Submitted:
03 March 2025
Posted:
03 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: While testing healthcare workers (HCWs) for SARS-CoV-2 is important to reduce transmission within healthcare settings, understanding the self-reported patterns of testing is important for interpreting vaccine effectiveness and other COVID-19-related information. Objective: Using longitudinal data from the COVID-19 Cohort Study, this study described trends in SARS-CoV-2 testing among Canadian HCWs between June 2020 and November 2023. Methods: HCWs completed an illness report for each instance of SARS-CoV-2 testing and episodes of symptoms compatible with COVID-19 even if untested. Overall rates of testing were calculated along with rates stratified by participating province, reason for testing, and COVID-19 vaccination status. Results: Rates of testing for SARS-CoV-2 generally mirrored rates of hospitalization for COVID-19 among Canadians. Rates of testing were highest during the Omicron BA.1 wave and varied by region, while vaccination status did not impact rates. The most commonly reported reason for testing was for symptoms; testing for known/possible exposure or routine reasons greatly decreased after the Omicron BA.1 wave. In participants who were tested for episodes of symptomatic illness, the mean time to first test was 1.3 days. Reported retesting after an initial negative result remained low throughout the study period. Conclusions: Understanding testing behaviours is important for public health decision-making including the analysis and interpretation of case data and vaccine effectiveness studies. It can also highlight possible missed case-finding opportunities in healthcare settings.
Keywords:
COVID-19
; healthcare workers
; Canada
; testing
Diagnostic testing for agents of infectious diseases such as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is imperative to facilitate timely treatment and improve prognosis and to trigger transmission-limiting behaviours [1,2]. At the facility level, the suspicion or confirmation of an infectious patient or healthcare worker (HCW) should prompt the implementation of enhanced infection prevention and control measures intended to protect other patients and staff [3]. At the population level, testing is a key element in population-based surveillance to inform public health intervention planning [4]. For researchers, participant-level self-reports represent a useful data collection method that can enhance formal reporting methods in the interpretation of findings [5].
There have been numerous changes in testing methods, access, and attitudes and behaviours for SARS-CoV-2 testing in Canada. Eligibility and testing criteria, availability of tests, type of tests, and reporting requirements have all changed over time [6]. At the beginning of the coronavirus disease 2019 (COVID-19) pandemic, testing was primarily completed using the polymerase chain reaction (PCR) tests that were administered in designated facilities by trained individuals and processed in the public health laboratory system [7]. Testing criteria were narrow and largely focused on individuals with symptoms compatible with COVID-19, a history of travel, or known exposure to a confirmed case of COVID-19 [6]. By May 2020, supply chain issues eased and testing was expanded [7]. By early 2022, rapid antigen tests (RATs) were widely deployed across Canada to enhance testing capacity [8]. PCR tests were still available and recommended for people at high risk of serious outcomes and for those working in high-risk institutions, such as acute care facilities [9,10,11,12]. While there are benefits to increased availability and accessibility to testing, one drawback of RATs is the decoupling from the public health reporting systems that hinders surveillance measures [13].
Observational study designs are commonly employed to evaluate real world vaccine effectiveness [14]. As such, it is important to understand differences that may bias the results. Beyond differences in barriers to testing and test accuracy, differences may occur in test-seeking behaviour, such as between vaccinated and unvaccinated individuals [15,16,17]. It is therefore important to understand the behaviours that lead to testing and to assess why and how often individuals seek testing [18].
Studies investigating SARS-CoV-2 testing trends among underserved or avoidant populations in Canada found lower rates of testing among individuals who identify as male [19,20,21,22,23], had lower levels of education [21,23], or who live in rural areas [19] or areas with higher densities of visible minority populations [23]. Conversely, higher rates of testing were noted in people with a known exposure to COVID-19 [20] or who had symptoms of COVID-19 [21]. Several studies noted variations or discrepant results in the effects by age, household income, and other social determinants of health, as well as between Canadian provinces [19,20,21,22,23]. The differences between provinces may reflect the influences of time and evolving provincial policies on testing behaviours. To the best of these authors’ knowledge, no studies have investigated the trends in SARS-CoV-2 testing in Canadian HCWs.
The COVID-19 Cohort Study (CCS) collected data from HCWs between June 2020 and November 2023, a period of many COVID-19-related scientific advances (e.g., vaccine development and deployment) and policy and attitude changes [24]. These data provide a unique opportunity to analyze testing patterns that would not be evident through traditional public health reporting.
This study sought to describe trends in SARS-CoV-2 testing among Canadian HCWs enrolled in the CCS from June 2020 to November 2023. Specifically, the objective was to describe temporal trends in rates of participant testing across geographic regions, vaccination status, and reasons for testing and to describe testing patterns within episodes of illnesses with COVID-19 compatible symptoms.
Materials and Methods
Design and Participants
This study was conducted as part of the CCS, a 42-month prospective cohort study following a group of HCWs working in acute care, rehabilitation, and complex care hospitals across four Canadian provinces [25]. Recruitment occurred immediately following ethical approval at each site, with staggered enrolment from June 2020 to June 2023. Recruitment commenced in Ontario in June 2020, followed by Alberta in March 2021, Nova Scotia in May 2021, and Quebec in June 2021 (see Supplementary Figure S1). Recruitment, consent, and data collection were conducted electronically due to COVID-19 restrictions on in-person research activities. Data were collected anonymously using a secure online platform; collection ended on December 1, 2023 or upon participant withdrawal, whichever occurred first.
Participants were eligible for inclusion in these analyses if they were 18 to 75 years of age at time of enrolment and employed >20 hours per week by an acute care, rehabilitation, or complex care hospital; or were a physician or nurse practitioner with hospital privileges and caring for ill patients ≥8 hours per week; or worked in a medical office providing patient care for >20 hours per week. Eligibility was restricted to participants who participated in the study for ≥30 days and completed at least one baseline survey. Participants were eligible irrespective of their COVID-19 vaccination status or history of COVID-19.
Testing for SARS-CoV-2
As active case identification was imperative for many of the proposed analyses of the CCS, efforts were made to ensure participants had access to SARS-CoV-2 testing throughout the study. At the initiation of the study, PCR testing was available to both HCWs and the public [7]. RAT kits became publicly available in December 2021 in Quebec, Nova Scotia and Alberta [26,27,28] and by February 2022 in Ontario [29]. As of April 1, 2023, COVID-19 assessment centres in most provinces, including Ontario, closed and RATs were no longer being distributed, but were available as long as supplies lasted [30]. To encourage continued testing, RAT kits were distributed to study participants starting in May 2023. Given the accessibility to testing throughout the study period, access and barriers to testing were not examined.
Data Collection
Following consent, participants were asked to complete a baseline questionnaire that captured demographic characteristics, health status, and practices in the workplace, household, and community that may be associated with risk of respiratory infection. Vaccination self-reports collected the dates COVID-19 vaccines were received and the vaccine product name; they also included an option to indicate that no doses were [yet] received.
Participants were also asked to complete an illness report each time they were tested for SARS-CoV-2, regardless of the test result or type of test, as well as each time they had symptoms of a respiratory illness, even if they were not tested. Participants reported the dates of the SARS-CoV-2 test, test results, symptoms, and known/suspected exposures to people with COVID-19 prior to becoming symptomatic or being tested, as applicable. Participants had the opportunity to provide additional details as desired in an open-text question for general comments. For reports of symptomatic illness without a reported symptom onset date, the date of SARS-CoV-2 test was considered the symptom onset date (n=5). In June 2021, the illness report was revised to reduce participant burden associated with daily reporting of ongoing symptomatic episodes; daily updates for the duration of symptoms were condensed into a single report.
Data Preparation
Open text responses in the illness reports were reviewed for additional details about reasons for testing and/or additional tests for which participants did not create individual reports. In instances of additional tests, new reports were created if sufficient detail was provided (i.e., date and reason for testing).
Events of interest, i.e. rate of testing for SARS-CoV-2 and episodic testing trends for symptomatic illness, were calculated using four-week periods starting on June 16, 2020, the date of the first submission of an illness report. Participants’ times at risk were calculated for each four-week window accounting for leaves, changes of workplace, or withdrawals.
Responses to variables asking about symptoms, recent exposure to person(s) with COVID-19, and stated reason for testing were reviewed alongside open text responses to categorize reason for testing into the following three categories: 1) symptomatic, with or without known or suspected COVID-19 exposure; 2) known or suspected exposure in the absence of symptoms; and 3) routine testing, defined as testing with no reported symptoms and no known exposure (e.g., travel, social events, non-outbreak-related screening, or fitness to work assessments). Testing for symptoms included any of the following: new or worsening cough, new shortness of breath, chest pain (pressure or heaviness), feeling feverish, chills, or shivering, a fever of >37.6o Celsius, feeling generally unwell, new onset of abnormal tiredness, confusion, new onset of generalized muscle aches or pains, new onset of joint pain, ear ache or infection, unusual headaches, sinus pain, sore or scratchy throat, new onset of a loss of appetite, nausea and/or vomiting, diarrhea, new onset of a loss in taste or smell. These liberal criteria were used because infection with SARS-CoV-2 has been associated with a wide range of symptoms [31,32], and because testing was initially recommended for the presence of any symptom for HCWs [33].
An episode of symptomatic illness was defined as a report of new onset of any symptom(s) in a previously asymptomatic individual, starting from the reported symptom onset date. Any reports with symptoms within a ±14-day window were considered one episode of symptomatic illness; this period was extended when a participant reported ongoing symptoms without resolution. The denominator for analyses included all symptomatic illness reports, whether or not they were tested for SARS-CoV-2.
Participants were assigned the vaccination status they reported as of 10 days before the first day of each four-week period (to account for time to mount an immune response). Categories were 1) never vaccinated or one dose of a two-dose vaccine received, 2) most recent dose (excluding first dose of a two dose primary series) received ≤6 months prior, 3) most recent dose (as above) received >6 but ≤12 months prior, and 4) most recent dose (as above) received >12 months prior.
Statistical Analyses
Rate of SARS-CoV-2 Testing
Outcomes were dichotomized (tested versus not tested for SARS-CoV-2) for each four-week period of participation. Calculations per 1000 person-days at risk were made for overall rates of testing as well as rates by reason for testing, province, and vaccination status; data from 76 participants were excluded from the vaccination status analysis due to missing data. Participant tests were eligible only once per four-week period for the rates of overall, by province, and vaccination status testing. Rates of testing by reason could include more than one test per participant per four-week period if participants were tested for different reasons within the period; 11 tests were excluded from this analysis due to missing data. Poisson confidence intervals at the 95% level were calculated for graphs [34].
Results are displayed alongside Canadian data of hospitalization rates for COVID-19 [35] with a nine-day lag to incorporate time from symptom onset to hospitalization [36]. Hospitalization rates were used since they were less biased than case counts; case counts became increasingly unreliable after changes to testing eligibility in December 2021 [35].
Testing Based on Symptom Profile
Given the importance of rapid identification of infectious individuals to help reduce transmission, the time to first tests among HCWs with episodes of symptomatic illness were calculated using the mean and median times between symptom onset and first reported test for SARS-CoV-2; a cut-off of seven days from symptom onset was used to classify the participant as having been tested within the episode. Symptom onset was considered day zero, the succeeding day as day one, and so forth.
Episodes of symptomatic illness were then assigned to a four-week period (as described above) based on symptom onset date. Following the recommended timeline for retesting of 48 hours [when using RATs] by the U.S. Food and Drug Administration in 2022 [37] and by the Public Health Agency of Canada in 2023 [38], episodes of symptomatic illness that were initially tested within two days of symptom onset and reported a negative result were reviewed for a subsequently reported test(s) within two days following the negative test.
Results and Discussion
Of the 2793 HCWs enrolled in the CCS, 2535 (90.8%) were eligible for inclusion in this analysis (81 did not complete a baseline report, 177 participated for <30 days). The median age of those included was 40 years at enrolment, 2162 (85.3%) identified themselves as female, and 1538 (60.7%) participants worked in Ontario. See Table 1 for complete demographic details. A timeline of recruitment and active participation of HCWs included in these analyses is provided in Figure 1.
Rate of SARS-CoV-2 Testing
Rates of testing for SARS-CoV-2 fluctuated over the 3.5 years of data collection, as seen in Figure 2. Of note, the study began in June 2020, subsequent to increased access to testing for SARS-CoV-2 [7]. Rates of testing peaked at 11.9 participants tested at least once per 1000 person-days during the Omicron BA.1 wave, considerably higher than the 2.1 per 1000 person-days reported during the summer of 2023. Differences in rates may have been driven by changes in guidelines and policies, burden of community transmission of COVID-19 and other respiratory illnesses, as well as perceptions about individual susceptibility to SARS-CoV-2 and severity of COVID-19 [18,41,42,43].
Using the rates of hospitalization as a proxy for community transmission, the largest divergence between rates of HCW participant testing and rates of COVID-19 related hospitalization occurred early in the study, from June to December 2020 (see Figure 2). As shown in Figure 3, rates of testing for routine purposes (no symptoms and no known exposures to known/suspected cases) were similar to rates of testing due to symptoms and due to exposure to a case until the start of the Omicron waves, but declined in importance thereafter. This is likely because testing was used to enhance case finding and to reduce transmission of COVID-19 in healthcare settings prior to the availability of COVID-19 vaccines in Canada; vaccines were initially available in December 2020, but with very limited supply for several months [44,45]. Routine testing of HCWs was promoted in 2020 as a tactic to reduce occupational spread from atypical, mild, or asymptomatic cases of COVID-19 [46,47]. Routine testing was implemented for international travel [48], staff and visitors in long-term care homes [49], or (infrequently) as an alternative to vaccination in mandated settings [50].
Overall rates of testing in this HCW population were generally lower in 2021 than in 2020. This may be attributed to increasing COVID-19 vaccination coverage [51]. A 2021 Health Canada report [52] credited the reduction in test-seeking after the introduction of vaccines to a lower perception of risk from COVID-19, testing/pandemic fatigue, and/or the social cost of a positive result outweighing the benefit of being tested at the individual level. As shown in Figure 4, however, there is no discernable difference in rates of testing based on vaccination status in this sample of HCWs, with the notable exception of a spike in testing among recent recipients of vaccines in early 2021. This may reflect symptomatic testing due to vaccine side effects. This occurred prior to the implementation of policies in the spring of 2021 in Ontario, where the majority of our participants resided, that made exceptions for testing HCWs who had mild symptoms (headache, fatigue, muscle ache/joint pain) within 48 hours after vaccination unless COVID-19 was suspected for some other reason [53]. In contrast to our findings, Glasziou et al. [16] found that fully vaccinated adult participants in Australia were twice as likely as unvaccinated ones to report intentions to be tested if they awoke with a sore throat in late 2021. Alternatively, Kuitunen et al., [17] who surveyed the general public in Finland, found that those who had received three doses of vaccine against COVID-19 by January 2022 had the lowest testing rate, while those who were unvaccinated had the highest rate. These discrepant findings illustrate the need to understand each population’s testing behaviours. Further, it has been suggested that symptomatic individuals may have attributed their symptoms to respiratory illnesses other than COVID-19 and therefore did not seek testing for this reason [41]; however, this last point was not stratified by vaccination status, which may be noteworthy given the change in symptom profile/burden associated with COVID-19 illness in vaccinated individuals [31,54].
The social cost of a positive result on testing for SARS-CoV-2 is difficult to interpret [52] and was affected by policies on paid sick leave across Canada during the COVID-19 pandemic. The federal Canada Recovery Sickness Benefit, that supported individuals without access to paid sick leave, was in effect from September 2020 to May 2022 [55]. Provincial governments also implemented or modified existing paid sick leave policies, resulting in a variety of policies across the country [56] precluding us from making inferences on how paid sick leave may have been associated with changes in testing behaviours in this cohort.
A sharp increase in rates of testing coincided with the waves caused by the Omicron BA.1 and BA.2 variants in late 2021 through June 2022. As shown in Figure 3, participants reported that the reason for testing during this period was largely for symptoms compatible with COVID-19. The increase in the overall rate of testing (Figure 2) mirrors the increase in rates of hospital admission for COVID-19. This suggests that increasing community transmission does impact testing behaviours for people with symptoms. Similar to our results, Brankston et al. [57] reported that precautionary behaviours (avoiding close contact and indoor gatherings) among Canadian adults increased in the context of increasing COVID-19 incidence in 2020.
This period (late 2021/early 2022) also marked a dramatic shift in eligibility for PCR testing, that was restricted to high-risk individuals and settings, along with increasing availability of RATs to the general public [43,58,59]. An Australian study found increased test-seeking was associated with the increased availability of RATs [18]. Although RATs became the most commonly reported type of test used among those reporting positive results across Canada in January 2022 [59], a significant and sustained increase in testing was not noted in this study of HCW. This may be because the HCW population remained eligible for PCR testing for many months after it was made more restrictive for the general public [9,10,11,12]. However, it may also be related, in part, to under-reporting of testing with RATs, ostensibly those with negative results, by study participants.
COVID-19 does not have a discernable seasonal pattern of infection [60] and although there is some variability in rates of testing by season, the patterns are not consistent. This was expected in 2020/2021 when nonpharmaceutical interventions to stop the spread of COVID-19 caused an “effective absence” of the annual seasonal respiratory virus epidemic in Canada [61]. A delayed return of influenza circulation within the community was observed in the spring of the 2021-2022 season in Canada coinciding with the easing of transmission-limiting interventions, with pre-pandemic-like influenza circulation patterns returning in the 2022-2023 season [62,63]. Seasonal endemic co-circulation of multiple respiratory viruses in the winter months lends support for the utility of testing symptomatic HCWs for multiple pathogens using point-of-care multiplex tests in periods of high community transmission of respiratory pathogens [64]. In the meantime, rates of testing due to the presence of symptoms will likely be inflated during periods of co-circulating respiratory viruses making it necessary to consider these data in analyses.
The reported rates of testing after exposure to someone with COVID-19 but prior to exhibiting symptoms was generally lower than rates of testing due to being symptomatic (Figure 3). The rates of testing due to an exposure generally mirrored those for symptomatic testing (and hospitalization) but steadily declined, relative to symptomatic testing, following the wave caused by the Omicron BA.1 variant. This may have been, in part, due to changes in recommendations for HCWs, and a need to re-evaluate case and contact management procedures [65]. During 2020, enhanced case and contact management in Ontario included advising close contacts of cases to seek testing [66]. At the start of the Omicron BA.1 wave in December 2021, when increased community transmission and demand for testing outpaced the capacity of COVID-19 assessment centres [43], guidelines for testing were changed to include only symptomatic individuals with a higher risk of severe illness and/or symptomatic individuals working in high-risk settings, including acute care facilities [9,10,11,12].
Rate of SARS-CoV-2 Testing by Province
HCWs in Ontario, Quebec, and Alberta reported similar rates of testing and although Nova Scotia followed similar trends in peaks in rates of testing to the other three provinces, the rates were consistently higher (Figure 5). Although there are differences in population size, density and demographics amongst the provinces, there were also differences in terms of their approach to the COVID-19 pandemic [67] that is under the legislative responsibility of the provinces and territories in Canada [68]. During the pandemic, the Atlantic provinces (Nova Scotia, New Brunswick, Prince Edward Island, Newfoundland and Labrador) had a relatively successful proactive and coordinated containment strategy whereby they assertively traced and isolated cases and increased travel restrictions [67,69]. Transmission rates remained low and the province was able to avoid province-wide lockdowns [67]. In comparison, Ontario, Quebec, and Alberta experienced prolonged periods of lockdown and comparatively higher mortality rates [67]. Nova Scotia also implemented a “circuit breaker”, a period of increased testing and restrictions in response to an increase in cases of COVID-19 in April 2021 [67]. This explains the initial peak in the rate of testing when Nova Scotian participants first enrolled in the study. Note that the relatively smaller number of participants in Alberta, Nova Scotia, and Quebec (see Figure 1) make the results more reactive to increased testing during outbreaks or periodic mass screening within the participating hospitals.
Timing of Test Taking
Recalling that a symptomatic illness was defined as illness with any of the above-listed symptoms, there were 5880 reports of symptomatic illness. Of the episodes that were tested within 7 days of symptom onset (n=4984 or 84.8%), the median number of days to the first test was 1, with a mean of 1.3 days (95% confidence interval 1.3, 1.4); 29.5% of episodes were tested on the day of symptom onset. Early in the pandemic, it was acknowledged that people working in healthcare settings may face an increased risk of exposure to SARS-CoV-2 given the likelihood of contact with individuals ill with COVID-19 [70] and that HCWs could initiate or amplify the spread of COVID-19 in healthcare settings [71,72]. Our finding, that Canadian HCWs sought testing for SARS-CoV-2 upon recognition of symptoms suggests they were cognizant of the risks associated with their employment and were responsive to actions intended to protect patients and families. Gamble et al. [73] reported similar findings in their study of critical care nurses in Canada in 2020/2021. However, within our study, 741 episodes (13%) received their first test three to seven days after symptom onset and another 15% of episodes were not tested within seven days of symptom onset highlighting that potential transmission was possible for many HCWs. Further study into the attitudes and risk factors associated with delayed or missed testing is warranted.
Qualitative Responses to Reasons for Being Tested
Many study participants volunteered their reason for not being tested, however, they were not solicited so are not necessarily representative. The most common reason symptomatic participants used for not being tested was that they attributed their symptoms to post-vaccination side effects. As one participant stated, “I'm pretty sure the symptoms I experienced were merely a side effect of the booster shot.”. Several participants said that they monitored their symptoms post-vaccination, specifically onset relative to time of vaccination, what the symptoms were and their duration, and factored this into their judgement about whether or not a test was necessary. One HCW noted that they had “diarrhea, vomiting, loss of smell...all side effects of the booster”. While some studies and case reports reported the presence of post-vaccination olfactory and gustatory disorders [74,75], these symptoms were rare and worthy of further investigation.
Other reasons for not being tested for SARS-CoV-2 included receiving an alternative diagnosis from a medical professional “Was diagnosed with strep throat”; assuming the illness was another infectious agent “My son got flu from daycare and we all got it”; “I have a cold. (No fever, chills) I just need a good night's sleep.”; other ill family members or contacts had tested negative for COVID-19 “My children had been tested the week before due to cold symptoms and they were negative.”; testing was not recommended/required by their Occupational Health team “Felt overly fatigued for 5 days - missed one day of work. Was not required to get Covid tested”; “Occupational Health did not recommend I get swabbed for COVID.”; symptoms were due to environmental exposures such as allergies or poor air quality “Coughing due to smoky conditions from forest fires.”; lingering side effects from a previous COVID-19 infection “Still lingering symptoms from my covid infection - seems to get better and then worse and back and forth”; not having access to COVID-19 tests, which was quoted infrequently, “During holidays. I had no COVID test with me”; and assuming they were COVID-19 positive given their symptoms and a close contact exposure “Only work from home so did not PCR. Spouse was positive on RAT”. Future studies that elicit reasons for not being tested will also aid in our understanding and may aid in the development of targeted interventions to increase uptake of diagnostic testing when indicated.
Some of the reasons, particular those with self-diagnosis of other viral illnesses, present missed opportunities for testing for SARS-CoV-2 and the potential for spread of COVID-19 within the healthcare facility if proper precautions were not followed. The ongoing challenge with many respiratory [and other] illnesses is that people can present with a wide variety of symptoms or can be asymptomatic [31,32]. It is therefore important that other layers of protection are implemented to reduce the risks of transmission from unidentified sources. Vaccination and universal masking have the dual benefit of protecting the HCW from infection and reducing the risk of forward transmission [76,77,78]. Many healthcare settings across Canada have or are moving towards making vaccination for several vaccine-preventable diseases (e.g., influenza, measles) a condition of employment [77]. Healthcare settings are also encouraged to consider universal masking policies for HCWs during times of increased community transmission of respiratory pathogens to reduce transmission within their facilities [79].
Retesting After a Negative Result
Testing too early or too late in the illness process may reduce test sensitivity [80]. This is further complicated by lower viral loads in vaccinated and previously infected individuals [81,82] along with a delay in peak viral loads with the Omicron variant [83], for example. As such, if people tested only once, and not at the optimal time, cases of COVID-19 may have been missed.
As shown in Figure 6, the overall rate of re-testing after an initial negative test for symptomatic reports was low; it was <14% throughout the duration of data collection. Low rates of re-testing early in the pandemic were likely because repeat testing was not generally recommended when tested by PCR [9,10,11,12]. At this time, evidence suggested that repeat testing would not provide enough benefit to outweigh the burden it would have placed on the laboratory system [10]. It is also likely that study participants under-reported repeat tests within one episode of illness due to the burden of doing so on the online reporting system.
An increase in re-testing following a negative test occurred towards the end of the Delta period, coinciding with the availability of RATs. While RATs improved access to testing, the difference in sensitivity and specificity of the tests must be considered. The U.S. Food and Drug Administration recommended repeat testing after 48 hours following a negative result on a RAT due to lower sensitivity compared with a PCR test [37,84]. In addition, Frediani et al. [83] found low estimates of sensitivity of RATs on the first day of symptoms (30-60%) from samples collected from symptomatic individuals, with sensitivity peaking on day four of symptoms (80-93%), which is consistent with a delayed peak viral load observed during the Omicron and recombinant variant waves of the pandemic. It is important that these limitations are accounted for when interpreting surveillance, research, and diagnostic data. It is also important to consider these limitations when using RATs to investigate infection with SARS-CoV-2 among HCWs; procedures may include requiring a second negative test result 48 hours after the first or if the HCW must work, wearing a tight-fitting respirator or mask and modifying work duties to enhance physical distancing [85].
Study Strengths and Limitations
This data was collected over a 3.5 year period and four Canadian provinces enabling comparison across time and place, including the potential temporal influences of public policy and scientific advancements such as the introduction of the RAT and of COVID-19 vaccines. It enabled investigation of temporality, including whether symptom onset preceded SARS-CoV-2 testing, more sufficiently than many surveillance programs and retrospective studies. Further, our study captures multiple occupations within the healthcare environment that may acquire or transmit SARS-CoV-2 within their workplace, providing a more complete picture than those that only capture clinical roles. The online reporting platform and questionnaire also allowed for more in-depth investigation into episodes of illness.
Given that information and events were self-reported, there was likely under-reporting of illnesses and/or testing, as competing priorities related to responding to the COVID-19 pandemic would have made frequent reporting especially burdensome. Under-reporting was likely even more pronounced for negative tests as was found in an analysis of public testing behaviours conducted in the United Kingdom [86]. To reduce the effect of under-reporting, testing within each four-week period was used for these analyses under the assumption that participants would be less likely to report subsequent tests within the same episode or to report subsequent illnesses within a short period. Social desirability bias may have also contributed to under-reporting as it was possible that symptomatic participants who were not tested did not submit an illness report. The use of anonymized surveys was used in an attempted to reduce this bias, however, it was not possible to reduce the burden of completing reports.
This study relied on voluntary participation making it unlikely that participants were representative of all HCWs in Canada. In addition, other studies report selection bias as health-conscious individuals were more likely to participate in studies [87] and that may inflate the observed rates of testing for SARS-CoV-2 among HCWs. The dynamic nature of participation in the CCS also increases the possibility of differences among participants over time that could potentially bias rates of testing if participants who were more or less likely to test were also more or less likely to continue their participation in the study. The rolling enrolment by province may reduce the generalizability of our findings in 2020 and early 2021, before all four participating provinces were enrolled. Finally, participating hospitals were located in large metropolitan areas so findings may not be generalizable to healthcare facilities in smaller jurisdictions.
Conclusions
Testing for SARS-CoV-2 within the Canadian HCW study population fluctuated over the 3.5 years of data collection with rates generally following the rates of hospitalization for COVID-19 in Canada, a proxy for rates of infection. The spread of the Omicron variant signalled a shift in the way Canadian governments dealt with the COVID-19 pandemic and there was a shift in the patterns of testing at this point. As such, monitoring and understanding the effects of internal (e.g., HCWs ability to recognize COVID-19 symptoms, attitudes towards testing or perceived risks of testing), and external (e.g. testing eligibility and availability) influences on testing rates and behaviours over time is important for interpreting data for vaccine effectiveness studies and surveillance information that impacts public health decision-making. It can also highlight instances of missed case-finding opportunities that can drive transmission in healthcare settings.
Data availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Conflicts of interest
The authors declare that they have no competing interests.
Funding statement
This work was funded by the Canadian Institutes of Health Research [173212 & 181116]; the Weston Family Foundation [no number]; and Physicians’ Services Incorporated Foundation [6014200738]. Funders had no role in the collection, analysis, or interpretation of data, writing of the manuscript, or the decision to submit it for publication.
Acknowledgements
The investigators thank their staff, who worked tirelessly throughout the study and the participants, who gave freely of their time amidst the stress of working during the pandemic. We also thank the non-author members of the CCS working group for their contributions to the studies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Trends in testing for SARS-CoV-2 among healthcare workers in a Canadian cohort study during the COVID-19 pandemic, June 2020 to November 2023.
References
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat Rev Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Shang, M.; Guo, J.; Guo, J. Point-of-care testing of infectious diseases: Recent advances. Sens Diagn. 2023, 2, 1123–1144. [Google Scholar] [CrossRef]
- World Health Organization. Core components for infection prevention and control programmes: Report of the Second Meeting Informal Network on Infection Prevention and Control in Health Care [Internet]. Geneva, Switzerland, 2008. Available online: https://iris.who.int/bitstream/handle/10665/69982/WHO_HSE_EPR_2009.1_eng.pdf;jsessionid=2692FD4093AF143ACA71B0B15295DF61?sequence=1 (accessed on 15 September 2024).
- Kanyangarara, M.; Daguise, V.; Gual-Gonzalez, L.; Litwin, A.H.; Korte, J.; Ross, C.; et al. COVID-19 Testing Practices, Preventive Behaviors, and Factors Associated With Test Positivity: Population-Based Statewide Survey Study. JMIR Public Health Surveill. 2023, 9, e34579. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J Multidiscip Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, E.; Bielska, I.A.; Hopkins, S.; Belal, A.A.; Goldstein, D.M.; Slick, J.; et al. Limitations of COVID-19 testing and case data for evidence-informed health policy and practice. Health Res Policy Syst. 2023, 21, 11. [Google Scholar] [CrossRef]
- Lee, M.H.-Y.; Xu, G.; Cheng, F.; Khalid, A.F. Testing surge capacity—A Canadian COVID-19 experience, Ontario's surge capacity for the first wave. Health Policy. 2021, 125, 1291–1296. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Interim guidance on the use of rapid antigen detection tests for the identification of SARS-CoV-2 infection [Internet]. Government of Canada, 2024. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/use-rapid-antigen-detection-tests.html (accessed on 15 September 2024).
- Alberta Health Services. Information for AHS Staff & Health Professionals: COVID-19 [Internet]. 2023. Available online: https://web.archive.org/web/20230404181411/https://www.albertahealthservices.ca/topics/Page16947.aspx (accessed on 15 September 2024).
- Government of Ontario. COVID-19 testing and treatment [Internet]. 2022. Available online: https://www.ontario.ca/page/covid-19-testing-and-treatment (accessed on 15 September 2024).
- Government of Québec. Getting a COVID-19 test [Internet]. 2023. Available online: https://web.archive.org/web/20230202174514/https://www.quebec.ca/en/health/advice-and-prevention/screening-and-carrier-testing-offer/testing-flu-like-symptoms/get-covid-19-test#c148948 (accessed on 1 October 2024).
- Nova Scotia Health. COVID-19 Testing [Internet]. 2023. Available online: https://web.archive.org/web/20230406001955/https://www.nshealth.ca/coronavirustesting (accessed on 1 October 2024).
- Health Canada. Pan-Canadian COVID-19 Testing and Screening Guidance: Technical guidance and implementation plan [Internet]. 2021. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/medical-devices/testing/pan-canadian-guidance.html (accessed on 1 October 2024).
- World Health Organization. Evaluation of COVID-19 vaccine effectiveness: Interim guidance; World Health Organization: Geneva, 17 March 2021. [Google Scholar]
- Bodner, K.; Irvine, M.A.; Kwong, J.C.; Mishra, S. Observed negative vaccine effectiveness could be the canary in the coal mine for biases in observational COVID-19 studies. Int J Infect Dis. 2023, 131, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Glasziou, P.; McCaffery, K.; Cvejic, E.; Batcup, C.; Ayre, J.; Pickles, K.; et al. Testing behaviour may bias observational studies of vaccine effectiveness. J Assoc Med Microbiol Infect Dis Can. 2022, 7, 242–246. [Google Scholar] [CrossRef]
- Kuitunen, I.; Uimonen, M.; Seppälä, S.J.; Ponkilainen, V.T. COVID-19 vaccination status and testing rates in Finland-A potential cause for bias in observational vaccine effectiveness analysis. Influenza Other Respir Viruses. 2022, 16, 842–845. [Google Scholar] [CrossRef]
- Eales, O.; Teo, M.; Price, D.J.; Hao, T.; Ryan, G.E.; Senior, K.L.; et al. Temporal trends in test-seeking behaviour during the COVID-19 pandemic. medRxiv 2024. [Google Scholar] [CrossRef]
- Antonova, L.; Somayaji, C.; Cameron, J.; Sirski, M.; Sundaram, M.E.; McDonald, J.T.; et al. Comparison of socio-economic determinants of COVID-19 testing and positivity in Canada: A multi-provincial analysis. PLoS ONE. 2023, 18, e0289292. [Google Scholar] [CrossRef]
- Caya, C.; Menzies, D.; Papenburg, J.; Yansouni, C.; Campbell, J. Characteristics associated with SARS-CoV-2 testing, infection and vaccine uptake among essential non-healthcare workers in Montréal, 2021. Can Commun Dis Rep. 2024, 50, 223–232. [Google Scholar] [CrossRef]
- Pongou, R.; Ahinkorah, B.O.; Mabeu, M.C.; Agarwal, A.; Maltais, S.; Yaya, S. Examining the association between reported COVID-19 symptoms and testing for COVID-19 in Canada: A cross-sectional survey. BMJ Open. 2022, 12, e056229. [Google Scholar] [CrossRef]
- Righolt, C.H.; Zhang, G.; Sever, E.; Wilkinson, K.; Mahmud, S.M. Patterns and descriptors of COVID-19 testing and lab-confirmed COVID-19 incidence in Manitoba, Canada, March 2020-May 2021: A population-based study. Lancet Reg Health Am. 2021, 2, 100038. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, M.E.; Calzavara, A.; Mishra, S.; Kustra, R.; Chan, A.K.; Hamilton, M.A.; et al. Individual and social determinants of SARS-CoV-2 testing and positivity in Ontario, Canada: A population-wide study. Canadian Medical Association Journal. 2021, 193, E723. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Research to Insights: A look at Canada’s economy and society three years after the start of the COVID-19 pandemic [Internet]. 2023. Available online: https://www150.statcan.gc.ca/n1/pub/11-631-x/11-631-x2023004-eng.htm (accessed on 15 September 2024).
- Coleman, B.L.; Gutmanis, I.; Bondy, S.J.; Harrison, R.; Langley, J.; Fischer, K.; et al. Canadian health care providers' and education workers' hesitance to receive original and bivalent COVID-19 vaccines. Vaccine. 2024, 42, 126271. [Google Scholar] [CrossRef]
- Alberta Health. COVID-19 information : COVID-19 rapid testing : Information sheet [Internet]. 2021. Available online: https://open.alberta.ca/publications/covid-19-information-covid-19-rapid-testing#detailed (accessed on 15 September 2024).
- Government of Nova Scotia. Rapid Tests Available at Libraries for Holiday Season [Internet]. 2021. Available online: https://news.novascotia.ca/en/2021/12/13/rapid-tests-available-libraries-holiday-season (accessed on 2 September 2024).
- Ministère de la Santé et des Services sociaux Québec. Pandémie de la COVID-19 - Des tests de dépistage rapide distribués graduellement pour l’ensemble de la population [Internet]. 2021. Available online: https://www.msss.gouv.qc.ca/ministere/salle-de-presse/communique-3350/ (accessed on 15 September 2024).
- Government of Ontario. Ontario Expanding Access to Free Rapid Tests for General Public [Internet]. 2022. Available online: https://news.ontario.ca/en/release/1001575/ontario-expanding-access-to-free-rapid-tests-for-general-public (accessed on 15 September 2024).
- Government of Ontario. Rapid Testing for At-Home Use [Internet]. 2022. Available online: https://www.ontario.ca/page/rapid-testing-home-use (accessed on 15 September 2024).
- Fischer, K.; Langley, J.M.; Harrison, R.; Mubareka, S.; Nadarajah, J.; Smieja, M.; et al. Recent vaccination against SARS-CoV-2 is associated with less severe disease in working-age adults. Int J Environ Res Public Health 2024, 21, 1501. [Google Scholar]
- Whitaker, M.; Elliott, J.; Bodinier, B.; Barclay, W.; Ward, H.; Cooke, G.; et al. Variant-specific symptoms of COVID-19 in a study of 1,542,510 adults in England. Nat Commun. 2022, 13, 6856. [Google Scholar] [CrossRef]
- Ontario Ministry of Health. COVID-19 Provincial Testing Guidance Update: April 15, 2020 [Internet]. 2020. Available online: https://www.corhealthontario.ca/Item-4-Provincial-Testing-Guidance-Update.pdf (accessed on 30 September 2024).
- Crow, E.L.; Gardner, R.S. Confidence Intervals for the Expectation of a Poisson Variable. Biometrika. 1959, 46, 441–453. [Google Scholar] [CrossRef]
- Government of Canada. COVID-19 epidemiology update: Current situation [Internet]. 2024. Available online: https://health-infobase.canada.ca/covid-19/current-situation.html (accessed on 5 March 2024).
- Ward, T.; Fyles, M.; Glaser, A.; Paton, R.S.; Ferguson, W.; Overton, C.E. The real-time infection hospitalisation and fatality risk across the COVID-19 pandemic in England. Nat Commun. 2024, 15, 4633. [Google Scholar] [CrossRef]
- U.S Food; Drug Administration. At-Home COVID-19 Antigen Tests-Take Steps to Reduce Your Risk of False Negative Results: FDA Safety Communication [Internet]. 2022. Available online: https://www.fda.gov/medical-devices/safety-communications/home-covid-19-antigen-tests-take-steps-reduce-your-risk-false-negative-results-fda-safety (accessed on 1 October 2024).
- Public Health Agency of Canada. Information for patients: A guide to antigen self-testing for COVID-19 [Internet]. 2023. Available online: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19/testing-screening-contact-tracing/information-patients-guide-self-testing.html (accessed on 4 November 2024).
- Microsoft Corporation. Microsoft Excel for Microsoft 365.
- StataCorp. Stata Statistical Software: Release 18.5; College Station, TX, 2024. [Google Scholar]
- Bevan, I.; Stage Baxter, M.; Stagg, H.R.; Street, A. Knowledge, Attitudes, and Behavior Related to COVID-19 Testing: A Rapid Scoping Review. Diagnostics 2021, 11, 1685. [Google Scholar] [CrossRef] [PubMed]
- Pitzer, V.E.; Chitwood, M.; Havumaki, J.; Menzies, N.A.; Perniciaro, S.; Warren, J.L.; et al. The Impact of Changes in Diagnostic Testing Practices on Estimates of COVID-19 Transmission in the United States. Am J Epidemiol. 2021, 190, 1908–1917. [Google Scholar] [CrossRef]
- Yuan, P.; Aruffo, E.; Tan, Y.; Yang, L.; Ogden, N.H.; Fazil, A.; et al. Projections of the transmission of the Omicron variant for Toronto, Ontario, and Canada using surveillance data following recent changes in testing policies. Infect Dis Model. 2022, 7, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. COVID-19 vaccination: Doses administered [Internet]. 2024. Available online: https://health-infobase.canada.ca/covid-19/vaccine-administration/ (accessed on 25 September 2024).
- Office of the Premier. News Release: Ontario Enhancing COVID-19 Case and Contact Management [Internet]. Government of Ontario Newsroom, 2020. Available online: https://news.ontario.ca/en/release/57279/ontario-enhancing-covid-19-case-and-contact-management (accessed on 30 September 2024).
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet. 2020, 395, 1418–1420. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.J.; Rosella, L.; Milijasevic, N.; Small, L.N. Mass testing for asymptomatic COVID-19 infection among health care workers at a large Canadian hospital. J Assoc Med Microbiol Infect Dis Can. 2020, 5, 245–250. [Google Scholar] [CrossRef]
- Transport Canada. New pre-departure COVID-19 testing requirements come into effect for all air travellers flying into Canada [Internet]. 2021. Available online: https://www.canada.ca/en/transport-canada/news/2021/01/new-pre-departure-covid-19-testing-requirements-come-into-effect-for-all-air-travellers-flying-into-canada.html (accessed on 15 September 2024).
- Government of Ontario. COVID-19: Long-term care home surveillance testing and access to homes [Internet]. 2020. Available online: https://www.ontario.ca/page/covid-19-long-term-care-home-surveillance-testing (accessed on 1 October 2024).
- Government of Alberta. New Vaccination Policy for Alberta Public Servants [Internet]. 2021. Available online: https://www.alberta.ca/release.cfm?xID=79917372CAAE4-A799-9E9B-C3F39550E2141819 (accessed on 15 September 2024).
- Government of Canada. COVID-19 vaccination in Canada [Internet]. 2021. Available online: https://web.archive.org/web/20211201003830/https://health-infobase.canada.ca/covid-19/vaccination-coverage/ (accessed on 1 October 2024).
- Health Canada. Testing for COVID-19 in vaccinated populations [Internet]. 2021. Available online: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19/testing-screening-contact-tracing/testing-vaccinated-populations.html#a8 (accessed on 1 October 2024).
- Ontario Ministry of Health. Guidance for Employers Managing Workers with Symptoms within 48 Hours of COVID-19 or Influenza Immunization [Internet]. 2021. Available online: https://files.ontario.ca/moh-guidance-employers-managing-workers-symptoms-48-hours-covid-19-influenza-immunization-en.pdf (accessed on 30 September 2024).
- World Health Organization. Coronavirus disease (COVID-19): Vaccines and vaccine safety [Internet]. 2024. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease- (accessed on day month year).
- Canada Revenue Agency. COVID-19 benefits from the CRA: Canada Recovery Sickness Benefit (CRSB). 2022. Available online: https://www.canada.ca/en/revenue-agency/services/benefits/recovery-sickness-benefit.html (accessed on 4 November 2024).
- MacIsaac, S.; Morissette, R. Employee paid sick leave coverage in Canada, 1995 to 2022 2023. Available online: https://www150.statcan.gc.ca/n1/pub/36-28-0001/2023010/article/00001-eng.htm (accessed on 4 November 2024).
- Brankston, G.; Merkley, E.; Loewen, P.J.; Avery, B.P.; Carson, C.A.; Dougherty, B.P.; et al. Pandemic fatigue or enduring precautionary behaviours? Canadians’ long-term response to COVID-19 public health measures. Prev Med Rep. 2022, 30, 101993. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Federal, Provincial, Territorial Public Health Response Plan for Ongoing Management of COVID-19 [Internet]. Government of Canada, 2022. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/federal-provincial-territorial-public-health-response-plan-ongoing-management-covid-19.html (accessed on 1 October 2024).
- Statistics Canada. Self-reported COVID-19 test results in Canada, January 2020 to March 2022 [Internet]. 2022. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/220906/dq220906a-eng.htm (accessed on 15 September 2024).
- Public Health Agency of Canada. Full Report: The Chief Public Health Officer of Canada's Report on the State of Public Health in Canada 2023. 2023. Available online: https://www.canada.ca/en/public-health/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/state-public-health-canada-2023/report.html (accessed on 4 November 2024).
- Groves, H.E.; Piché-Renaud, P.-P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; et al. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg Health Am. 2021, 1, 100015. [Google Scholar] [CrossRef]
- Health Infobase. Laboratory Data Report: Respiratory Virus Trends in Canada. 2024. Available online: https://health-infobase.canada.ca/respiratory-virus-detections/ (accessed on 4 November 2024).
- Schmidt, K.; Ben Moussa, M.; Buckrell, S.; Rahal, A.; Chestley, T.; Bastien, N.; et al. National Influenza Annual Report, Canada, 2022-2023: Canada's first fall epidemic since the 2019-2020 season. Can Commun Dis Rep. 2023, 49, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Canadian Agency for Drugs and Technologies in Health. Point-of-Care Tests for COVID-19 and Influenza in Canada [Internet]. Ottawa, Ontario, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK604825/ (accessed on 15 September 2024).
- Government of Ontario. Ontario Updating Public Health Measures and Guidance in Response to Omicron 2021. Available online: https://news.ontario.ca/en/release/1001386/ontario-updating-public-health-measures-and-guidance-in-response-to-omicron (accessed on 4 November 2024).
- Ontario Ministry of Health. Protecting Ontarians Through Enhanced Case and Contact Management [Internet]. 2020. Available online: https://www.oha.com/Bulletins/Protecting%20Ontarians%20through%20Enhanced%20Case%20and%20Contact%20Management%20-%20June%2018,%202020.pdf (accessed on 30 September 2024).
- Broschek, J. Federalism, political leadership and the COVID-19 pandemic: Explaining Canada’s tale of two federations. Territ Politic Gov. 2022, 10, 779–798. [Google Scholar] [CrossRef]
- Government of Canada. Testing for COVID-19: Roles and responsibilities across Canada [Internet]. 2023. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/testing/roles-responsibilities.html (accessed on 4 September 2024).
- Executive Council. Atlantic Premiers Working Together to Improve Health Care and Promote Prosperity [Internet]. Newfoundland & Labrador Canada, 2021. Available online: https://www.gov.nl.ca/releases/2021/exec/0928n07/ (accessed on 10 October 2024).
- Government of Canada. COVID-19 infections among healthcare workers and other people working in healthcare settings [Internet]. 2022. Available online: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19/epidemiological-economic-research-data/infections-healthcare-workers-other-people-working-healthcare-settings.html (accessed on 4 September 2024).
- Abbas, M.; Robalo Nunes, T.; Martischang, R.; Zingg, W.; Iten, A.; Pittet, D.; et al. Nosocomial transmission and outbreaks of coronavirus disease 2019: The need to protect both patients and healthcare workers. Antimicrob Resist Infect Control. 2021, 10, 7. [Google Scholar] [CrossRef]
- Asad, H.; Johnston, C.; Blyth, I.; Holborow, A.; Bone, A.; Porter, L.; et al. Health Care Workers and Patients as Trojan Horses: A COVID19 ward outbreak. Infect Prev Pract. 2020, 2, 100073. [Google Scholar] [CrossRef]
- Gamble, K.; Murthy, S.; Silverberg, S.L.; Gobat, N.; Puchalski Ritchie, L.M. Canadian critical care nurses experiences on the front lines of the COVID-19 pandemic: A qualitative descriptive study. BMC Nurs. 2022, 21, 330. [Google Scholar] [CrossRef]
- Arabzadeh Bahri, R.; Esmaeilpur Abianeh, F.; Peisepar, M.; Hadi, R.; Basti, F.A.; Maleki, S.; et al. Anosmia or Ageusia Following COVID-19 Vaccination: A Systematic Review. Ear Nose Throat J. 2024, 103, 164s–70s. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Diallo, A.O.; Dachy, B.; Bon, S.D.L.; Maniaci, A.; Vaira, L.A.; et al. COVID-19: Post-vaccine Smell and Taste Disorders: Report of 6 Cases. Ear Nose Throat J. 2024, 103, NP104–NP7. [Google Scholar] [CrossRef]
- Klompas, M.; Pearson, M.; Morris, C. The Case for Mandating COVID-19 Vaccines for Health Care Workers. Ann Intern Med. 2021, 174, 1305–1307. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Immunization of Workers: Canadian Immunization Guide: For Health Professionals. 2024. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-3-vaccination-specific-populations/page-11-immunization-workers.html#p3c10t1 (accessed on 6 November 2024).
- Seidelman, J.L.; Lewis, S.S.; Advani, S.D.; Akinboyo, I.C.; Epling, C.; Case, M.; et al. Universal masking is an effective strategy to flatten the severe acute respiratory coronavirus virus 2 (SARS-CoV-2) healthcare worker epidemiologic curve. Infect Control Hosp Epidemiol. 2020, 41, 1466–1467. [Google Scholar] [CrossRef]
- Lai, J.; Coleman, K.K.; Tai, S.H.S.; German, J.; Hong, F.; Albert, B.; et al. Relative efficacy of masks and respirators as source control for viral aerosol shedding from people infected with SARS-CoV-2: A controlled human exhaled breath aerosol experimental study. eBioMedicine. 2024, 104, 105157. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Testing for COVID-19: Test accuracy [Internet]. Government of Canada, 2023. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/testing/accuracy.html (accessed on 15 September 2024).
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir Med. 2021, 9, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Puhach, O.; Meyer, B.; Eckerle, I. SARS-CoV-2 viral load and shedding kinetics. Nat Rev Microbiol. 2023, 21, 147–161. [Google Scholar] [CrossRef]
- Frediani, J.K.; Parsons, R.; McLendon, K.B.; Westbrook, A.L.; Lam, W.; Martin, G.; et al. The New Normal: Delayed Peak SARS-CoV-2 Viral Loads Relative to Symptom Onset and Implications for COVID-19 Testing Programs. Clin Infect Dis. 2024, 78, 301–307. [Google Scholar] [CrossRef]
- Canadian Public Health Laboratory Network Laboratory Directors Council and the Canadian Public Health Laboratory Network Respiratory Virus Infection Working Group. Interim guidance for the detection of SARS-CoV-2 with the Abbott Panbio COVID-19 antigen rapid test. Can Commun Dis Rep. 2021, 47, 17–22. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Respiratory Infectious Diseases: How to Reduce the Spread with Personal Protective Measures 2024 [cited 2024 Nov 6].
- UK Health Security Agency. COVID-19: General public testing behaviours [Internet]. 2023. Available online: https://www.gov.uk/government/publications/lfd-tests-how-and-why-they-were-used-during-the-pandemic/covid-19-general-public-testing-behaviours#references (accessed on 15 September 2024).
- Graham, M.S.; May, A.; Varsavsky, T.; Sudre, C.H.; Murray, B.; Kläser, K.; et al. Knowledge barriers in a national symptomatic-COVID-19 testing programme. PLOS Glob Public Health. 2022, 2, e0000028. [Google Scholar] [CrossRef]
Figure 1.
Person-days of participation, by province; eligible Canadian healthcare workers in the COVID-19 Cohort Study, June 2020-November 2023.
Figure 1.
Person-days of participation, by province; eligible Canadian healthcare workers in the COVID-19 Cohort Study, June 2020-November 2023.
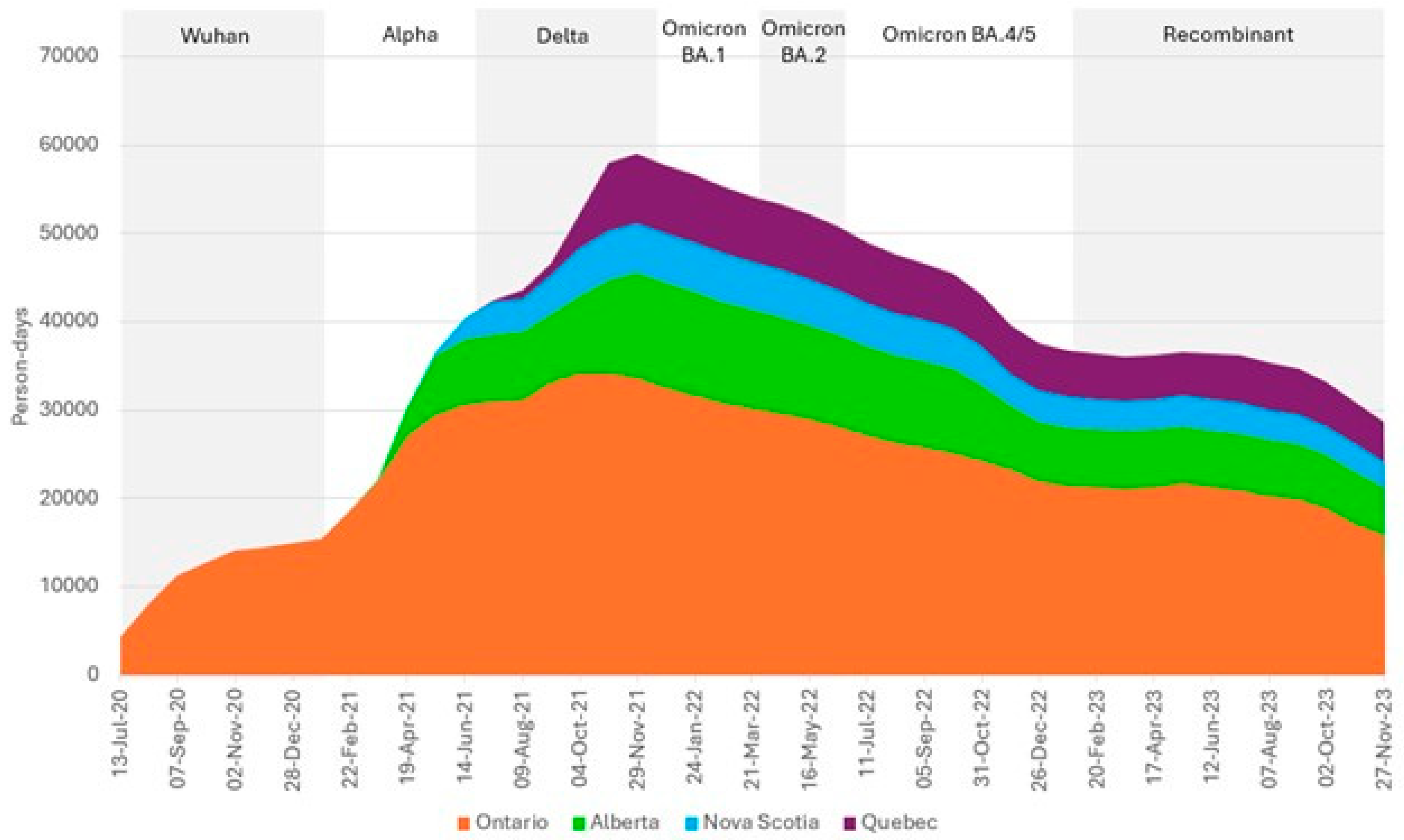
Figure 2.
Rates of testing for SARS-CoV-2 by Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023 and rates of hospital admission for COVID-19 in Canada. CI: confidence interval; Blue: Rate of testing for SARS-CoV-2 per 1000 person-days within each 4-week period; Blue dashed lines: 95% confidence interval for rate of testing; Green: Weekly rate of hospitalizations for COVID-19 per 100,000 Canadians (all ages).
Figure 2.
Rates of testing for SARS-CoV-2 by Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023 and rates of hospital admission for COVID-19 in Canada. CI: confidence interval; Blue: Rate of testing for SARS-CoV-2 per 1000 person-days within each 4-week period; Blue dashed lines: 95% confidence interval for rate of testing; Green: Weekly rate of hospitalizations for COVID-19 per 100,000 Canadians (all ages).
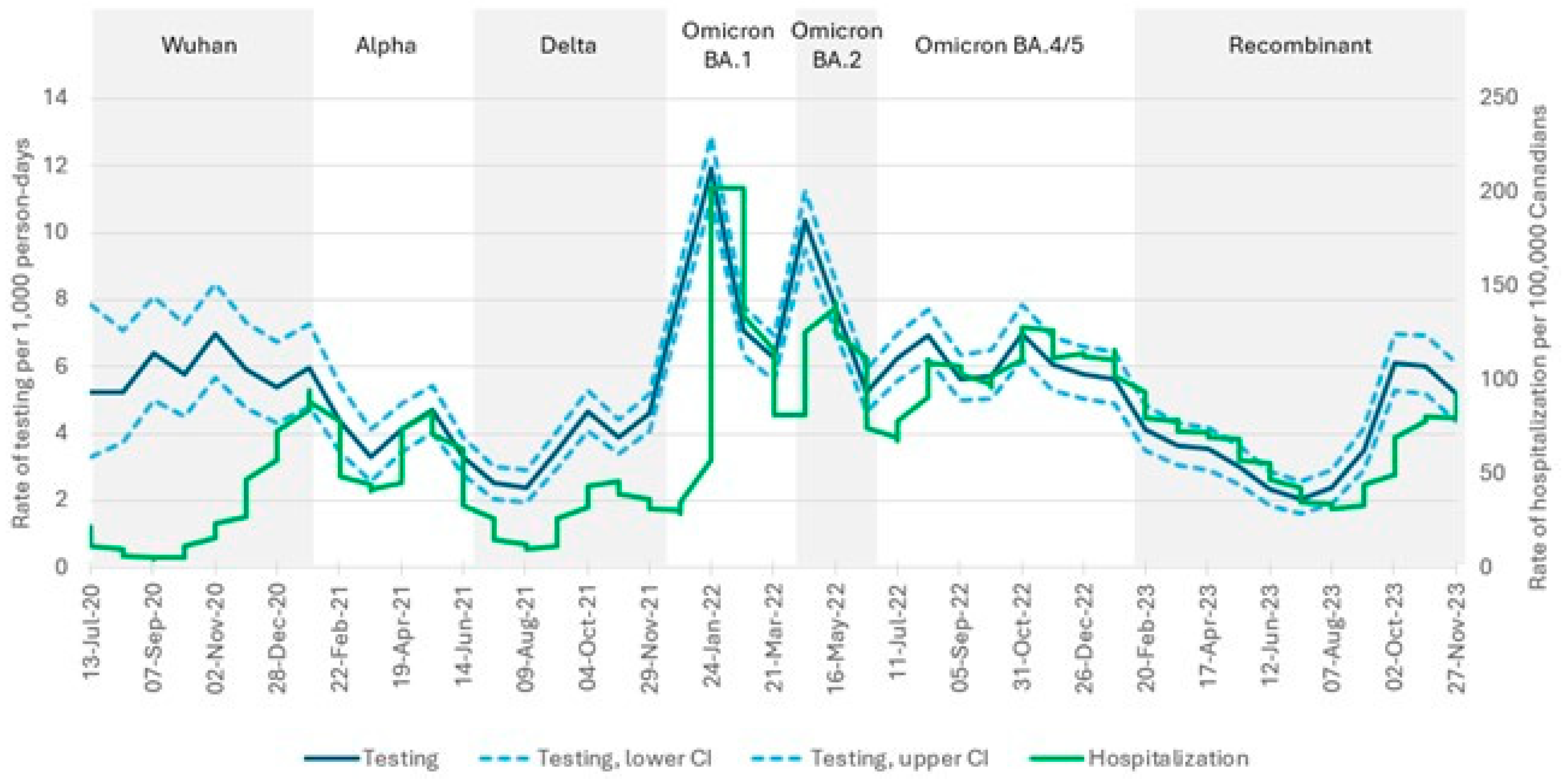
Figure 3.
Rates of testing for SARS-CoV-2 by reason for testing, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates are per 1000 person-days, for each four-week period.
Figure 3.
Rates of testing for SARS-CoV-2 by reason for testing, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates are per 1000 person-days, for each four-week period.
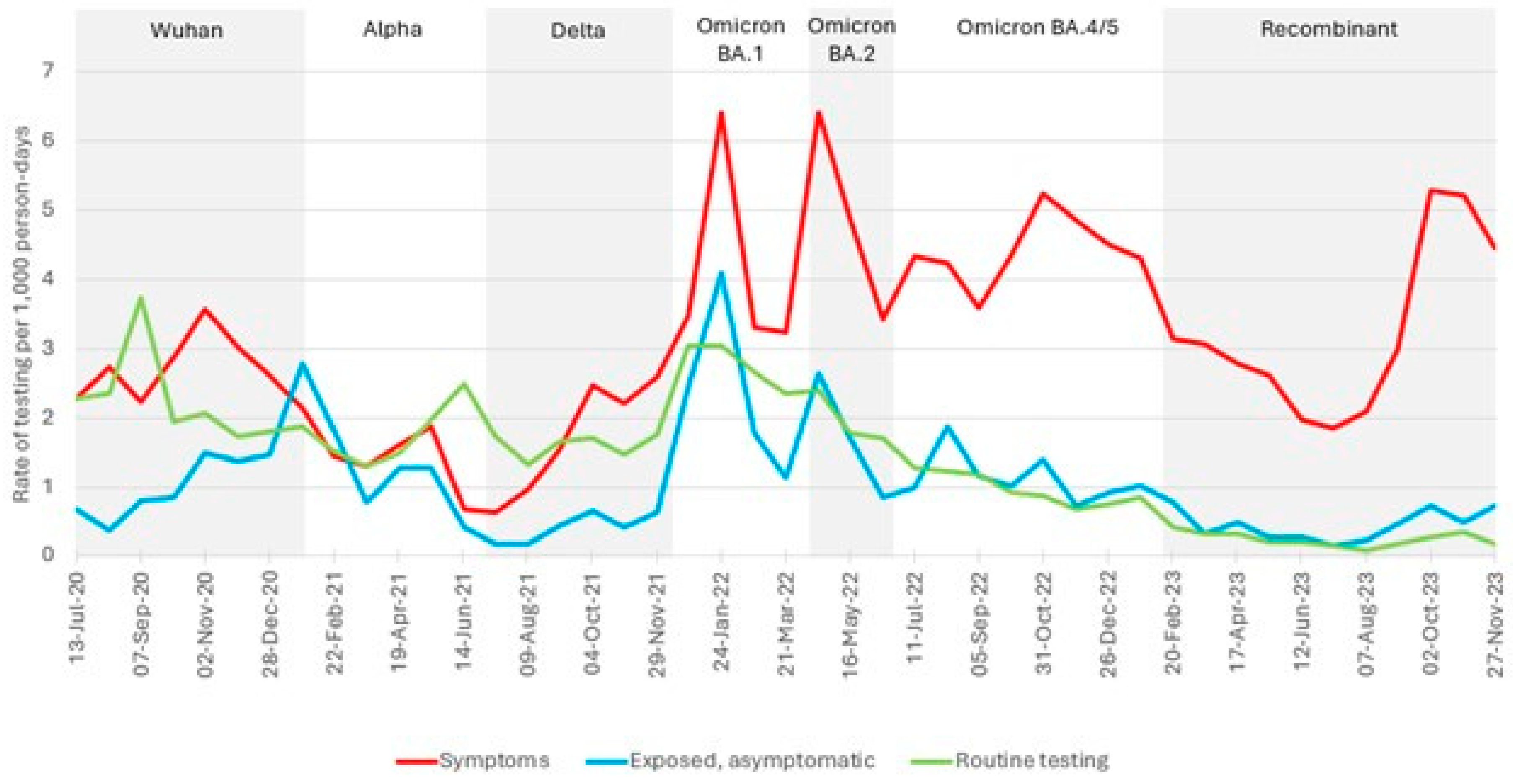
Figure 4.
Rates of testing for SARS-CoV-2 by vaccination status, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates are per 1000 person-days, for each four-week period.
Figure 4.
Rates of testing for SARS-CoV-2 by vaccination status, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates are per 1000 person-days, for each four-week period.
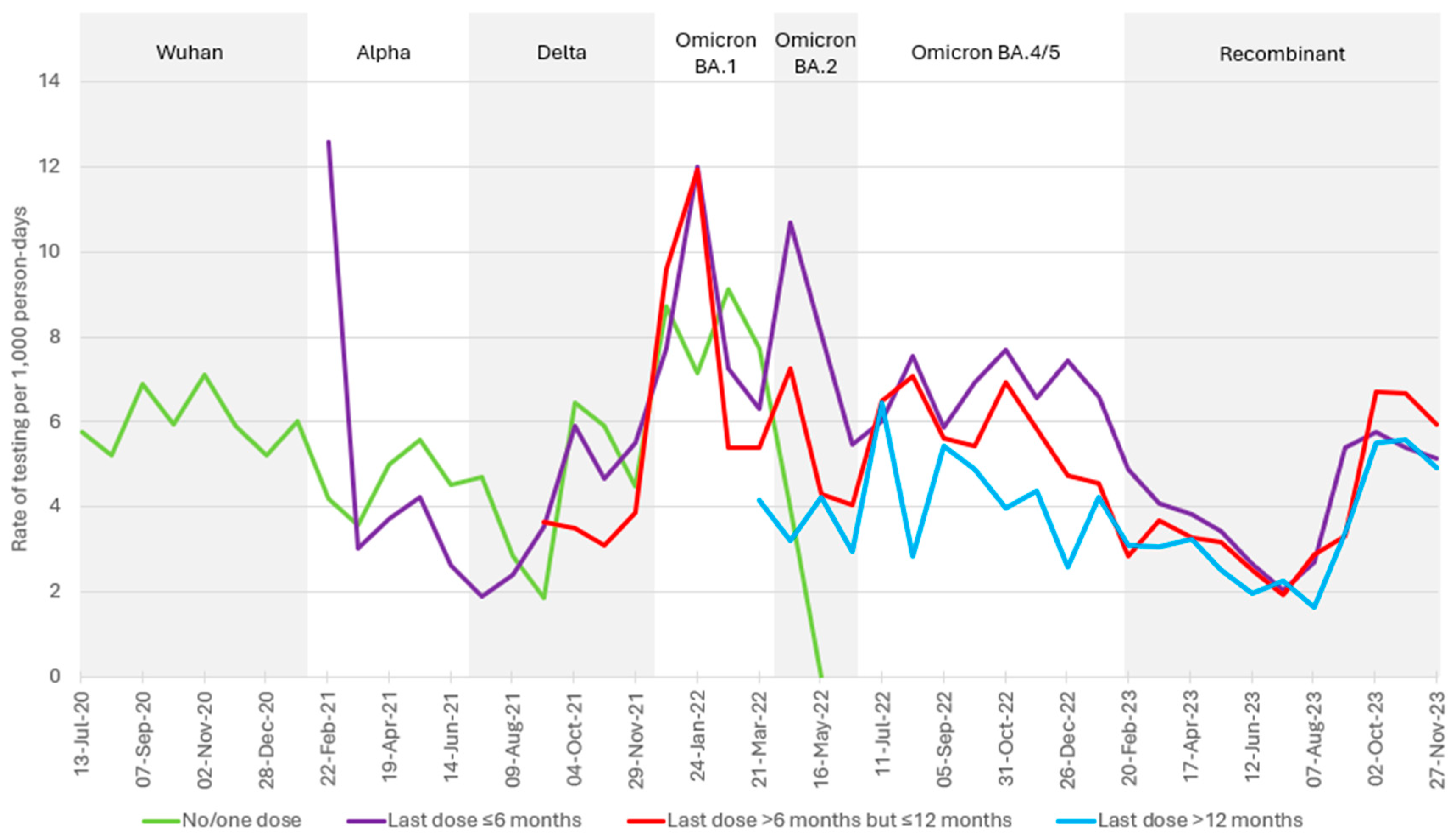
Figure 5.
Rates of testing for SARS-CoV-2 by province, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates per 1000 person-days participation within each four-week period.
Figure 5.
Rates of testing for SARS-CoV-2 by province, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Rates per 1000 person-days participation within each four-week period.
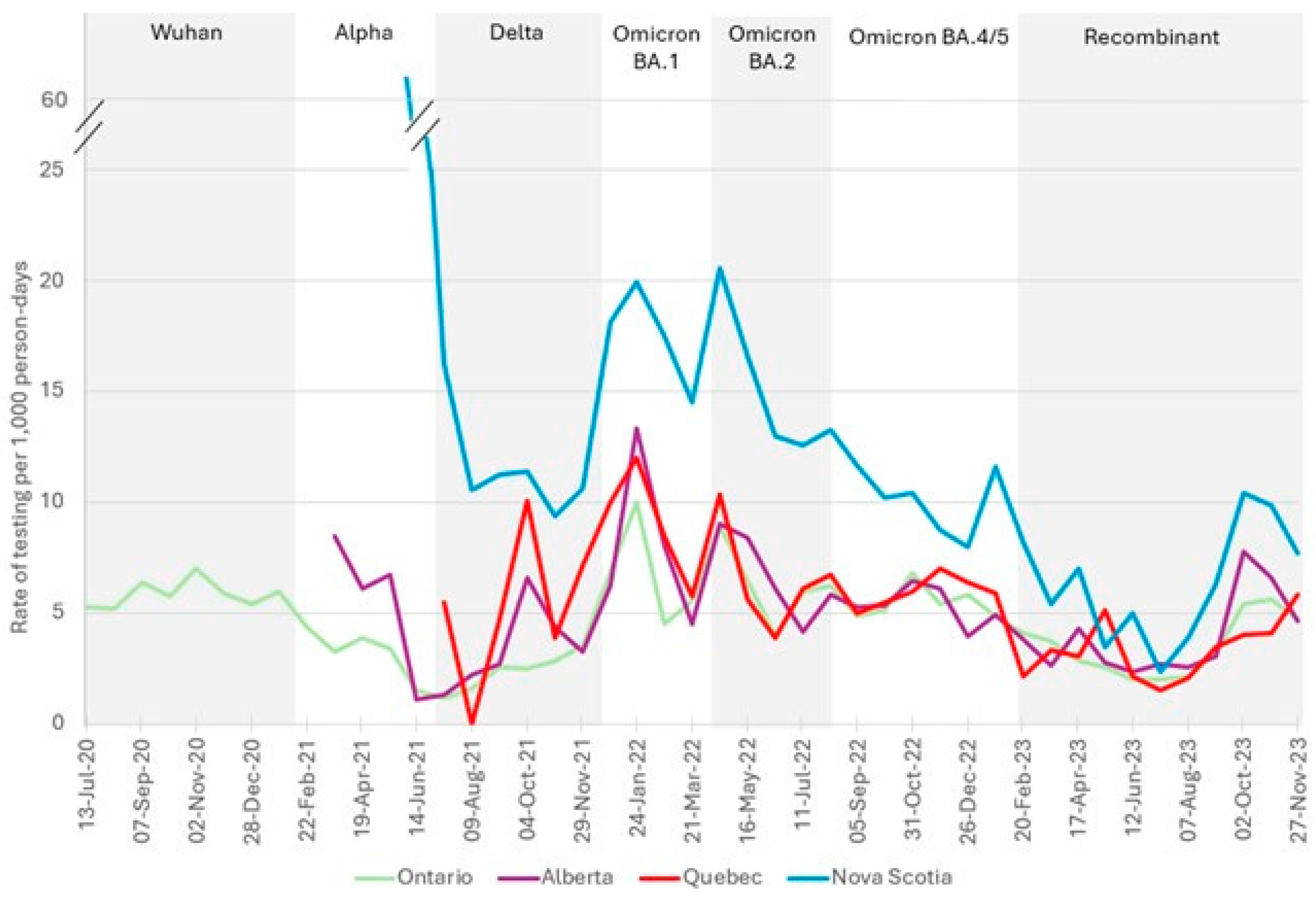
Figure 6.
Rates of re-testing for SARS-CoV-2 following an initial negative test result, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Percentage of participants within each four-week period.
Figure 6.
Rates of re-testing for SARS-CoV-2 following an initial negative test result, Canadian healthcare workers participating in the COVID-19 Cohort Study, June 2020-November 2023. Percentage of participants within each four-week period.
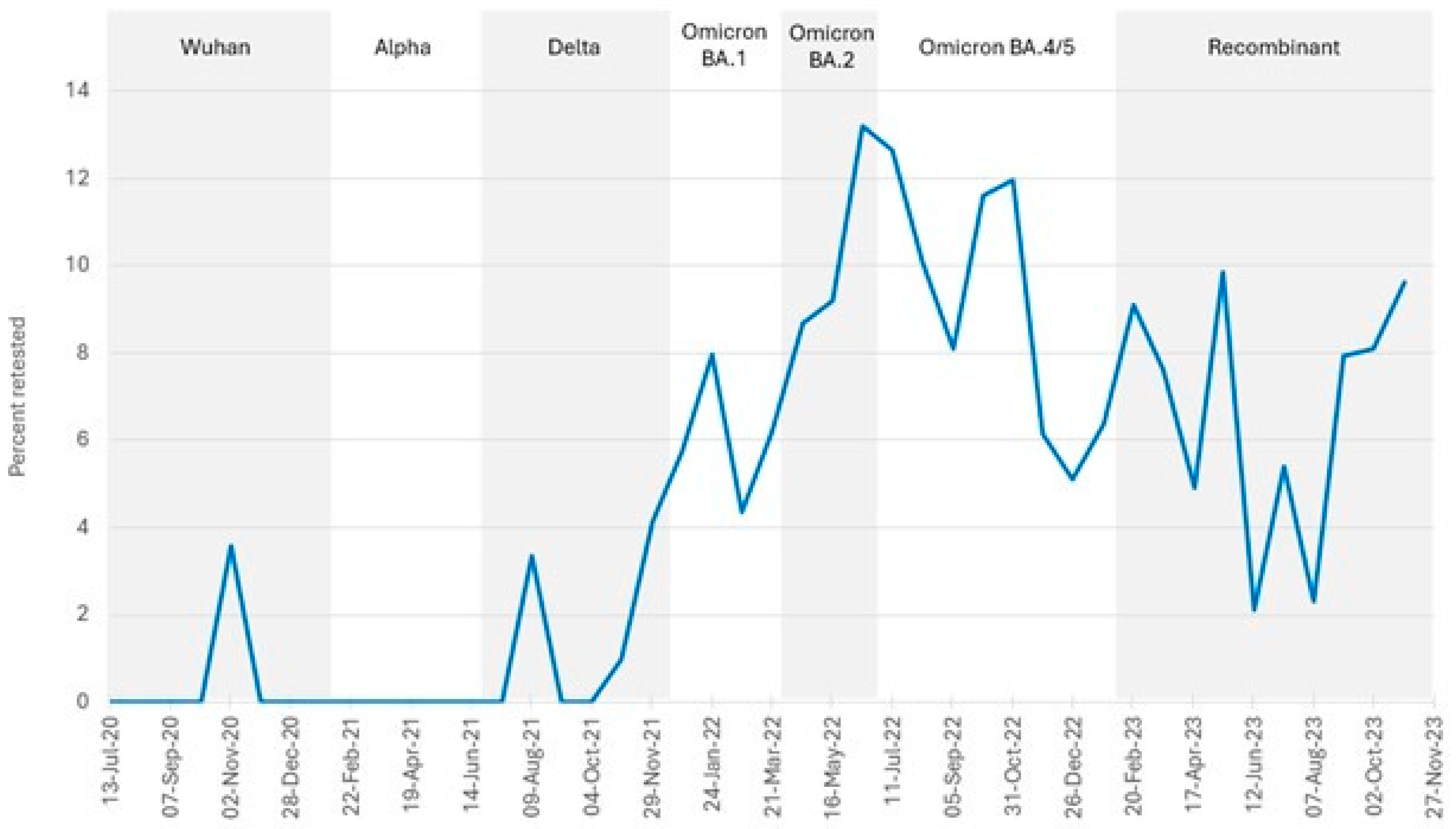

Table 1.
Characteristics of Canadian healthcare workers at enrolment; COVID-19 Cohort Study (June 2020-November 2023), Number (percent) unless otherwise noted.
Table 1.
Characteristics of Canadian healthcare workers at enrolment; COVID-19 Cohort Study (June 2020-November 2023), Number (percent) unless otherwise noted.
| Characteristic | Participants N = 2535 |
|---|---|
| Age in years, median (95% CI) | 40 (39, 41) |
| Gender | |
| Female | 2162 (85.3) |
| Male | 364 (14.4) |
| Other | 9 (0.4) |
| Occupation | |
| Nurse/nurse practitioner/midwife | 833 (32.9) |
| Physician/physician assistant | 273 (10.8) |
| Other regulated health worker1 | 741 (29.2) |
| Other2 | 688 (27.1) |
| Province | |
| Ontario | 1538 (60.7) |
| Alberta | 460 (18.1) |
| Nova Scotia | 226 (8.9) |
| Quebec | 311 (12.3) |
CI: confidence interval. 1 Respiratory therapist, laboratory technician, physical therapist, occupational therapist, imaging technician/technologist, pharmacist, pharmacy technician, psychologist, social worker. 2 Food service, ward clerk, administration, healthcare aids, housekeeper, porter, research, other clinical support.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



