Submitted:
22 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Despite their increasing prevalence epidemiological data on thoracic spine injuries(TSI) is under-presented in the literature. Furthermore, these studies fail to correlatemechanisms of injury to the specific spinal regions injured. Team ball sports appear tobe common activities undertaken in these age groups. A narrative review wasconducted to understand the aetiology of traumatic TSI, with a focus on sporting causes in youth populations. A literature search was conducted through various databases (from inception to April 2024) such as PubMed, CINAHL, Medline, ProQuest Central, Science Direct and SPORTDiscus. Seven studies, including 1670 patients were included in the dataset. TSI, particularly fractures, were found to be more common in adolescent age groups. Common sporting causes of spinal trauma included equestrian and team ball/contact sports. This review found few studies failed to correlate the mechanism of injury and the specific spinal level affected, supporting the need for further research.
Keywords:
Background
Research Question and Objectives
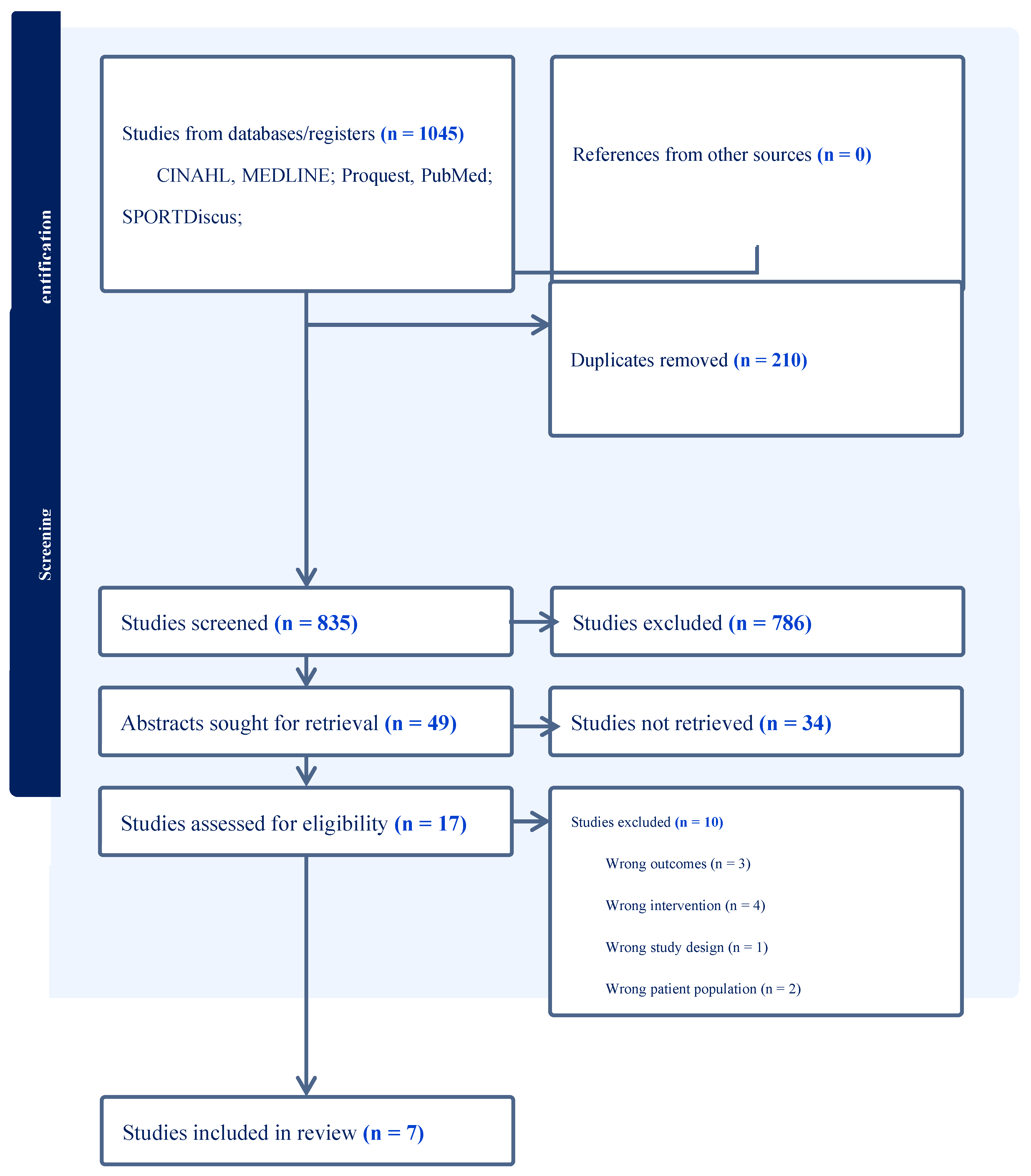
Methods
Results
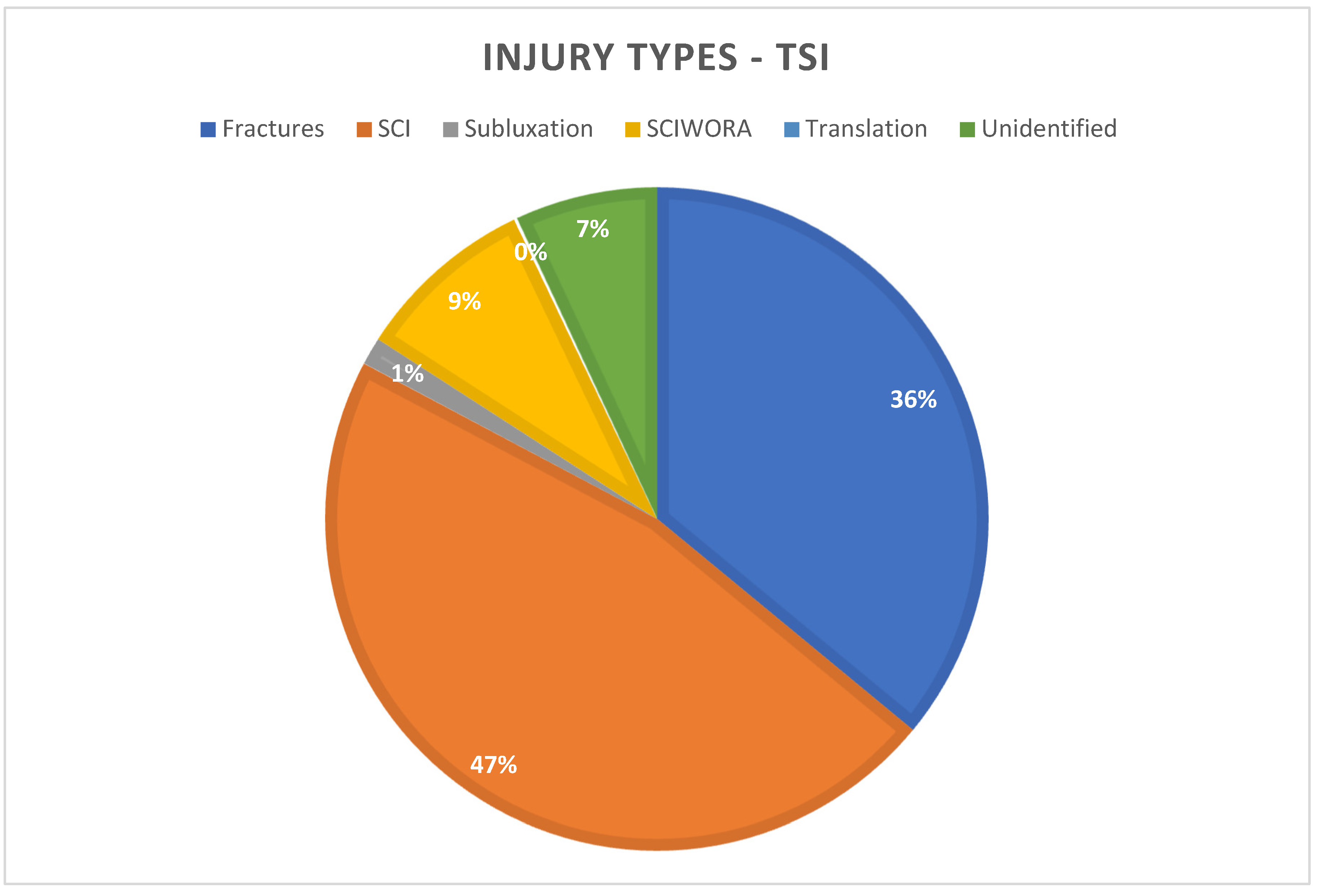
Injury Types
Paediatric Injuries
Injury Aetiology and Mechanism
Imaging
Discussion
Summary
Limitations
Conclusion
Funding
Disclosure Statement
References
- Bae SW, Shin HI, Bang MS, Lee MY. Epidemiology of Work-Related Traumatic Spinal Cord Injury: An Analysis of Workers’ Compensation Claims in Korea, 2011-2019. J Occup Environ Med. 2023 Jul 1;65(7):e453-e457. [CrossRef] [PubMed] [PubMed Central]
- McGuinness MJ, Isles S, Xu W, Harmston C. Incidence and outcomes of major trauma patients with thoracic injuries and rib fractures in Aotearoa New Zealand. Injury. 2023 Sep;54(9):110787. [CrossRef] [PubMed]
- Yadollahi M, Karajizadeh M, Bordbar N, Ghahramani Z. Incidence and pattern of traumatic spine injury in a single level I trauma center of southern Iran. Chin J Traumatol. 2023 Jul;26(4):199-203. [CrossRef] [PubMed] [PubMed Central]
- Crain J, McFaull S, Thompson W, Skinner R, Do MT, Fréchette M, Mukhi S. Status report - The Canadian Hospitals Injury Reporting and Prevention Program: a dynamic and innovative injury surveillance system. Health Promot Chronic Dis Prev Can. 2016 Jun;36(6):112-7. Erratum in: Health Promot Chronic Dis Prev Can. 2016 Jul;36(7):140. [CrossRef] [PubMed] [PubMed Central]
- Risetti M, Gambugini R, Testa M, Battista S. Management of non-specific thoracic spine pain: a cross-sectional study among physiotherapists. BMC Musculoskelet Disord. 2023 May 19;24(1):398. [CrossRef] [PubMed] [PubMed Central]
- Neck and Upper Back Claims [Internet]. New Zealand Government [updated 2023 January 10; cited 2024 April 10]. Available from: https://catalogue.data.govt.nz/dataset/ce6c5fb9-b97a-4681-8655-dda8d79f0620/resource/30d2c081-acb6-4c92-b2c6-e3e60b6392ec/download/ar-3572-response.xlsx.
- Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. Erratum in: Spine J. 2014 Aug 1;14(8):A18. Lebl, Darren S [corrected to Lebl, Darren R]. [CrossRef] [PubMed]
- Leucht P, Fischer K, Muhr G, Mueller EJ. Epidemiology of traumatic spine fractures. Injury. 2009 Feb;40(2):166-72. [CrossRef] [PubMed]
- Gupta S, Hauser BM, Zaki MM, Xu E, Cote DJ, Lu Y, Chi JH, Groff M, Khawaja AM, Harris MB, Smith TR, Zaidi HA. Morbidity after traumatic spinal injury in pediatric and adolescent sports-related trauma. J Neurosurg Spine. 2019 Dec 27;32(5):642-648. [CrossRef] [PubMed] [PubMed Central]
- Compagnon R, Ferrero E, Leroux J, Lefevre Y, Journeau P, Vialle R, Glorion C, Violas P, Chalopin A, Odent T, Haddad E, Nallet J, Garin C, Choufani E, Langlais T, Sales de Gauzy J; French Society of Spinal Surgery (SFCR), French Society of Pediatric Orthopedics (SOFOP). Epidemiology of spinal fractures in children: Cross-sectional study. Orthop Traumatol Surg Res. 2020 Nov;106(7):1245-1249. [CrossRef] [PubMed]
- Herren C, Jarvers JS, Jung MK, Blume C, Meinig H, Ruf M, Weiß T, Rüther H, Welk T, Badke A, Gonschorek O, Heyde CE, Kandziora F, Knop C, Kobbe P, Scholz M, Siekmann H, Spiegl U, Strohm P, Strüwind C, Matschke S, Disch AC, Kreinest M; Pediatric Spinal Trauma Working Group, Spine Section of the German Society for Orthopaedics, Trauma (DGOU). Paediatric spine injuries in the thoracic and lumbar spine-results of the German multicentre CHILDSPINE study. Eur Spine J. 2024 Apr;33(4):1574-1584. [CrossRef] [PubMed]
- An S, Hyun SJ. Pediatric Spine Trauma. J Korean Neurosurg Soc. 2022 May;65(3):361-369. [CrossRef] [PubMed] [PubMed Central]
- Falavigna A, Righesso O, Guarise da Silva P, Sanchez Chavez FA, Sfreddo E, Pelegrini de Almeida L, Valencia Carrasco MJ, Joaquim AF. Epidemiology and Management of Spinal Trauma in Children and Adolescents. [CrossRef] [PubMed]
- Leventer L, Dicks M, Duarte R, Davids K, Araújo D. Emergence of contact injuries in invasion team sports: an ecological dynamics rationale. Sports Med. 2015 Feb;45(2):153-9. [CrossRef] [PubMed]
- Eime RM, Harvey JT, Charity MJ, Payne WR. Population levels of sport participation: implications for sport policy. BMC Public Health. 2016 Aug 9;16:752. [CrossRef] [PubMed] [PubMed Central]
- Hulteen RM, Smith JJ, Morgan PJ, Barnett LM, Hallal PC, Colyvas K, Lubans DR. Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Prev Med. 2017 Feb;95:14-25. [CrossRef] [PubMed]
- Chan CW, Eng JJ, Tator CH, Krassioukov A; Spinal Cord Injury Research Evidence Team. Epidemiology of sport-related spinal cord injuries: A systematic review. J Spinal Cord Med. 2016 May;39(3):255-64. [CrossRef] [PubMed] [PubMed Central]
- Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009 Jun;26(2):91-108. [CrossRef] [PubMed]
- Green BN, Johnson CD, Adams A. Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. J Chiropr Med. 2006 Autumn;5(3):101-17. [CrossRef] [PubMed] [PubMed Central]
- Rozas LW, Klein WC. The value and purpose of the traditional qualitative literature review. J Evid Based Soc Work. 2010 Oct;7(5):387-99. [CrossRef] [PubMed]
- Al-Habib A, Alaqeel A, Marwa I, Almohammadi M, Al Shalaan H, AlEissa S, Zamakhshary M, Al-Bedah K, Al-Enazi S, Mukhtar F. Causes and patterns of spine trauma in children and adolescents in Saudi Arabia: implications for injury prevention. Ann Saudi Med. 2014 Jan-Feb;34(1):31-7. [CrossRef] [PubMed] [PubMed Central]
- Babu RA, Arimappamagan A, Pruthi N, Bhat DI, Arvinda HR, Devi BI, Somanna S. Pediatric thoracolumbar spinal injuries: The etiology and clinical spectrum of an uncommon entity in childhood. Neurol India. 2017 May-Jun;65(3):546-550. [CrossRef] [PubMed]
- Boran S, Lenehan B, Street J, McCormack D, Poynton A. A 10-year review of sports-related spinal injuries. Ir J Med Sci. 2011 Dec;180(4):859-63. [CrossRef] [PubMed]
- Mitchell J, Nunnerley J, Frampton C, Croot T, Patel A, Schouten R. Epidemiology of traumatic spinal cord injury in New Zealand (2007-2016). N Z Med J. 2020 Feb 7;133(1509):47-57. [PubMed]
- Payr S, Schuller A, Dangl T, Chocholka B, Binder H, Tiefenboeck TM. Spine Fractures in Children and Adolescents-Frequency, Causes, Diagnostics, Therapy and Outcome-A STROBE-Compliant Retrospective Study at a Level 1 Trauma Centre in Central Europe. Children (Basel). 2021 Dec 3;8(12):1127. [CrossRef] [PubMed] [PubMed Central]
- Reddy SP, Junewick JJ, Backstrom JW. Distribution of spinal fractures in children: does age, mechanism of injury, or gender play a significant role? Pediatr Radiol. 2003 Nov;33(11):776-81. [CrossRef] [PubMed]
- Ye C, Sun T, Li J, Zhang F. Pattern of sports- and recreation-related spinal cord injuries in Beijing. Spinal Cord. 2009 Dec;47(12):857-60. [CrossRef] [PubMed]
- The Global Value of Grassroots Rugby Report [Internet]. World Rugby [updated 2023 October 26; cited 2024 April 19]. Available from: https://www.world.rugby/news/885796.
- Compagnon R, Ferrero E, Leroux J, Lefevre Y, Journeau P, Vialle R, Glorion C, Violas P, Chalopin A, Odent T, Haddad E, Nallet J, Garin C, Choufani E, Langlais T, Sales de Gauzy J; French Society of Spinal Surgery (SFCR), French Society of Pediatric Orthopedics (SOFOP). Epidemiology of spinal fractures in children: Cross-sectional study. Orthop Traumatol Surg Res. 2020 Nov;106(7):1245-1249. [CrossRef] [PubMed]
- Carroll T, Smith CD, Liu X, Bonaventura B, Mann N, Liu J, Ebraheim NA. Spinal cord injuries without radiologic abnormality in children: a systematic review. Spinal Cord. 2015 Dec;53(12):842-8. [CrossRef] [PubMed]
- Akin D, Sisiopiku VP, Alateah AH, Almonbhi AO, Al-Tholaia MMH, Al-Sodani KAA. Identifying Causes of Traffic Crashes Associated with Driver Behavior Using Supervised Machine Learning Methods: Case of Highway 15 in Saudi Arabia. Sustainability [Internet]. 2022;14(24):16654. [CrossRef]
- Karul M, Bannas P, Schoennagel BP, Hoffmann A, Wedegaertner U, Adam G, Yamamura J. Fractures of the thoracic spine in patients with minor trauma: comparison of diagnostic accuracy and dose of biplane radiography and MDCT. Eur J Radiol. 2013 Aug;82(8):1273-7. [CrossRef] [PubMed]
- Lee YW, Jang JH, Kim JJ, Lim YS, Hyun SY, Yang HJ. The Value of X-ray Compared with Magnetic Resonance Imaging in the Diagnosis of Traumatic Vertebral Fractures. J Trauma Inj. 2017;30(4):158-165. [CrossRef]
- Earl VJ, Potter AOG, Perdomo AA. Effective doses for common paediatric diagnostic general radiography examinations at a major Australian paediatric hospital and the communication of associated radiation risks. J Med Radiat Sci. 2023 Mar;70(1):30-39. [CrossRef] [PubMed] [PubMed Central]
- Sirén A, Nyman M, Syvänen J, Mattila K, Hirvonen J. Emergency MRI in Spine Trauma of Children and Adolescents-A Pictorial Review. Children (Basel). 2023 Jun 21;10(7):1094. [CrossRef] [PubMed] [PubMed Central]

| Phase 1 | Phase 2 | Phase 3 | Phase 4 |
|
|
|
|
| Author, year | Design | Study characteristics | Main Findings | Study Limitations |
|---|---|---|---|---|
| Al-Habib et al., 2014 | Retrospective | Traumatic spinal injuries in patients under 19 years of age at Medical centre between May 2001 and May 2009. 120 patients were included, making up 141 spinal fractures. The mean age was 13.5 years. |
MVC was the most common injury aetiology at 60.8%, followed by pedestrian injuries at 90.8%, then fall related injuries at 15%. MVC injuries were most commonly seen in 12-18 year olds. Falls and pedestrian related injuries were seen in children under 12. Overall, cervical injuries were most common 55.8%. Thoracic injury was most common in 12-18 years. 19.2% suffered SCI. The average age was 13.7 years. Thoracic SCI was most common. |
Unable to define “Traumatic Spine Injury” Single centre study Patient population did not include minor injuries |
| Babu et al., 2017 | Retrospective |
Children with thoracolumbar trauma (fractures, dislocations, discoligamentous lesions and/or spinal cord injuries) occurring between 2002 and 2014, aged under 18 years. 90 children with thoracolumbar spine injuries were included. The mean age was 15.9 years. |
71.1% were inured falling from a height, 20% from MVA, 6.7% following fall of a heavy object , 1.1% from trivial fall, and 1.1% diving from diving. 34.4% of injuries occurred in the thoracic spine. These were most commonly fractures, followed by subluxation and SCIWORA. The lumbar spine was the most common level injured making up 53.3% on injuries. 81% of TL injuries occurred in the 15-18 age group. 23.1% had SCI. These were mostly graded Frankel A. |
Unable to break down age, gender and mechanism into spinal segment injured. Single centre study Retrospective |
| Boran et al., 2011 | Prospective | Examined all patients admitted under The National Spinal Injuries Centres between 1993 and 2003. 196 spinal injuries were admitted. This included 145 males and 51 females, with an average age of 30.2 years, extending from 14 to 72 years. |
Sports related spinal injuries made up 11% of all admitted spinal injuries. Equestrian injuries made up 41.8% of all injuries, followed by rugby 16.3%, diving 15.3%. 60% are injuries occurred in the cervical spine, 21% in the thoracic and 19% in the lumbar spine. In 40% of patients more than one vertebral level was injured, and in 9.25% more than one region was injured. Neurological injury was seen in 36% of patients, 65% of these were incomplete and 25 complete |
Did not directly assess paediatric population. Unable to break down injuries into specific injuries |
| Mitchell et al., 2020 | Retrospective | Retrospective data from Auckland Spinal Rehabilitation Unit and Burwood Spinal Unit over 10 years was examined. 929 patients, over the age of 16 were included. The mean age was between 43 to 48. |
The highest incidence of TSCI was in Māori. Transport accounted for 32% of injuries, falls 31% and sports 21%. MVA and sports causes were more common in younger age groups. Team ball sports was the most common sporting cause making up 20% of sporting injuries. In the 16-30 year old age group, team ball sports caused 31% of sporting spinal injuries. Cervical TSCI made up 54% of injuries, thoracic 28% and lumbosacral 18%. Thoracic injury was most common in 16 – 45 year olds. Cervical TSCI was more common in older age groups. |
Age group 16 and above. Failed to break down common aetiologies for each spinal region. Retrospective |
| Payr et al., 2021 | Retrospective epidemiological | Evaluation of patients aged 0 to 18 years with spinal fractures, presenting to a level 1 trauma centre between January 2002 to December 2021 144 patients with a mean age of 14.5 years, and 269 fractures were included. The population consisted of 40.3% female and 59.7% male |
52.8% of fractures occurred in the 16 to 18 year aged group. Falls from a height caused 45.8% or fractures, followed by sport incidents causing 29.9%, then road accidents at 20.8%. Skiing was the most common sporting cause of injury. Sporting injuries increased between 2002 and 2019. The thoracic spine was the most common fracture site, followed by lumbar then cervical. L1 was the most commonly injured vertebra. 5.6% of patient present with neurological deficits, this was most common in adolescents and sporting injuries |
Single centre study Retrospective Limited to fractures only Failed to break down common aetiologies for each spinal region fractured. |
| Reddy et al., 2003 | Retrospective | Patients under 18 years of age with a vertebral fracture and/or a neurological injury that were referred to Spectrum Health trauma service between 1996 and 2001. There were 134 patients; 84 patients with vertebral fractures and 50 neurological injury without radiographic abnormality included. The average age was 16 years. There were 56 males and 28 females. |
Thoracic fractures made up the majority of fractures 28.7%, followed by lumbar 23.2% and mid-cervical 18.9%. The thoracolumbar junction (T11-L1) made up 18.9%, the cervicothoracic junction (C7-T1) 7.9% and C0-C2 6.7%. Thoracic fractures were most common in the 9-14 year old age group, closely followed by 15 -17 year olds. MVA incidents accounted for 83 injuries. Thoracic fractures were most common in the MVA and non-MVA group. Neurological injury without fracture was most common in the 0-8 age group. |
Failed to break down common aetiologies for each spinal region fractured, only MVA and non-MVA. Neurological injury levels were not outlined. Single centre study Retrospective |
| Ye et al., 2009 | Retrospective | Patients with sports and recreation related SCI presenting to six institutions between 1993 and 2006 were examined. 57 patients were included in the population. The mean age was 24.5 years. 77.2% were males and 22.8% were females. |
64.7% occurred from water sports, 35.1% other incidents. 63.2% of injuries occurred in 12-29 age group. Cervical cord injuries made up 89.5% of injuries, and thoracic 10.5%. Diving caused 59.6% of water based SCI. Dancing was the most common cause of thoracic SCI, ranging from T9 to T12. ASIA A injuries made up 56.1% of injuries. |
Small population size Retrospective |
| MVA | Road incidents/transport (MVA and pedestrian) | Pedestrian | Falls | Sports | Other or unspecified | |
| Al-Habib et al., 2014 | 60.8% | 20.80% | 15% | 3.4% | ||
| Babu et al., 2017 | 20% | 73.30% | 6.6% | |||
| Boran et al., 2011 | 100% | |||||
| Mitchell et al., 2020 | 32% | 31% | 21% | |||
| Payr et al., 2021 | 20.8% | 45.8% | 29.9% | 3.5% | ||
| Reddy et al., 2003 | 61.9% | 4.5% | 11.2% | 11.9% | 11.9% | |
| Ye et al., 2009 | 100% |
| Team ball/contact | Wheeled non-motor | Water sports | Wheeled motor | Ice/Snow | Equestrian | Gymnastics/acrobatics/dancing | Other | |
| Boran et al., 2011 | 24.4% (48) | 4.2% (8) | 15.3% (30) | 3.5% (6) | 1.2% (2) | 41.8% (82) | 0.6% (1) | 12% (20) |
| Mitchell et al., 2020 | 20% (36) | 18% (32) | 18% (32) | 11% (19) | 9% (15)% | 7% (13) | 18% (30) | |
| Payr et al., 2021 | 21% (9) | |||||||
| Reddy et al., 2003 | 40% (4) | 60% (6) | ||||||
| Ye et al., 2009 | 7% (4) | 64.9% (37) | 1.75% (1)% | 17.8% (10) | 8.8% (5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



