
Submitted:
25 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
The burden of scabies in Far North Queensland (FNQ), tropical Australia is incompletely defined. We reviewed the results of every skin scraping collected in FNQ’s public health system between 2000 and 2023; 121/4345 (2.8%) were positive, including 19/1071 (1.8%) in the last 5 years of the study; the proportion of tests that were positive for scabies declined over the study period (rs=-0.62, p=0.0001) Individuals who tested positive for scabies were no more likely to have had a prior diagnosis of ARF or RHD compared to matched controls (1/101 (1%) versus 3/101 (3%); OR (95% CI): 0.32 (0.03–3.20), p=0.33). During a median (IQR) of 14.7 (6.6-20.1) years of follow up, individuals who tested positive for scabies were also no more likely to have a diagnosis of ARF or RHD than matched controls (2/100 (2%) versus 6/98 (6%); hazard ratio (HR) (95% CI): 0.30 (0.06-1.50) p=0.14). We reviewed all 292 individuals diagnosed with scabies in the Cairns Hospital Emergency Department between March 2016 and May 2024. Skin scrapings were performed in 14/292 (4.5%); only 1/14 was positive for scabies. Microbiologically confirmed scabies is uncommon in FNQ and appears to make a limited contribution to the local incidence of ARF and RHD.
Keywords:
Scabies
; Acute rheumatic fever
; Rheumatic heart disease
; Chronic kidney disease
; Social determinants of health
; Aboriginal and Torres Strait Islander Australian Health
; Tropical Medicine
1. Introduction
Scabies, an ectoparasitic skin infestation caused by the mite Sarcoptes scabiei var hominis, affects more than 200 million people globally.[1] It primarily occurs in disadvantaged populations, is more common in tropical regions and was defined as a Neglected Tropical Disease by the World Health Organisation in 2017.[2,3,4] In Australia, scabies disproportionately affects Aboriginal communities in the tropical north of the country.[2,5]
Infestation with scabies mites results in a pruritic rash that can profoundly affect quality of life. The rash can impair sleep, affect an individual’s ability to work, and lead to stigmatisation and embarrassment.[6,7,8] Scabies also predisposes to secondary bacterial infection, often by Staphylococcus aureus or Streptococcus pyogenes, that can result in life-threatening sepsis.[5,9,10] Additional sequelae of S. pyogenes infection include acute rheumatic fever (ARF) and rheumatic heart disease (RHD), and post-streptococcal glomerulonephritis (PSGN).[11,12,13] The rates of ARF and RHD in Aboriginal and Torres Strait Islander Australians (hereafter respectfully referred to, collectively, as First Nations Australians) are amongst the highest recorded in the world.[14] Meanwhile, PSGN is increasingly recognised as a risk factor for chronic kidney disease (CKD).[15,16] RHD and CKD are both important causes of premature morbidity and mortality in First Nations Australians in tropical Australia.[14,17]
In classic scabies, the most common manifestation of scabies, individuals have fewer than 20 mites, and the most prominent symptom is pruritus.[18] A severe form of scabies, crusted scabies, is characterised by hyper-infestation with millions of mites and the formation of hyperkeratotic crusts.[19] Crusted scabies is associated with a much higher rate of complications than classic scabies, is far more contagious and therefore has significant public health implications.[20,21]
Early recognition and treatment of scabies improves quality of life and would also be expected to reduce the incidence of secondary bacterial skin infections and their sequelae. Indeed, scabies recognition and treatment has been incorporated into guidelines and programmes for the management of ARF/RHD and PSGN.[22,23,24,25] Identifying and treating scabies is an attractive public health intervention as treating individual cases is relatively simple. Both topical (permethrin) and oral (ivermectin) medications are available, effective, and generally well tolerated.[26] However, due to challenges of timely treatment of household contacts, and the resulting high rates if reinfection, scabies remains endemic in many First Nations communities in tropical Australia.[1,27]
The majority of Australian research into scabies occurs in the Northern Territory (NT), where guidelines for both individual cases and public health strategies have been developed.[28,29,30] There is interest in applying these strategies elsewhere in the nation, particularly in First Nations communities. One of these regions is FNQ in the tropical northeast of the country, where 17% of the population identify as First Nations Australians.[31] The FNQ region has a significant burden of skin infection, ARF/RHD and CKD, and has three of the seven most disadvantaged Local Government Areas in Australia.[32,33,34,35] Given the similar demographics, the similar climate, and similar impact of the social determinants of health, it might be expected that there is a similar incidence of scabies and crusted scabies in FNQ to that seen in the NT.
However, the anecdotal experience of physicians who have worked across Northern Australia is that the prevalence and severity of scabies appears to be lower in FNQ than the NT. If true, some interventions proposed in the NT, such as mass drug administration, may have a limited impact in FNQ. Public health strategies that address access to care, health literacy and housing adequacy may represent higher value interventions to reduce the local burden of ARF/RHD and CKD.[14,17,36]
This study was therefore conducted to define the temporospatial epidemiology of scabies infestation in FNQ. It also evaluated whether individuals with confirmed scabies had a higher risk of subsequently developing ARF, RHD and renal impairment. Finally, it examined whether the practice of local clinicians who were assessing individuals at risk of scabies was in accordance with contemporary published guidelines. It was hoped that the data collected would help inform strategies to improve the skin health of people living in the FNQ region, reduce the local incidence of RHD and PSGN, and to optimise the use of finite health resources.
2. Methods
2.1. Study Design and Population
This retrospective study was performed at Cairns Hospital, the 581-bed tertiary referral hospital for the FNQ region of tropical Australia (Figure 1). The hospital serves a population of approximately 290,000 people who live across an area of 380,000 km2.[31] There are two health services in the region, the Cairns and Hinterland Hospital and Health Service (CHHHS) ‒ which serves the population of the administrative hub of Cairns and the surrounding region ‒ and the Torres and Cape Hospital and Health Service (TCHHS), which serves the almost exclusively rural and remote population living on the Cape York Peninsula and the Torres Strait Islands.
2.2. Identification of Individuals with a Positive Skin Scraping in the FNQ Region Between 2000 and 2023
The Cairns Hospital laboratory is the referral laboratory for all microbiology services in the public health system in the FNQ region and the sole facility that performs microscopy of skin scrapings. All laboratory results collected in the state of Queensland’s public health system are entered into the electronic database AUSLAB. The AUSLAB database was interrogated to identify all skin scraping requests processed in the Cairns Hospital laboratory between 1st January 2000 and 31st December 2023.
The patients’ demographics and the date and location of the request were recorded. Tests that were not performed on skin were removed, as were tests where microscopy could not be performed. Duplicate tests (performed on the same individual within 30 days) were also removed; if any duplicate tests within the 30-day period were positive for scabies mites, eggs or faecal pellets, this was defined as a positive episode. If all of these duplicate tests were negative, this was defined as a negative episode. All individuals receiving care in Queensland’s public health system are asked whether they identify as a First Nations Australian. Individuals aged 15 years and younger were defined as children. Individuals tested in Cairns were said to have had testing in an urban location; those tested outside of Cairns were said to have had testing in a rural or remote location.
2.3. The Association Between a Positive Skin Scraping and Subsequent Diagnosis of ARF/RHD or CKD
A list of the individuals that had a positive skin scraping for scabies between 2000 and 2023 was generated and a corresponding list of controls (matched to age, sex, location, and First Nations Australian status) who tested negative was selected manually. The date that the scraping was performed was also matched (+/- 2 years) to ensure there was a similar duration of follow-up. ARF and RHD have been notifiable diseases in the state of Queensland since 1998 and 2018, respectively. The Queensland Rheumatic Heart Disease register was interrogated to determine if these individuals had been notified to the register for either ARF or RHD, and, if they had been, the date of their first notification. The individuals’ most recent formal estimated glomerular filtration rate (eGFR) was also identified through the AUSLAB system. CKD was defined as an eGFR <60mL/min/1.73m2.[37] Patients who had a diagnosis of ARF/RHD or CKD preceding their skin scraping were excluded from the respective analyses.
2.4. Assessment of Individuals Presenting to the Cairns Hospital Emergency Department with a Diagnosis of Scabies
Patients presenting to the Cairns Hospital Emergency Department who had an ICD-10 coded diagnosis of scabies were identified with the Emergency Department’s electronic health record system, FirstNet (Oracle Health, version 19.19, Microsoft, Kansas City, MO, USA) This system was established in Cairns Hospital in March 2016. All presentations that were coded with a diagnosis of scabies between 1st March 2016 to 31st May 2024 were identified; representations within 30 days were excluded. Each patient was cross-referenced with AUSLAB to determine if skin scrapings were collected in the public health system 30 days before or after their presentation. The patients’ medical records were reviewed, and demographic and relevant clinical data were recorded. The diagnostic approach of the attending clinicians was recorded to determine if this was in accordance with IACS guidelines (Supplementary Table S1), and if the assessment of possible cases of crusted scabies followed NT guidelines.[29]
2.5. Statistical Analysis
Data were de-identified, entered into an electronic database (Microsoft Excel version 16.0, Microsoft, Redmond, WA, USA) and analysed using statistical software (Stata version 18.0, StataCorp LLC., College Station, TX, USA). Trends over time were analysed using Spearman’s test for correlation. Groups were compared using logistic regression, the chi-squared or Fisher’s exact test, as appropriate. Multivariate analysis was performed using logistic regression with variables selected for the multivariate model if their p-value in univariate analyses was <0.10. The subsequent incidence of ARF/RHD or an eGFR <60mL/min/1.73m2 in individuals who with positive skin scrapings and matched controls were analysed using a Cox proportional hazards model and presented using Kaplan–Meier curves. If individuals were missing data, they were not included in analyses which evaluated those variables.
2.6. Ethics Statement
The Far North Queensland Human Research Ethics Committee provided ethical approval for the study (EX/2023/QCH/102367). As the retrospective data were de-identified and presented in an aggregated manner, the Committee waived the requirement for informed consent.
3. Results
3.1. Skin Scrapings
Review of the AUSLAB electronic laboratory database identified 6199 episodes recorded as skin scrapings. After excluding duplicates and non-skin samples, there were a total of 4345 distinct testing episodes that were included in the analysis (Supplementary Figure S1).
3.2. Characteristics of the Individuals Who Were Tested
From 2000 to 2023, there was a median of 188 annual skin scraping episodes (interquartile range (IQR): 162-224). The number of annual episodes increased during the study period (rs=0.64, p=0.001) (Figure 2). The median age of patients having skin scrapings taken was 42 years (IQR 23-58, range 0-100) and 790/4345 (18%) were children. Of the 4342 episodes where the location of testing was available, 3397 (78%) scrapings were collected in rural or remote locations. Of the 4314 episodes where First Nations Australian status was available, in 2707 (63%) episodes the individuals identified as a First Nations Australian.
3.3. Number of Positive Tests and Trend Over Time
Scabies was diagnosed in 121/4345 (2.8%) skin scraping episodes. The 121 diagnoses of scabies occurred in 101 individuals. The proportion of tests that were positive for scabies declined over the study period (rs=-0.62, p=0.0001) (Figure 3). Indeed, scabies was diagnosed in only 19/1071 (1.8%) scrapings in the last 5 years of the study. In multivariate analysis, positive tests were more common in First Nations Australians, in adults, and in individuals tested in an urban location (Table 1).
3.4. Association of Microbiologically Diagnosed Scabies with a Subsequent Diagnosis of ARF/RHD or CKD
Individuals who tested positive for scabies were no more likely to have had a prior diagnosis of ARF or RHD compared to matched controls (1/101 (1%) versus 3/101 (3%); OR (95% CI): 0.32 (0.03 – 3.20), p=0.33). Furthermore, during a median (IQR) of 14.7 (6.6-20.1) years of follow up, individuals who tested positive for scabies were also no more likely to have a diagnosis of ARF or RHD than matched controls (2/100 (2%) versus 6/98 (6%); hazard ratio (HR) (95% CI): 0.30 (0.06-1.50) p=0.14). (Figure 4 and Supplementary Figure S2).
There were 168/202 (83%) individuals with skin scrapings who had an available eGFR; in 154/168 (92%) this was greater than 30 days after the skin scraping. Individuals who tested positive for scabies were not at an increased risk of having a GFR <60mL/min/1.73m2 during follow-up than matched controls (43/70 (61%) versus 40/84 (48%); HR (95% CI) 1.39 (0.90-2.14), p=0.13.) (Figure 5 and Supplementary Figure S3).
3.5. Assessment of Individuals Presenting to the Cairns Hospital Emergency Department with Clinically Suspected Scabies
There were 353 presentations to Cairns Hospital Emergency Department coded as a presentation of scabies. After representations within 30 days, and individuals who were subsequently confirmed to have and alternative diagnosis were removed, 292 presentations in 265 individuals were included in this analysis; 21/292 (7.2%) had a clinical suspicion of crusted scabies.
3.5.1. Classic Scabies
Only 9/271 (3.3%) with clinical suspicion for classic scabies had skin scrapings performed, none of which were positive for scabies (Table 2 and Supplementary Figure S4). Only 86/271 (31.7%) were reviewed by a specialist of any specialty (including emergency) during their hospital encounter. There was no documented use of dermatoscopy or high-powered imaging in any of the cases. The medical records of only 11/271 (4.1%) contained documentation to suggest that the clinicians involved had addressed all the IACS criteria for a diagnosis of scabies (Supplementary Table S1). However, recognising that not all IACS criteria need to be addressed in order to satisfy the diagnostic criteria for “clinical scabies”, 88/271 (32.4%) cases had sufficient recorded data to suggest the diagnosis. There was no discernible change in the documentation of clinical findings, nor the performance of skin scrapings, after March 2020 when the IACS criteria for the diagnosis of scabies were published.[38]
3.5.2. Crusted Scabies
Only 5/21 (23.8%) of cases where crusted scabies was considered had skin scrapings collected, of which only 1/5 (20%) was positive (Table 2 and Supplementary Figure S4). The medical records of only 4/21 (19%) cases contained documentation to suggest that the clinicians had addressed all aspects of the IACS criteria for the diagnosis of scabies (Supplementary Table S1). Overall, there were 13/21 (61.9%) cases of suspected crusted scabies who satisfied the IACS criteria for a diagnosis of clinical scabies. Only 14/21 (66.7%) were reviewed by a specialist of any specialty (including emergency) during their hospital encounter, and only 6/21 (28.6%) had review by the dermatology or infectious diseases services; two of these (both seen by dermatology) were the only two cases that had a severity grading assessment and one of these cases (seen by dermatology) was the only case that had dermatoscopy documented.[39] There was only 1/21 (4.7%) of suspected cases that satisfied the NT guidelines criteria for confirmed crusted scabies. There was only one case (not the confirmed case), that had a complete initial evaluation in accordance with the NT guidelines.
Only 16/21 (76%) of individuals with suspected crusted scabies were admitted to hospital and their hospitalisations were only for a median (IQR) of 3 (3-5) days. Only 16/21 (76%) received any ivermectin, although this was sometimes in the setting of concerns about the age of a paediatric patient. The median (IQR) number of ivermectin doses was 5 (3-5) doses, but only 3/21 received keratinolytic therapy and documentation about environmental control and treatment of family members was present in 9/21 (43%) and 10/21 (48%), respectively.
4. Discussion
This study of scabies in the FNQ region of tropical Australia had three main findings. The first was that less than 3% of skin scrapings within FNQ public health system between 2000 and 2023 were positive for scabies, and that the proportion of positive tests declined over this period. Indeed, despite an increasing annual collection of skin scrapings, there were fewer than 20 microbiologically confirmed cases of scabies in over a thousand episodes of testing in the last five years of the study. Secondly, despite a significant local burden of ARF/RHD and CKD, the individuals who tested positive for scabies were no more likely to subsequently develop ARF/RHD or renal impairment than matched controls who tested negative, suggesting a limited contribution of scabies infection to the development of these complications in the FNQ region. Thirdly, the diagnostic assessment of individuals presenting to the region’s tertiary referral hospital with a possible diagnosis of scabies, was frequently suboptimal, particularly in those with a possible diagnosis of crusted scabies. Clinical suspicion was rarely confirmed microbiologically, even when there was concern for crusted scabies. Other elements of the recommended clinical assessment and management of a patient with suspected scabies were also documented poorly, suggesting the need for a reassessment of current clinical practice in the Cairns Hospital Emergency Department, and, potentially, the FNQ region more broadly. Greater adherence to contemporary diagnostic approaches will help define the true burden of scabies in the region and the implications for local clinical practice and public health strategies.
First Nations Australians accounted for over 90% of the microbiologically confirmed cases of scabies in the region despite accounting for only 17% of the local population, which is consistent with the epidemiology of scabies reported from other Australian jurisdictions.[2,5] However, in contrast to other Australian studies, a confirmed diagnosis of scabies was, in multivariate analysis, over six times less likely in rural and remote communities in this study. This does not appear to be wholly explained by lower testing rates in rural and remote locations, as more than half of the skin scrapings were collected in remote communities in the Torres Strait and Cape York region, where less than 10% of FNQ’s population resides. A microbiologically confirmed diagnosis of scabies was also almost six times less common in children. This was surprising as scabies is consistently reported in the literature to be more prevalent in children, to the extent that monitoring scabies in children has been proposed as the most effective method to track prevalence and detect outbreaks.[2,4,28,41] While this finding might be partly explained by clinicians’ reluctance to perform potentially distressing skin scrapings in children, over 18% of the skin scrapings in our cohort were performed in individuals aged <16 years of age (less than 1% of which were positive, compared to >3% in adults), while 13% of the FNQ population is aged <20 years of age.[31] The fact that skin scrapings were performed in a variety of geographic settings and across the full age-range, suggests that there are no systemic barriers to performing this test.
Instead, it appears that local clinicians have a greater inclination to diagnose scabies clinically. This is supported by the finding that less than 5% of individuals seen in the emergency department with suspected scabies – and less than a quarter with suspected crusted scabies – had skin scrapings collected. There was also only a single case where the use of high-powered imaging or dermatoscopy was documented. The availability, efficacy and ease of use of ivermectin likely reduces the impetus for busy clinicians to perform confirmatory testing.[42] But without confirmatory testing there is a risk of bias informing the clinical diagnosis of scabies, particularly in populations believed to at greater risk.[43] The clinical diagnosis of scabies is challenging, relies heavily on the experience of the clinician and its accuracy is difficult to verify.[44,45] Even after dedicated training healthcare professionals have difficulty in identifying cases.[46] Many of the individuals with suspected scabies in this cohort were only seen by junior clinicians – with little to no training in the diagnosis of scabies – casting some doubt as to the accuracy of their clinical assessment. Although the documentation was often incomplete and the medical charts were reviewed retrospectively, only about 35% of the individuals in our cohort with a diagnosis of scabies in the Emergency Department satisfied IACS criteria for a diagnosis of clinical scabies. While scabies is under-recognised globally, in endemic or presumed-endemic regions overdiagnosis and overtreatment is also seen.[47,48] The limited documentation of the clinicians’ assessment seen in this cohort of may reflect documentation practices in a busy emergency department, a manifestation of the recognised phenomenon of the trivialisation of skin conditions, or further evidence of limited familiarity with scabies among the local health worker population.[47,49]
The very low rate of confirmed scabies in FNQ is consistent with anecdotal observations of local clinicians that have worked across tropical Australia, who believe there may be a lower burden of scabies in FNQ. However, there are data that challenges this view. A public health response to an outbreak of 2021 outbreak of PSGN in Aurukun, a remote Aboriginal community in Cape York, identified a scabies rate of 21% of the total population screened, and of 26% in the subgroup of screened children, rates that are comparable to the high rates seen in Top End Communities in NT.[2,5,41,50] However, none of the diagnoses were confirmed with laboratory testing, and the staff conducting clinical assessments had limited experience and training in diagnosing scabies (Neville, J 2023, oral communication, 19 May 2023). The association with a PSGN outbreak may have increased the risk of confirmation bias.[43]
Our study does provide data that crusted scabies is far less common in FNQ than other parts of tropical Australia. Crusted scabies has been a notifiable disease in the NT since 2016 and notified cases in that jurisdiction must satisfy both strict laboratory and clinical criteria, including positive skin scrapings and confirmation by either a dermatologist or infectious diseases specialist. There were 210 cases of crusted scabies between March 2016 and July 2023, in NT’s Top End Region, which has a population of approximately 200,000.[51] Crusted scabies is not a notifiable condition in QLD, but during the same March 2016 to July 2023 period there were only 31 laboratory confirmed cases of any – not just crusted – scabies in the FNQ public health system which serves a population of approximately 290,000.[52]
Of course, this may again be at least partly explained by inadequate testing, and it is concerning that over three-quarters of the individuals with a clinical diagnosis of crusted scabies presenting to the Cairns Hospital Emergency Department did not have confirmatory laboratory testing. Laboratory confirmation of crusted scabies is important as the condition is associated with a higher rate of complications – including life threatening sepsis – and up to 25% of individuals diagnosed with crusted scabies will die within 12-months.[21,40,53] A diagnosis of crusted scabies also has significant public health implications due to its contagiousness, as patients with crusted scabies have been identified as the index-case in outbreaks.[27,54] Conversely, the appearance of crusted scabies can also be non-specific and may mimic other diagnoses, some of which can be life-threatening, that require different management.[38] Millions of mites may be present in a patient with crusted scabies so correctly collected skin scrapings, therefore effectively exclude the diagnosis if they are negative.[19,55] NT guidelines also recommend dermatologist or infectious diseases specialist involvement, an assessment of severity, and admission to hospital.[40] However, a minority of the cases in this FNQ series had specialist review, very few had a complete assessment documented and almost a quarter were not admitted to hospital. Those that were rarely received keratinolytic therapy and the minority had documentation about environmental control or treatment of family members. This suggests that FNQ clinicians are unfamiliar with the recommended management of a patient with possible crusted scabies, which may, in turn, be at least partially explained by a lower incidence of crusted scabies in the region.
It has been suggested that earlier identification and treatment of scabies will reduce the risk of subsequent infection with S. pyogenes and therefore reduce the risk of ARF/RHD and CKD.[3] However, our study provides little evidence to support the suggestion that scabies contributes significantly to the development of either ARF/RHD or CKD in the FNQ region. The incidence of laboratory-confirmed scabies was very low in our cohort and there was no significant difference in the development of CKD or ARF/RHD in FNQ between laboratory-confirmed cases and matched controls. It is likely that the high prevalence of CKD in the FNQ region is more strongly linked to traditional risk factors, particularly diabetes.[56,57,58] While ARF and RHD, like scabies, are strongly linked to the social determinants of health, the FNQ region with the highest prevalence of RHD had only two confirmed cases of scabies in the 24 years of our study.[33,59]
Our study systematically evaluates laboratory data collected over 24 years, and over 8 years of hospital presentation data to provide a temporospatial estimate of the burden of scabies in the FNQ region. The study also allows a critical appraisal of local clinical practice. However, it also has many limitations. Our finding that skin scrapings were performed in fewer than 5% of presentations with a diagnosis of scabies may also, almost certainly, underestimate the local disease incidence. The sensitivity of skin scrapings in cases of non-crusted scabies has been reported to be less than 50% and the collection of adequate scrapings is operator dependent.[1,38,60,61] However, these factors need to be balanced against the fact that there were less than 20 cases of confirmed scabies across in the public health system across the whole FNQ region in the last 5 years of the study. Only scrapings collected in the public health system were reviewed, although testing for scabies is infrequently performed in private laboratories in the region and is unlikely to have had a significant impact on the overall results or conclusions of this study. It was not possible to determine the indication for the skin scrapings, and the low and declining proportion of cases may be at least partially explained by an increasing number of scrapings being conducted for other indications – for instance, dermatophyte infection – although these conditions are also often treated empirically. A very low incidence of crusted scabies does not necessarily mean a lower incidence of all scabies infection: programmes that have conducted whole population screening have reported on the absence of even a single case of crusted scabies, despite an overall prevalence of scabies up to 18.7%.[62,63] There are well recognised, inherent limitations in using clinical coding to identify patients with specific health conditions.[64,65] On review of the medical records, over 10% of the presentations to the Cairns Hospital Emergency coded as scabies had another diagnosis confirmed or simply no evidence of scabies (Supplementary Table S3). The study’s retrospective design and reliance on documentation in the medical record precluded the collection of comprehensive clinical data. The evaluation of the association between a laboratory diagnosis of scabies and the subsequent development of ARF/RDH or CKD did not consider the contribution of potential confounding factors.
Acknowledging these limitations, and recognising that it is likely that there is both under- and overdiagnosis of scabies in FNQ, our data support experienced clinicians’ impression that the local incidence of scabies is far lower than in other regions of tropical Australia. Future prospective studies that utilise standardised clinical assessment, as well as routine use of skin-scrapings, dermatoscopy and evolving molecular techniques will better quantify the prevalence of scabies across FNQ and the implications for local public health strategies.[38,66,67] This will also facilitate optimal management of patients with both scabies and other dermatological conditions.[68,69] Making crusted scabies a notifiable condition in Queensland, as it is in the NT, would also ensure appropriate patient evaluation and management, as well as more reliable tracking of cases, reducing the risk of ongoing transmission and minimising the likelihood of outbreaks.[27,54]
5. Conclusions
Microbiologically confirmed scabies infection is rare in the FNQ region and, despite an increase in local testing, the incidence of microbiologically confirmed cases is declining. FNQ individuals who have positive skin scrapings for scabies are no more likely to subsequently develop ARF/RHD or CKD than those with negative tests. The incidence of crusted scabies in the FNQ appears to be considerably lower than in other regions in tropical Australia. Most cases of scabies in the region are diagnosed clinically, even when crusted disease is suspected, although the evaluation of patients frequently does not follow contemporary guidelines for disease assessment and management.
Despite this, there are limited data to suggest that there is a major burden of scabies in the region. The social determinants of health have an important impact on the incidence of communicable and non-communicable diseases in FNQ and, importantly, also increase the risk of scabies emerging as an important local health issue. While scabies recognition and treatment has been incorporated into guidelines and programmes for the management of ARF/RHD and PSGN in other parts of Australia and mass drug administration has been implemented in some communities,[22,23,24,25,28] in FNQ a greater focus on strategies that address the ongoing socioeconomic disadvantage in the region are likely to be a better use of finite local health resources.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org
References
- Walton SF, Currie BJ. Problems in diagnosing scabies, a global disease in human and animal populations. Clinical microbiology reviews. 2007;20(2):268-79. [CrossRef]
- Romani L, Steer AC, Whitfeld MJ, Kaldor JM. Prevalence of scabies and impetigo worldwide: A systematic review. The Lancet Infectious Diseases. 2015;15(8):960-7. [CrossRef]
- Scabies Geneva: World Heath Organization; 2023 [updated 31 May 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/scabies.
- Li J, Liu Z, Xia X. The disability-adjusted life years (DALYs), prevalence and incidence of scabies, 1990–2021: A systematic analysis from the Global Burden of Disease Study 2021. PLOS Neglected Tropical Diseases. 2024;18(12):e0012775.
- Davidson L, Knight J, Bowen AC. Skin infections in Australian Aboriginal children: a narrative review. The Medical journal of Australia. 2020;212(5):231-7. [CrossRef]
- Lake SJ, Engelman D, Sokana O, Nasi T, Boara D, Marks M, et al. Health-related quality of life impact of scabies in the Solomon Islands. Trans R Soc Trop Med Hyg. 2022;116(2):148-56. [CrossRef]
- Collinson S, Timothy J, Zayzay SK, Kollie KK, Lebas E, Candy N, et al. The prevalence of scabies in Monrovia, Liberia: A population-based survey. PLoS neglected tropical diseases. 2020;14(12):e0008943. [CrossRef]
- Nair PA, Vora RV, Jivani NB, Gandhi SS. A Study of Clinical Profile and Quality of Life in Patients with Scabies at a Rural Tertiary Care Centre. J Clin Diagn Res. 2016;10(10):Wc01-wc5.
- Steer AC, Jenney AWJ, Kado J, Batzloff MR, La Vincente S, Waqatakirewa L, et al. High burden of impetigo and scabies in a tropical country. PLoS Neglected Tropical Diseases. 2009;3(6). [CrossRef]
- Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG, Jr. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603-61.
- Parks T, Smeesters PR, Steer AC. Streptococcal skin infection and rheumatic heart disease. Curr Opin Infect Dis. 2012;25(2):145-53. [CrossRef]
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5(11):685-94.
- Dowler J, Wilson A. Acute post-streptococcal glomerulonephritis in Central Australia. The Australian journal of rural health. 2020;28(1):74-80. [CrossRef]
- Acute rheumatic fever and rheumatic heart disease in Australia, 2022. Canberra: AIHW; 2024.
- Hoy WE, White AV, Dowling A, Sharma SK, Bloomfield H, Tipiloura BT, et al. Post-streptococcal glomerulonephritis is a strong risk factor for chronic kidney disease in later life. Kidney international. 2012;81(10):1026-32. [CrossRef]
- Pinto SWL, Sesso R, Vasconcelos E, Watanabe YJ, Pansute AM. Follow-up of patients with epidemic poststreptococcal glomerulonephritis. American journal of kidney diseases. 2001;38(2):249-55. [CrossRef]
- Chronic kidney disease in Aboriginal and Torres Strait Islander people. Canberra: AIHW; 2011.
- Fernando DD, Mounsey KE, Bernigaud C, Surve N, Estrada Chávez GE, Hay RJ, et al. Scabies. Nature Reviews Disease Primers. 2024;10(1):74.
- Cinotti E, Perrot JL, Labeille B, Vercherin P, Chol C, Besson E, et al. Reflectance confocal microscopy for quantification of Sarcoptes scabiei in Norwegian scabies. Journal of the European Academy of Dermatology and Venereology. 2013;27(2):e176-e8. [CrossRef]
- Hasan T, Krause VL, James C, Currie BJ. Crusted scabies; a 2-year prospective study from the Northern Territory of Australia. PLoS neglected tropical diseases. 2020;14(12):e0008994. [CrossRef]
- Lynar S, Currie BJ, Baird R. Scabies and mortality. The Lancet Infectious diseases. 2017;17(12):1234.
- The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 2020 March 2022.
- Andrews RM, Kearns T, Connors C, Parker C, Carville K, Currie BJ, et al. A regional initiative to reduce skin infections amongst aboriginal children living in remote communities of the Northern Territory, Australia. PLoS neglected tropical diseases. 2009;3(11):e554. [CrossRef]
- Jones M, Thomas H, Snelling T, Bowen A, Marsh J. The SToP (See, Treat, Prevent) Skin Sores and Scabies Trial - a stepped wedge cluster randomised trial for skin disease control in remote Western Australia: Statistical analysis plan. 2023.
- Gardner K, Van Gool K, Van der Linden N, Agostino J, Campbell M, Dickinson H, et al. Evaluation of the one disease crusted scabies elimination project. Canberra: Public Service Research Group, Business School, University of New South Wales. 2018.
- Rosumeck S, Nast A, Dressler C. Ivermectin and permethrin for treating scabies. Cochrane Database Syst Rev. 2018;4(4):CD012994. [CrossRef]
- Lokuge B, Kopczynski A, Woltmann A, Alvoen F, Connors C, Guyula T, et al. Crusted scabies in remote Australia, a new way forward: lessons and outcomes from the East Arnhem Scabies Control Program. The Medical journal of Australia. 2014;200(11):644-8. [CrossRef]
- Kearns TM, Speare R, Cheng AC, McCarthy J, Carapetis JR, Holt DC, et al. Impact of an Ivermectin Mass Drug Administration on Scabies Prevalence in a Remote Australian Aboriginal Community. PLoS neglected tropical diseases. 2015;9(10):e0004151.
- Simple, Complicated and Crusted Scabies NT Health Guideline. 2024.
- Public Health Management of Crusted Scabies. NT Health. Northern Territory Government; 2023.
- 2021 Australian Census Canberra. Australian Bureau of Statistics; 2021.
- Fox H, Hempenstall A, Pilot P, Callander E, Smith S, McDonald MI, et al. Significant healthcare resource utilisation in the management of skin and soft tissue infections in the Torres Strait, Australia. Rural and remote health. 2024. [CrossRef]
- Kang K, Chau KW, Howell E, Anderson M, Smith S, Davis TJ, et al. The temporospatial epidemiology of rheumatic heart disease in Far North Queensland, tropical Australia 1997–2017; impact of socioeconomic status on disease burden, severity and access to care. PLOS Neglected Tropical Diseases. 2021;15(1):e0008990. [CrossRef]
- Vos L, Baer R, McDonald M. Addressing chronic kidney disease in F ar N orth Q ueensland: gains and opportunities. Australian Journal of Rural Health. 2013;21(6):313-8.
- Socio-Economic Indexes for Areas (SEIFA), Australia. Australian Bureau of Statistics; 2021.
- Coffey PM, Ralph AP, Krause VL. The role of social determinants of health in the risk and prevention of group A streptococcal infection, acute rheumatic fever and rheumatic heart disease: a systematic review. PLoS neglected tropical diseases. 2018;12(6):e0006577. [CrossRef]
- Stevens PE, Ahmed SB, Carrero JJ, Foster B, Francis A, Hall RK, et al. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney international. 2024;105(4):S117-S314. [CrossRef]
- Engelman D, Yoshizumi J, Hay RJ, Osti M, Micali G, Norton S, et al. The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies. The British journal of dermatology. 2020;183(5):808-20. [CrossRef]
- Davis JS, McGloughlin S, Tong SY, Walton SF, Currie BJ. A novel clinical grading scale to guide the management of crusted scabies. PLoS neglected tropical diseases. 2013;7(9):e2387. [CrossRef]
- NT Health Guideline: Simple, Complicated and Crusted Scabies. . Infectious Diseases Department, Royal Darwin Hospital. NT Health; 2024.
- Gramp P, Gramp D. Scabies in remote Aboriginal and Torres Strait Islander populations in Australia: A narrative review. PLoS neglected tropical diseases. 2021;15(9):e0009751. [CrossRef]
- Paltridge M, Smith S, Traves A, McDermott R, Fang X, Blake C, et al. Rapid Progress toward Elimination of Strongyloidiasis in North Queensland, Tropical Australia, 2000–2018. The American journal of tropical medicine and hygiene. 2020;102(2):339. [CrossRef]
- Elston DM. Confirmation bias in medical decision-making. Journal of the American Academy of Dermatology. 2020;82(3):572. [CrossRef]
- Karimkhani C, Colombara DV, Drucker AM, Norton SA, Hay R, Engelman D, et al. The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. The Lancet Infectious diseases. 2017;17(12):1247-54. [CrossRef]
- Leung V, Miller M. Detection of scabies: A systematic review of diagnostic methods. Canadian Journal of Infectious Diseases and Medical Microbiology. 2011;22(4):143-6.
- Osti MH, Sokana O, Gorae C, Whitfeld MJ, Steer AC, Engelman D. The diagnosis of scabies by non-expert examiners: A study of diagnostic accuracy. PLoS neglected tropical diseases. 2019;13(8):e0007635. [CrossRef]
- Yeoh DK, Anderson A, Cleland G, Bowen AC. Are scabies and impetigo “normalised”? A cross-sectional comparative study of hospitalised children in northern Australia assessing clinical recognition and treatment of skin infections. PLoS neglected tropical diseases. 2017;11(7):e0005726. [CrossRef]
- Felmingham C, Tilakaratne D. Overdiagnosis of scabies and overprescribing of scabies treatment in a scabies-endemic region. The Australian journal of rural health. 2020;28(4):394-8. [CrossRef]
- Lorenzetti DL, Quan H, Lucyk K, Cunningham C, Hennessy D, Jiang J, et al. Strategies for improving physician documentation in the emergency department: a systematic review. BMC Emergency Medicine. 2018;18(1):36. [CrossRef]
- Public Health Response- Aurukun- November 2021 In: Team TPH, editor.: Torres and Cape Health Service; 2023.
- Taylor G. NT Health Guideline: Public Health Management of Crusted Scabies.: Centre of Disease Control NT Health. NT Health; 2023.
- List of notifiable Conditions Queensland.: Queensland Health. Queensland Government; 2023.
- Bonazzetti C, Pagani G, Giacomelli A, Morena V, Bassoli C, Corbellino M, et al. A case of crusted scabies with a delayed diagnosis and inadequate therapy. Le Infezioni in Medicina. 2020;28(3):436-40.
- Mounsey KE, Murray HC, King M, Oprescu F. Retrospective analysis of institutional scabies outbreaks from 1984 to 2013: lessons learned and moving forward. Epidemiol Infect. 2016;144(11):2462-71. [CrossRef]
- Currie BJ, Maguire GP, Wood YK. Ivermectin and crusted (Norwegian) scabies. Medical Journal of Australia. 1995;163(10):559-60. [CrossRef]
- Hoy WE, Wang Z, Zhang J, Diwan V, Cameron A, Venuthurupalli SK, et al. Chronic kidney disease in public renal practices in Queensland, Australia, 2011–2018. Nephrology. 2022;27(12):934-44. [CrossRef]
- Kidney disease, Aboriginal and Torres Strait Islander Health Performance Framework website. Australian Institute of Health Welfare. National Indigenous Australians Agency.; 2023.
- The Health of Queenslanders. Report of the Chief Health Officer Queensland. Chronic diseases. Brisbane: Queensland Health; 2024.
- Wyber R, Noonan K, Halkon C, Enkel S, Cannon J, Haynes E, et al. Ending rheumatic heart disease in Australia: the evidence for a new approach. Medical Journal of Australia. 2020;213:S3-S31. [CrossRef]
- Shoukat Q, Rizvi A, Wahood W, Coetzee S, Wrench A. Sight the mite: a meta-analysis on the diagnosis of scabies. Cureus. 2023;15(1). [CrossRef]
- Walter B, Heukelbach J, Fengler G, Worth C, Hengge U, Feldmeier H. Comparison of dermoscopy, skin scraping, and the adhesive tape test for the diagnosis of scabies in a resource-poor setting. Arch Dermatol. 2011;147(4):468-73. [CrossRef]
- Romani L, Marks M, Sokana O, Nasi T, Kamoriki B, Cordell B, et al. Efficacy of mass drug administration with ivermectin for control of scabies and impetigo, with coadministration of azithromycin: a single-arm community intervention trial. The Lancet Infectious Diseases. 2019;19(5):510-8. [CrossRef]
- Marks M, Toloka H, Baker C, Kositz C, Asugeni J, Puiahi E, et al. Randomized Trial of Community Treatment With Azithromycin and Ivermectin Mass Drug Administration for Control of Scabies and Impetigo. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019;68(6):927-33. [CrossRef]
- Shepheard J. Clinical coding and the quality and integrity of health data. Health Information Management Journal. 2020;49(1):3-4. [CrossRef]
- O’Malley KJ, Cook KF, Price MD, Wildes KR, Hurdle JF, Ashton CM. Measuring diagnoses: ICD code accuracy. Health Serv Res. 2005;40(5 Pt 2):1620-39. [CrossRef]
- Park JH, Kim CW, Kim SS. The diagnostic accuracy of dermoscopy for scabies. Ann Dermatol. 2012;24(2):194-9. [CrossRef]
- Bae M, Kim JY, Jung J, Cha HH, Jeon N-Y, Lee H-J, et al. Diagnostic value of the molecular detection of Sarcoptes scabiei from a skin scraping in patients with suspected scabies. PLoS Neglected Tropical Diseases. 2020;14(4):e0008229. [CrossRef]
- Hendrickx D, Bowen AC, Marsh JA, Carapetis JR, Walker R. Ascertaining infectious disease burden through primary care clinic attendance among young Aboriginal children living in four remote communities in Western Australia. PloS one. 2018;13(9):e0203684. [CrossRef]
- Amgarth-Duff I, Hendrickx D, Bowen A, Carapetis J, Chibawe R, Samson M, et al. Talking skin: attitudes and practices around skin infections, treatment options, and their clinical management in a remote region in Western Australia. Rural and remote health. 2019;19(3):5227. [CrossRef]
Figure 1.
Map of tropical Far North Queensland, Australia, showing catchment area for current scabies study (1 January 2000 to 31 December 2023). Image taken from Bird, K., Bohanna, I., McDonald, M., Wapau, H., Blanco, L., Cullen, J., McLucas, J., Forbes, S., Vievers, A., Strivens, E. and Barker, R. (2023). A good life for people living with disability: the story from Far North Queensland. Disability and Rehabilitation, 46(9), 1787–1795. https://doi.org/10.1080/09638288.2023.2205172.
Figure 1.
Map of tropical Far North Queensland, Australia, showing catchment area for current scabies study (1 January 2000 to 31 December 2023). Image taken from Bird, K., Bohanna, I., McDonald, M., Wapau, H., Blanco, L., Cullen, J., McLucas, J., Forbes, S., Vievers, A., Strivens, E. and Barker, R. (2023). A good life for people living with disability: the story from Far North Queensland. Disability and Rehabilitation, 46(9), 1787–1795. https://doi.org/10.1080/09638288.2023.2205172.
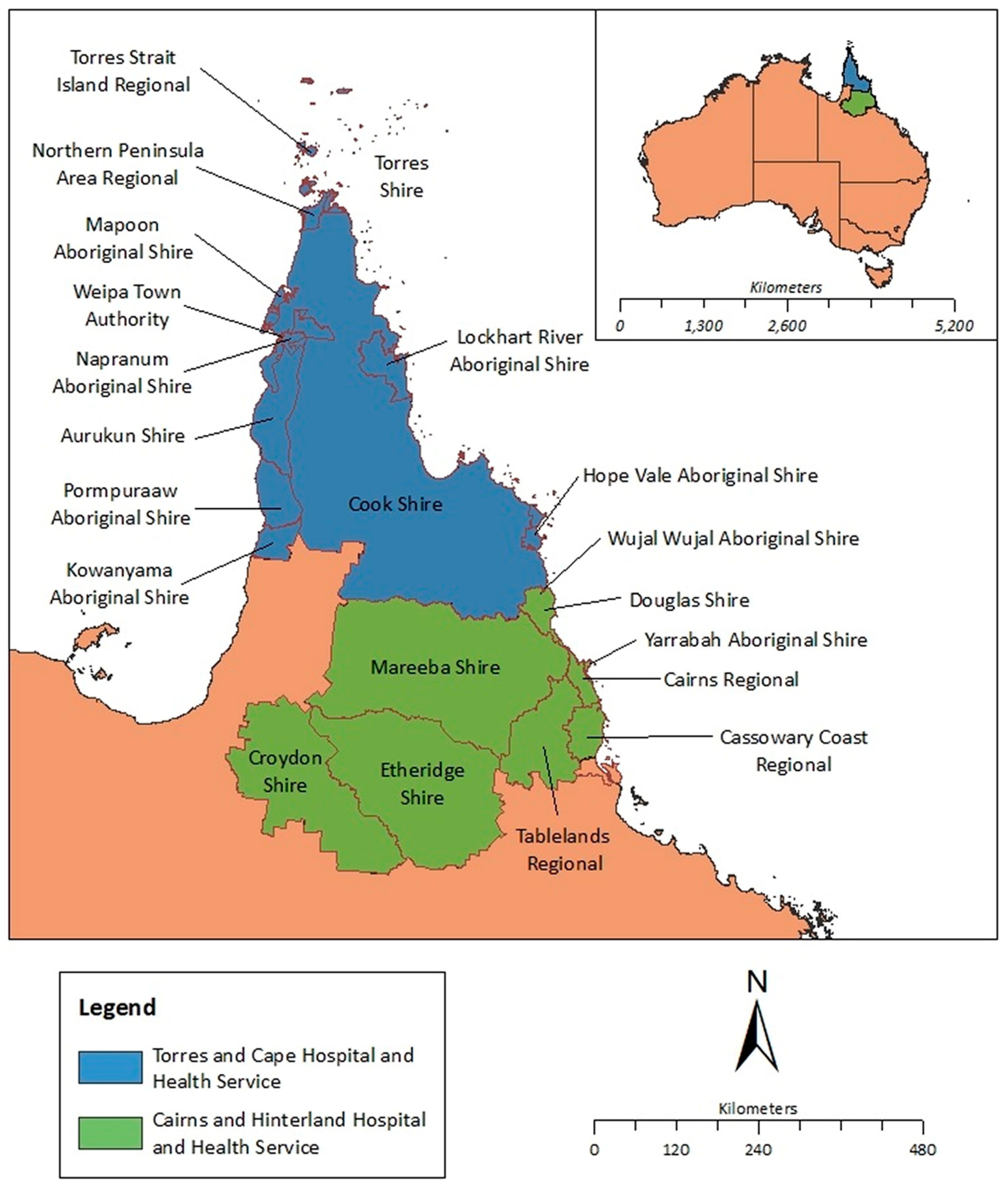
Figure 2.
Number of annual skin scraping episodes collected over a 24-year period (1st January 2000 to 31st December 2023) from Cairns Hospital in tropical Far North Queensland, Australia.
Figure 2.
Number of annual skin scraping episodes collected over a 24-year period (1st January 2000 to 31st December 2023) from Cairns Hospital in tropical Far North Queensland, Australia.
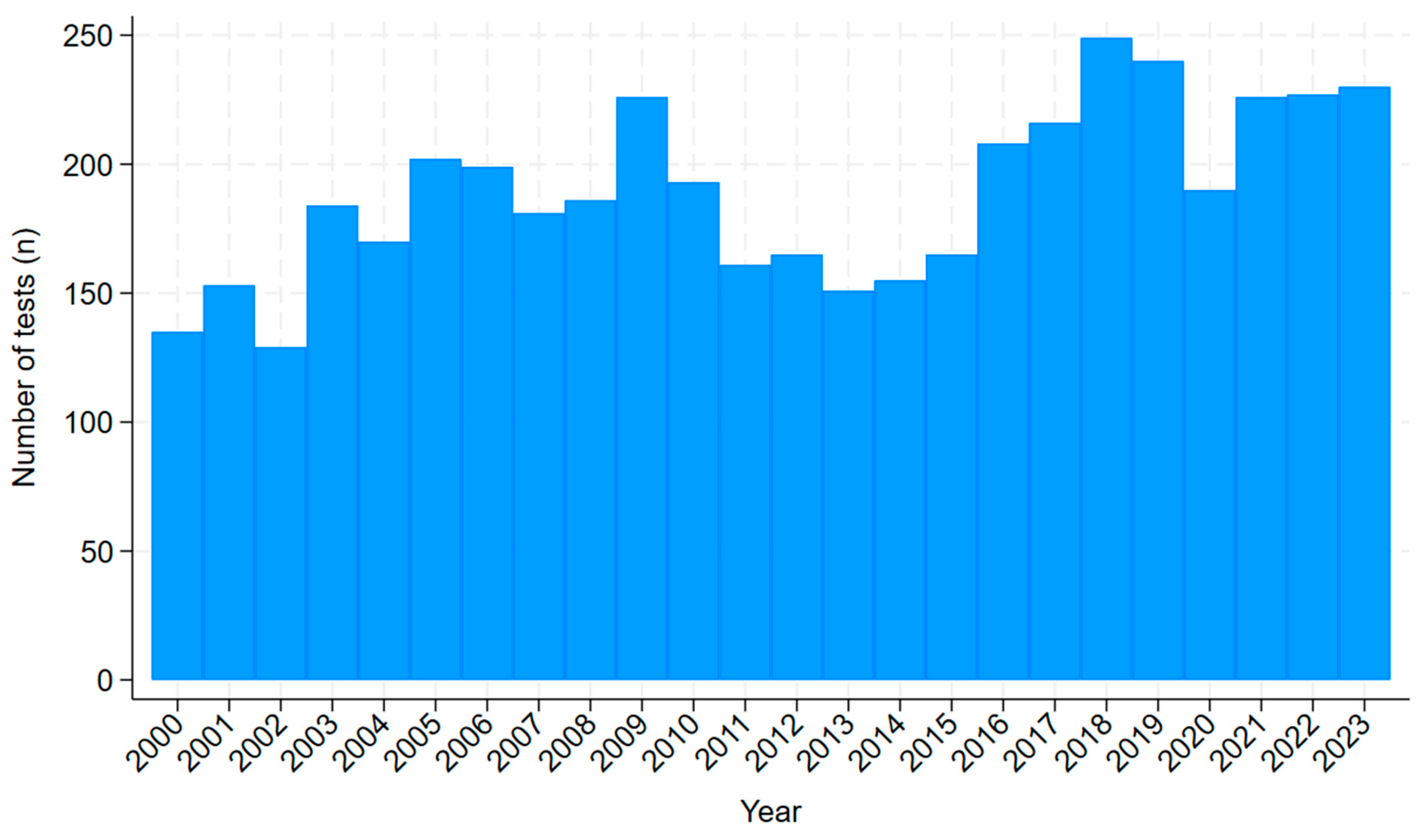
Figure 3.
Percentage of skin scraping episodes that were positive for scabies collected over a 24-year period (01-Jan-2000 and 31-Dec-2023) from Cairns Hospital in tropical Far North Queensland, Australia (with line of best fit to highlight trend).
Figure 3.
Percentage of skin scraping episodes that were positive for scabies collected over a 24-year period (01-Jan-2000 and 31-Dec-2023) from Cairns Hospital in tropical Far North Queensland, Australia (with line of best fit to highlight trend).
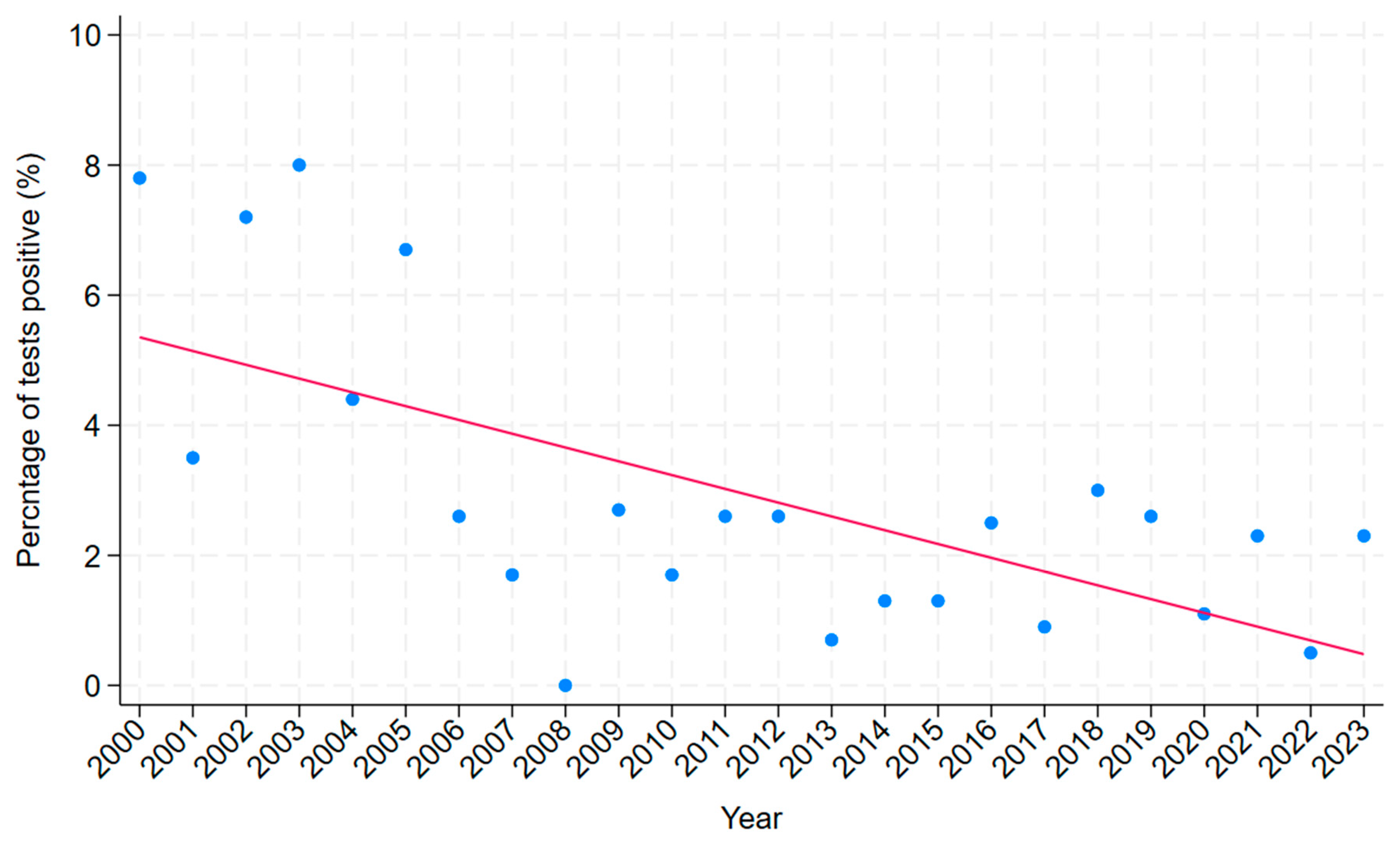
Figure 4.
Kaplan Meier Curve showing time to new diagnosis of ARF or RHD after the episode of skin scraping between 2000 and 2023 in Far North Queensland (individuals with ARF or RHD prior to skin scraping excluded from this analysis).
Figure 4.
Kaplan Meier Curve showing time to new diagnosis of ARF or RHD after the episode of skin scraping between 2000 and 2023 in Far North Queensland (individuals with ARF or RHD prior to skin scraping excluded from this analysis).
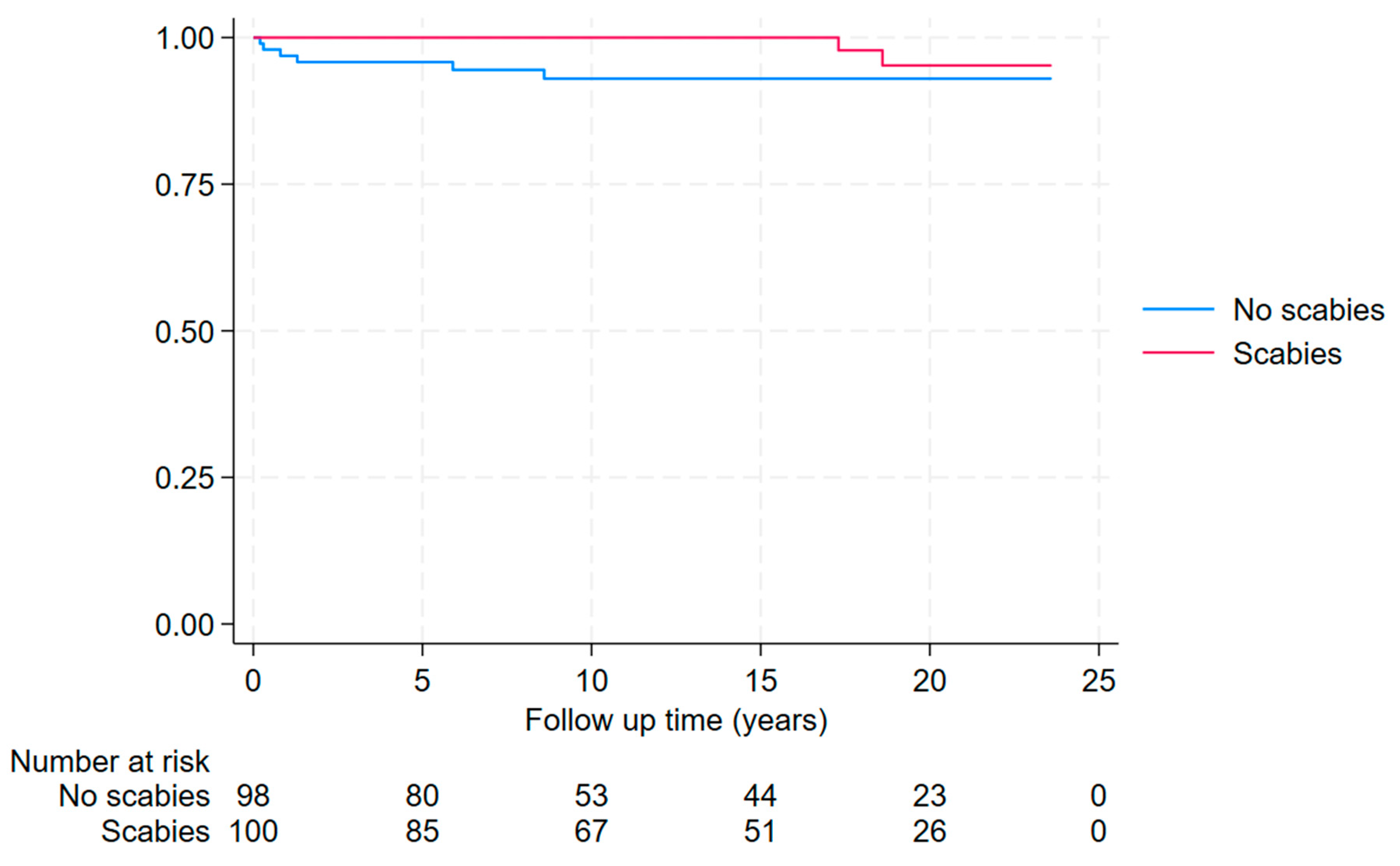
Figure 5.
Kaplan Meier Curve showing time to eGFR<60 mL/min/1.73m2 during follow-up after the episode of skin scraping between 2000 and 2023 in Far North Queensland (individuals with eGFR<60 mL/min/1.73m2 prior to skin scraping excluded from this analysis).
Figure 5.
Kaplan Meier Curve showing time to eGFR<60 mL/min/1.73m2 during follow-up after the episode of skin scraping between 2000 and 2023 in Far North Queensland (individuals with eGFR<60 mL/min/1.73m2 prior to skin scraping excluded from this analysis).
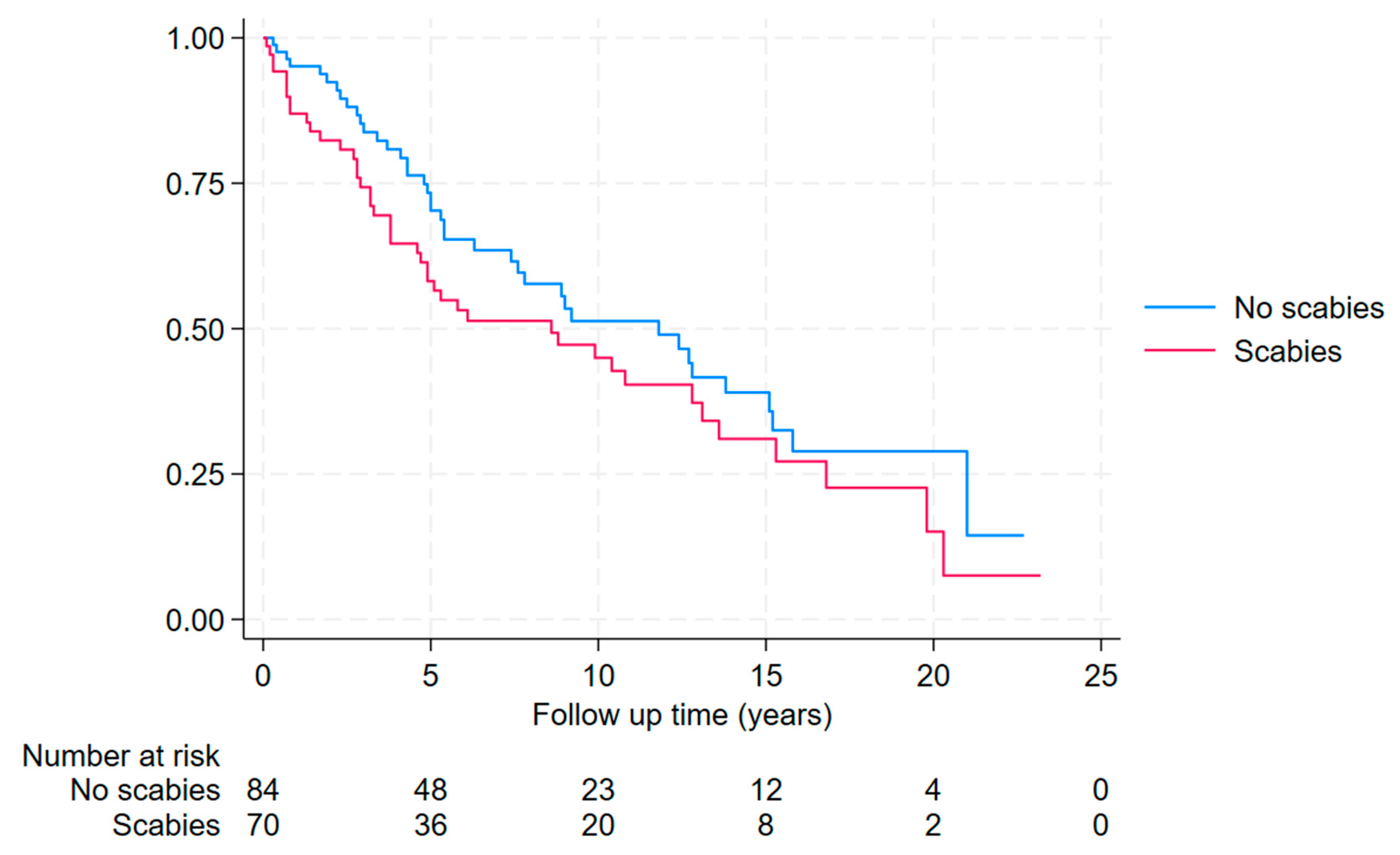

Table 1.
Association with a skin scraping positive for scabies.
| Variable | Total a | Positive | Negative | Odds ratio b (95% CI) | p b | Odds ratio c (95% CI) | p c |
|---|---|---|---|---|---|---|---|
| Tested in Cairns | 945/4342 (22%) | 67/120 (55%) | 878/4222 (20%) | 4.72 (3.28-6.81) | <0.001 | 6.18 (4.24-9.02) | <0.001 |
| First Nations Australian | 2706/4313 (63%) | 110/120 (92%) | 2596/4193 (61%) | 6.76 (3.53–12.96) | <0.001 | 10.54 (5.43-20.45) | <0.001 |
| Adult (age >16) | 3555/4345 (82%) | 116/121 (96%) | 3439/4224 (79%) | 5.30 (2.16–13.01) | <0.001 | 5.94 (2.40-14.69) | <0.001 |
| Female sex | 2174/4344 (50%) | 70/121 (58%) | 2104/4223 (48%) | 1.38 (0.96–1.99) | 0.08 | 1.13 (0.77-1.65) | 0.53 |
Percentages rounded to the nearest whole number. a Incomplete data for some of the 4345 episodes. b Odds ratio in univariate logistic regression. c Odds ratio in multivariate logistic regression.
Table 2.
Characteristics of presentations to Cairns Hospital Emergency Department with a diagnosis of classic scabies and crusted scabies.
Table 2.
Characteristics of presentations to Cairns Hospital Emergency Department with a diagnosis of classic scabies and crusted scabies.
| Classic scabies a (n=271) |
Crusted scabies a (n=21) |
Total (n= 292) |
|
|---|---|---|---|
| First Nations Australian | 197 (73%) | 19 (91%) | 216 (74.0%) |
| Male sex | 140 (52%) | 9 (43%) | 149 (51.0%) |
| Child (<16 years) | 150 (55%) | 8 (38%) | 158 (54.1%) |
| Scrapings performed | 9 (3%) | 5 (24%) | 14 (4.8%) |
| Positive skin scrapings | 0 | 1 (5%) | 1 (0.3%) |
| Infectious disease or dermatology service involvement | 7 (3%) | 6 (29%) | 13 (4.5%) |
| Complete documentation of IACS criteria b | 11 (4%) | 4 (19%) | 15 (5.1%) |
| Adequate documentation for clinical scabies diagnosis b | 115 (42%) | 11 (52%) | 126 (43.2%) |
| Satisfied IACS criteria for confirmed scabies b | 0 | 1 (5%) | 1/292 (0.3%) |
| Satisfied IACS for clinical scabies b | 88 (33%) | 13 (62%) | 101 (34.6 %) |
| Documented crusted scabies severity grading | Not Applicable | 2 (10%) d | Not Applicable |
| Followed all NT guidelines for crusted scabies c | Not Applicable | 1 (5%) | Not Applicable |
| Admitted to hospital from the Emergency Department | 60 (22%) | 16 (76%) | 76 (26.0%) |
a Based on the attending clinician’s documented assessment. b IACS criteria for the diagnosis of scabies (Supplementary Table S1).[38]. c Including skin scrapings, dermatology or infectious diseases service involvement, assessment of severity, and hospital admission. [40]. d Both cases were seen by dermatology.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



