References
- Mihali, S. G., Lolos, D., Popa, G., Tudor, A., & Bratu, D. C. (2022). Retrospective long-term clinical outcome of feldspathic ceramic veneers. Materials (Basel), 15(6), 2150. [CrossRef]
- Morimoto, S., Albanesi, R. B., Sesma, N., Agra, C. M., & Braga, M. M. (2016). Main clinical outcomes of feldspathic porcelain and glass-ceramic laminate veneers: A systematic review and meta-analysis of survival and complication rates. The International Journal of Prosthodontics, 29(1), 38–49. [CrossRef]
- Venezia, P., Ronsivalle, V., Isola, G., Ruiz, F., Casiello, E., Leonardi, R., & Lo Giudice, A. (2022). Prosthetically guided orthodontics (PGO): A personalized clinical approach for aesthetic solutions using digital technology. Journal of Personalized Medicine, 12(10), 1716. [CrossRef]
- Korkut, B., Unal, T., Murat, N., & Özcan, M. (2025). Effect of prerestorative short-term clear aligner therapy in restorative treatment planning. The Journal of Prosthetic Dentistry, 133(2), 455–463. [CrossRef]
- Ackerman, M. B., & Ackerman, J. L. (2002). Smile analysis and design in the digital era. Journal of Clinical Orthodontics: JCO, 36(4), 221–236.
- Coachman, C., & Paravina, R. D. (2016). Digitally enhanced esthetic dentistry - From treatment planning to quality control. Journal of Esthetic and Restorative Dentistry, 28(Suppl 1), S3–S4. [CrossRef]
- Cooper, L. F., Culp, L., & Luedin, N. (2016). A digital approach to improved overdentures for the adolescent oligodontia patient. Journal of Esthetic and Restorative Dentistry, 28(3), 144–156. [CrossRef]
- Cervino, G., Fiorillo, L., Arzukanyan, A. V., Spagnuolo, G., & Cicciù, M. (2019). Dental restorative digital workflow: Digital smile design from aesthetic to function. Dentistry Journal, 7(2), 30. [CrossRef]
- Garcia, P. P., da Costa, R. G., Calgaro, M., Ritter, A. V., Correr, G. M., da Cunha, L. F., & Gonzaga, C. C. (2018). Digital smile design and mock-up technique for esthetic treatment planning with porcelain laminate veneers. Journal of Conservative Dentistry: JCD, 21(4), 455–458. [CrossRef]
- Alshiddi, I. F., BinSaleh, S. M., & Alhawas, Y. (2015). Patient's perception on the esthetic outcome of anterior fixed prosthetic treatment. The Journal of Contemporary Dental Practice, 16(11), 845–849. [CrossRef]
- Joda, T., & Gallucci, G. O. (2015). The virtual patient in dental medicine. Clinical Oral Implants Research, 26(6), 725–726. [CrossRef]
- Mangano, F. G., Gandolfi, A., Luongo, G., & Logozzo, S. (2020). Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health, 20, 1–11. [CrossRef]
- Zarone, F., Russo, S., Sorrentino, R., Ferrari, M., & Morgano, S. M. (2021). Minimally invasive approaches for anterior teeth restoration: Clinical guidelines. The International Journal of Esthetic Dentistry, 16(4), 408–422.
Figure 1.
Initial situation. Intra-oral frontal picture in occlusion.

Figure 2.
Initial situation. Intra-oral frontal picture, maxillary teeth.
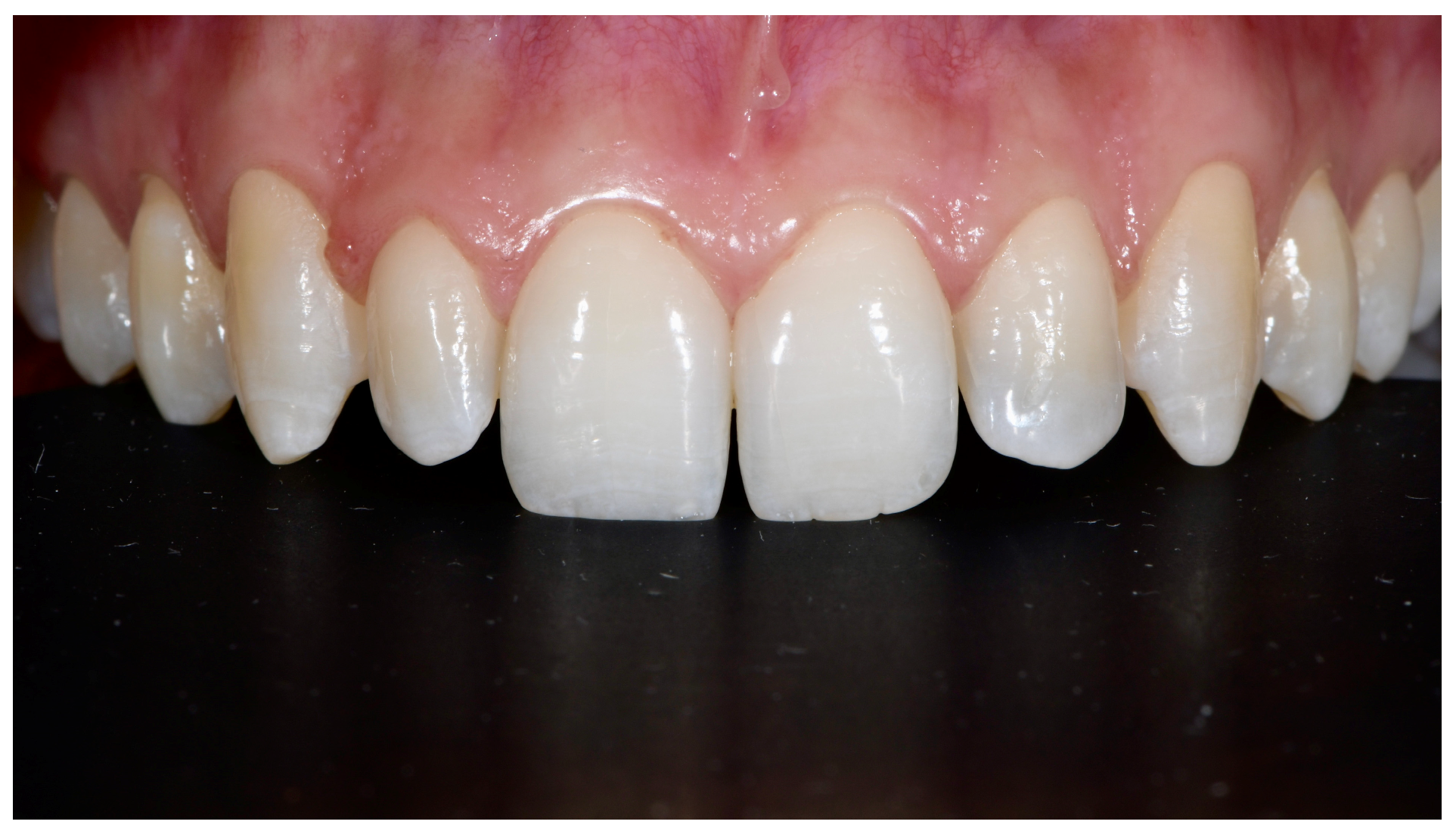
Figure 3.
Initial situation. Extra-oral frontal picture with smile.

Figure 4.
Initial situation. Extra-oral frontal picture with retractor.

Figure 5.
Pre-visualization with Smile Creator (exocad Elefsina 3.2, Smile Creator, exocad GmbH).

Figure 6.
Pre-visualization with TruSmile (exocad Elefsina 3.2, Smile Creator, exocad GmbH).

Figure 7.
ClinCheck® (Align Technology, Inc., San Jose, CA, USA) with the comparison between the pre-treatment condition (A) and the final digital plan (B) with the recovery of ideal space distribution (green box) and tooth inclination in the maxillary arch.
Figure 7.
ClinCheck® (Align Technology, Inc., San Jose, CA, USA) with the comparison between the pre-treatment condition (A) and the final digital plan (B) with the recovery of ideal space distribution (green box) and tooth inclination in the maxillary arch.
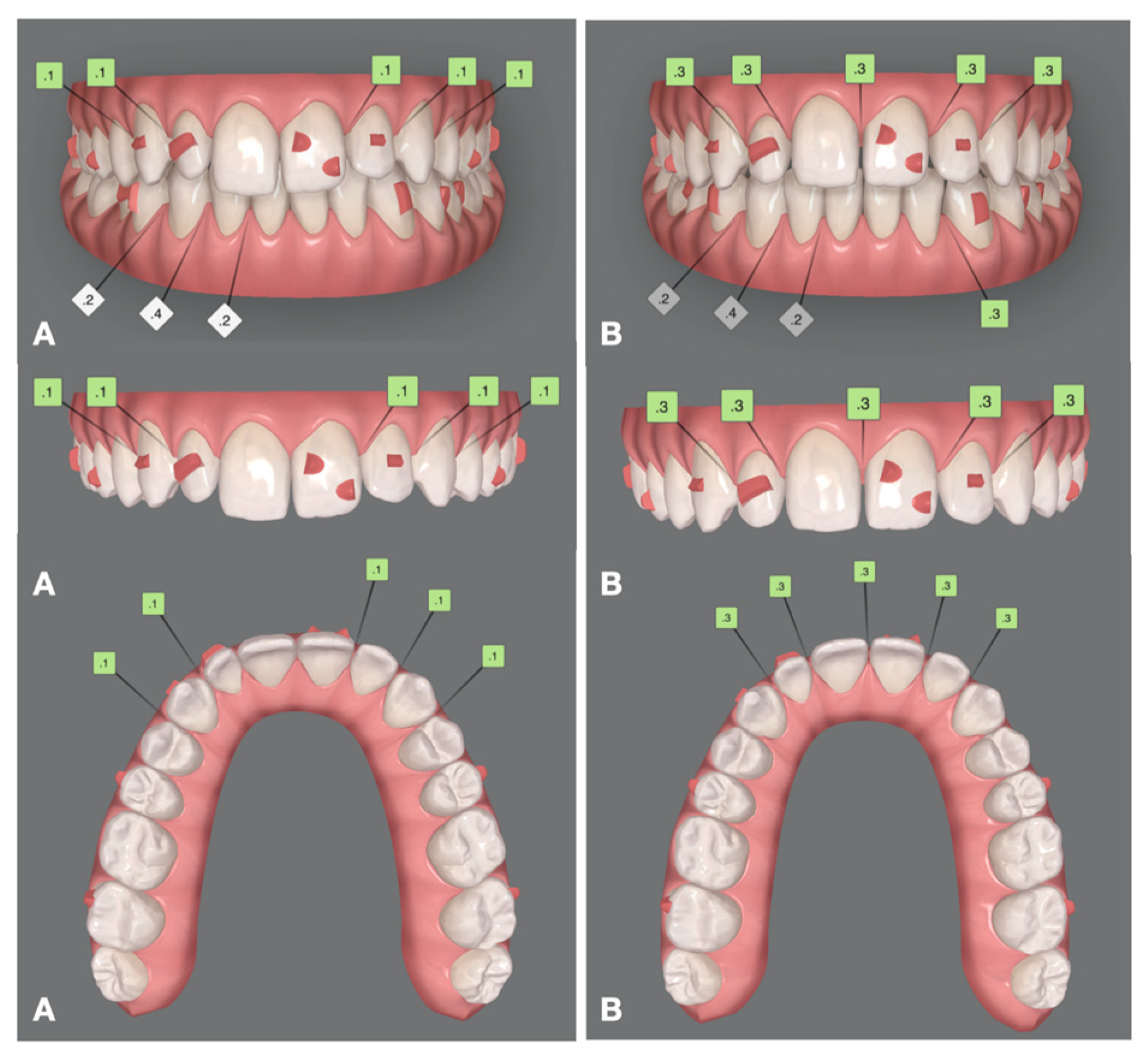
Figure 8.
Mock-up: preparation using acrylic resin and silicone mask.

Figure 9.
Mock-up: smile view.

Figure 10.
Minimally invasive preparations for feldspathic veneers.

Figure 11.
Feldspathic veneers two weeks after adhesive cementation.

Figure 12.
Extra-oral picture. Patient’s smile.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



