
Submitted:
13 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
Ankle sprains are exceedingly common injuries in both athletes and general population. They account for 10 to 30% of all sports injuries. Although the vast majority of lateral ankle ligamentous injuries respond successfully to conservative management, the absolute number of those that progress to chronic lateral ankle instability (CLAI) remains considerably important. This condition is characterized by persistent symptoms and may be associated with short-term and long-term complications and functional deficits. There is still a lack of ideal postoperative management of CLAI patients. Furthermore, an evidence-based rehabilitation phasing does not exist and most of the published studies regarding this subject suggest some protocols based on a wide variety of functional assessment scores and other modalities which are not accurate enough. Moreover, the literature that assesses the ability to return to work (RTW) and return to sport (RTS) in general population and athletes operated for CLAI shows most commonly aggregated results with global rates of RTW or RTS without describing a detailed timeline based on the readiness of patients to return to each level of activity. Although stress radiographs and MRI have been assessed as potential tools to improve postoperative management of CLAI patients, the first modality is limited by its low sensitivity to detect laxity and the second one by its static character and its inability to predict the healing process phase nor the mechanical properties of the repaired/reconstructed ligaments. Bioelectrical impedance, mechanical impedance and near-infrared spectroscopy are non-invasive methods of measurement that could be potential assessment tools to help surgeons improve the postoperative management of patients after CLAI surgery.
Keywords:
ankle instability
; chronic ankle instability
; postoperative management
; diagnostics
; NIRS
Introduction
Ankle sprains are exceedingly common injuries in both athletes and general population [1,2,3,4]. They account for 10% to 30% of all sports injuries [5]. Inversion-type is the most common mechanism of injury occurring in 80 to 90% of cases [3,5]. Although the vast majority of lateral ankle ligamentous injuries respond successfully to conservative management, 10% to 30% of patients may develop Chronic Lateral Ankle Instability (CLAI) [1,6]. This condition is characterized by persistent symptoms including pain, feeling of insecurity and sensation of giving way. Moreover, it may result in short and long-term functional deficits, with risk to other structures requiring surgical correction including osteochondral injuries and peroneal tendons pathology [5,7]. There is a variety of surgical procedures intended to address CLAI ranging from ligament repair to reconstructions using auto- or allograft tissue in order to replace torn ligaments [2,5,8,9,10]. Currently, there is still a lack of uniform phasing or even individualized protocol for rehabilitation of patients following CLAI surgery regarding weight bearing, Return To Work (RTW) and Return To Sport (RTS) [3,11]. As shown by Clements et al. in their systematic review [11], the postoperative outcomes in most studies are being measured using a variety of objective and subjective functional assessment scores and questionnaires, Range Of Motion (ROM) on physical examination and stress radiographs. However, these outcomes measurement methods do not reflect the histologic stage of the healing process of the repaired/reconstructed ligaments nor the mechanical stability of the ankle joint except for stress radiographs which are limited by their low sensitivity [2,7,12,13]. The aim of this article is to review and assemble the most important and recent literature on CLAI and to suggest possible methods that can guide the surgeons in the future to better manage CLAI patients postoperatively by providing precise data concerning the healing process of tissue and the stability of ankle joint reflecting the ability to RTS.
Overview of ankle lateral ligamentous anatomy
As shown in Figure 1, 3 ligaments compose the lateral ligament complex of the ankle: Anterior TaloFibular Ligament (ATFL), Posterior TaloFibular Ligament (PTFL) and CalcaneoFibular Ligament (CFL) [5,14]. ATFL is formed by a superior intra-articular and inferior extra-articular fascicles. The inferior fascicle shares its fibular insertion with the CFL and both are connected together by the arciform fibers. Thus, they are sometimes also referred to as the lateral fibulotalocalcaneal ligament complex [5,15,16].
Given the aforementioned findings, the ATFL provides restraint to talar translation in the sagittal plane as well as talar rotation in the axial plane, while the CFL controls talar and calcaneal inversion [2].Moreover, evidence from biomechanical studies shows that CFL contributes to subtalar joint stability, but thethe talocalcaneal ligaments do not provide stability to the ankle joint [2,17,18]. It was also observed that maximal tensile force of ATFL occurs during ankle plantar flexion while for CFL, the maximal tensile force occurs during ankle dorsiflexion [2,19].
Mechanism of injury
The most common mechanism of acute ankle injury is a combination of inversion (Figure 2) and internal rotation forces associated with a plantar flexed or less frequently dorsiflexed foot [5]. The superior fascicle of ATFL is the weakest structure among the lateral ligaments of the ankle. It is the first ligament to be injured during ankle sprain [5,20,21]. In 65 to 80% of cases, there is an isolated rupture of the ATFL whereas a combined rupture of both ATFL and CFL (Figure 3) happens in around 20% of cases [5,20]. The PTFL is rarely injured during the abovementioned mechanism [21,22].
Diagnosis
Given that the purpose of this paper is to focus on the improvement of the postoperative management, the different aspects that should be addressed by anamnesis [7,23] and the clinical tests [5,7,23] that should be done in order to rule out other associated injuries with lateral ligamentous ruptures including osteochondral lesions, bone fractures and peroneal tendons lesions will not be detailed in this article. Special tests are usually used to help surgeons diagnose ankle instability. Typically, Anterior Drawer (AD) and Talar Tilt (TT) tests are used to assess the integrity of ATFL and CFL, respectively [2,5,7,23]. However, Van Dijk et al. considered that AD test may not be accurate because it applies isolated sagittal translation without taking into account the rotational laxity [24]. Phisitkul et al. described the AnteroLateral Drawer (ALD) testing in which the foot is allowed to internally rotate while translating it anteriorly, and they showed that ALD is a more accurate test than AD in detecting ATFL inefficiency [25]. Frey et al. compared Magnetic Resonance Imaging (MRI) results with physical examination findings and found that grade II lesions were most often underestimated by clinicians with an accuracy of only 25% in diagnosing those lesions [26]. Some authors suggested to delay the performance of physical examination in the acute setting in order to increase testing accuracy [24].
Imaging
Three imaging modalities have been classically used to help diagnose CLAI: stress radiographs, MRI and UltraSonography (US) [2]. While stress radiographs have been proposed as an objective tool to visualize the subjective findings of AD and TT tests, with established threshold values including 10mm anterior translation of talus for AD testing, and 10° tilt for TT testing. When performing comparative radiographs between the injured and the normal sides, a side to side difference of at least 5mm for AD or at least 5˚ for TT is required to support the diagnosis of lateral ankle instability [2]. In 1993, Peyre and Rodineau showed that auto-varus active stress radiographs may provide better results compared to passive testing realized manually or using a stress device [27]. However, the variety of measurement methods make the results difficult to exploit and until today the main limitation of stress radiographs remains their low sensitivity which is around 57% [2,5,7,23,27].
MRI is sensitive for identification of ligaments defects and ruptures, but its static nature prevents its ability to assess ligament function [2,5,28]. In their retrospective study, Jolman et al. compared the MRI findings of 112 patients operated for CLAI with those of 75 patients referred for other pathologies. The authors identified a high sensitivity but a relatively low specificity (53.3%) and concluded that MRI can be useful to identify associated extra and intra-articular lesions that can be associated with CLAI rather than being a primary tool to help establish the diagnosis of CLAI [28].
Ultrasonography (US) has showed its substantial accuracy with high sensitivity and specificity in detecting ATFL and CFL defects [2,5,29]. Dynamic US can be performed using stress maneuvers in order to assess lateral ankle stability in real time. Although favorable outcomes are being observed in some studies, further clinical and biomechanical studies are still necessary before validating it as a diagnostic tool for CLAI. Finally, useful data cannot be obtained with US unless it is performed by a skilled operator.
Surgical treatment
The surgical treatment of CLAI includes a number of procedures ranging from simple repair of the injured ligaments to reconstruction techniques. They can all be performed as open procedures or arthroscopically, and they can all be classified either as anatomic or non-anatomic techniques. Broström first described its anatomic open repair technique in 1966, consisting of tightening the ruptured lateral ligaments to the fibula [30]. Several modifications have been described subsequently including the Gould et al. procedure that comprised an additional step which is an augmentation of the repair using the inferior extensors retinaculum [31], then the Karlsson et al. modification that consisted of performing a shortening of the ligaments when they are elongated rather than disrupted [32]. The augmentation using non-absorbable suture-tape have been also advocated by some authors [5,33]. Non-anatomic reconstruction techniques involving tenodesis and including Chrisman-Snook, Evans and Watson-Jones procedures were initially introduced to replace the direct repair for cases with severely injured ligaments. However, they have been associated with many complications including decreased ROM, recurrent lateral ankle instability, osteoarthritis, and it was shown that they may compromise the normal joint biomechanics [2,5,34]. Anatomic reconstruction procedures involve direct reconstruction of the ATFL and CFL using either autografts (Figure 4), allografts or synthetic ligaments. They have showed positive results and superior outcomes compared with non-anatomic reconstruction [2,5,35]. Nowadays, arthroscopically-assisted and all-arthroscopic procedures are increasingly used for performing both repair and reconstruction with favorable outcomes in clinical studies. To our knowledge, we are still lacking high-level biomechanical evidence directly comparing arthroscopic versus open lateral ankle instability surgical techniques.
Postoperative rehabilitation and management
Postoperative rehabilitation is essential to achieve optimal functional outcomes without altering the stability of the ankle joint and increasing the risk of complications. However, we are still lacking uniform or optimal evidence-based rehabilitation protocols. In their systematic review including 14 articles with a total of 809 patients, Clements et al. showed that there is a wide variation of postoperative immobilization protocols as well as postoperative rehabilitation protocols [11]. The number of rehabilitation phases varied between 1 and 5, at times which even differed between groups within the same study. Given the available literature findings, they suggested a 4-phase protocol including progressive weight bearing, ROM, balance, proprioception and strengthening of peroneal muscles. The outcomes were measured based only on subjective functional assessments and objective outcome scores including, among others, the Foot and Ankle Ability Measure, the American Orthopedic Foot and Ankle Society questionnaire, the Karlsson Scoring, the Cumberland Ankle Instability Tool, and the Foot and Ankle Outcome Score.
In their systematic review including 1457 patients, Vopat et al. compared early and delayed postoperative mobilization protocols in patients after CLAI ligament repair surgery, and showed improved functional scores in early mobilization (EM) groups [4].However, anobjective radiographic laxity and higher complication rates were found in these patients. In a randomized study where EM after ligaments repair was defined as 7 to 10 days of plaster followed by an ankle brace, Karlsson et al. showed better functional outcomes in this group of patients compared with the delayed mobilization group, without noticing negative effects of EM on ankle stability [36]. Moreover, many surgeons are increasingly using anatomic reconstruction techniques with immediate weight bearing allowed postoperatively but there continues to be some debate on how to protect the reconstructed ligament if deemed necessary [2]. In a systematic review performed by Hunt et al. about the RTS following lateral ankle ligaments repair or reconstruction, it was shown that the literature is clearly deficient concerning the presence of a consistent timeline, with identification of a variety of metrics used for the measurement of outcomes, and those metrics were tracked in very few studies [3]. They mentioned that among 360 papers identified, only 5.5% detailed a return to play timeline. Furthermore, they observed that the studies generally reported aggregated mean time to RTS and that the variation of reported timelines depends on the injury patterns, the surgical technique, the type of sport, and the postoperative use of bracing. They concluded that there is still lack of a well-defined meaningful tool or protocol to assess the readiness and the ability of athletes to RTS.
Many authors proposed the use of MRI as a potential useful tool for the follow-up of CLAI patients postoperatively since the signal intensity reflects the water content of the tissue enabling the surgeons to track the graft healing process over time [16]. In order to increase the MRI effectiveness and reliability, some studies defined another MRI parameter taking into account the background signal in addition to signal intensity. This parameter is the signal to noise quotient (SNQ). It was initially used for graft maturity assessment in patients after anterior cruciate ligament (ACL) reconstruction. In fact, it has been demonstrated the presence of 3 stages of graft healing after ACL reconstruction: the early healing phase, then the proliferation phase followed by the ligamentization or maturation final stage [13]. In a systematic review performed to evaluate the possible relationships between histologic findings, SNQ and clinical outcomes in graft healing assessment after ACL reconstruction using autograft, Van Groningen et al concluded that the MRI SNQ does not predict neither graft maturity nor functional and clinical outcomes after ACL reconstruction [13]. Furthermore, they identified the presence of a heterogeneity of MRI methods used in the literature in addition to many technical restrictions.
According to all the aforementioned findings, we can consider that we are lacking meaningful, reliable and accurate modalities and methods that could help the surgeons improve the postoperative management of CLAI patients. Given the wide variety of the injury patterns and the surgical techniques described in the literature, in addition to the interindividual differences in the pain perception, we believe that we need to use objective and innovative outcome measurement modalities which may reflect more precisely the histological changes of tissue to track the healing process of the repaired/reconstructed ligaments and/or the mechanical stability of the ligaments and the ankle joint.
Alternative outcome monitoring methods in patients after CLAI surgery
Bioelectrical impedance (BEImp), mechanical impedance (MImp) and near-infrared spectroscopy (NIRS) are 3 non-invasive measurement methods that can be used to improve the postoperative management of CLAI patients.
Bioelectrical impedance spectroscopy measurement
Bioelectrical impedance (BEImp) represents a means for the assessment of the biological tissue composition by injecting an electrical current at defined frequencies and measuring the resultant voltage decrease across the biological sample (Figure 5). Impedance is a combination of 2 parameters: resistance and reactance. The former is the extent to which the current is limited when passing across the tested tissue while the latter represents the non-resistive imaginary component of impedance in an alternative current (AC) resulting from the effect of inductance or capacitance or both [37]. BEImp has been used in many medical fields, and recently we can find increasingly published studies evaluating its usefulness in assessment of tendons, ligaments and joints pathologies. Mabrouk et al. tracked ankle edema using BEImp [37]. They initially designed a wearable measurement system with a specific algorithm that allowed the mapping of the outputted raw values generated by an impedance analyzer into accurate real and imaginary impedance values. In order to allow this mapping to be more accurate through the range of the measured frequencies, they used the standard 2R1C electrical circuit model to represent the biological tissue. Given the frequency dependency of the penetration depth of current in tissue, they realized a differential measurement technique by moving the ankle through multiple positions. This method performed on cadaver models as well as on a cohort of patients showed favorable outcomes with low inter-individual and intra-individual variability. In an experimental study on rabbits, Yoon et al demonstrated that BEImp could be a useful modality to make the diagnosis of tendinitis [38]. They used the dissipation factor (D) to increase their results accuracy. This factor is defined as the resistance to reactance ratio (D= resistance/reactance), and it seems to be a very meaningful index because its standard deviation is one-tenth that of the resistance and it also reduces the interface problems that happen between the electrodes and tissues.
Mechanical impedance measurement
Mechanical impedance (MImp) represents the dynamic relationship between imposed deformations or motions and the resulting torques [39]. The estimates of MImp of a joint allow for the quantification of the mechanical properties of the tested joint (Figure 6). Given that the biomechanics of a joint are determined by the mechanical properties of the muscles and tendons spanning it, MImp could be a substantial modality to track the healing process and graft maturity in patients after CLAI surgery as well as the progression of mechanical stability and potential early postoperative laxity over time. Although the published studies classically measured the global joint MImp without taking into account the specific contribution from the tendon and muscle, there is actually recent evidence in the literature which supports our belief that MImp measurement may play an important role in the improvement of the postoperative management by helping surgeons to assess the readiness of patients and athletes to RTS. Jakubowski et al. developed an experimental model and analysis methods to quantify tendon, muscle and joint impedance by using an actuator with a single degree of freedom to impose pseudorandom rotations to the ankle while the corresponding torques were being measured [40]. At the same time, the displacement of the medial gastrocnemius muscle-tendon junction was measured using B-mode ultrasound. From these measurements, they were able to estimate the correspondent impedance values in addition to the assessment of the muscle and tendon stiffness.
Near-infrared spectroscopy (NIRS)
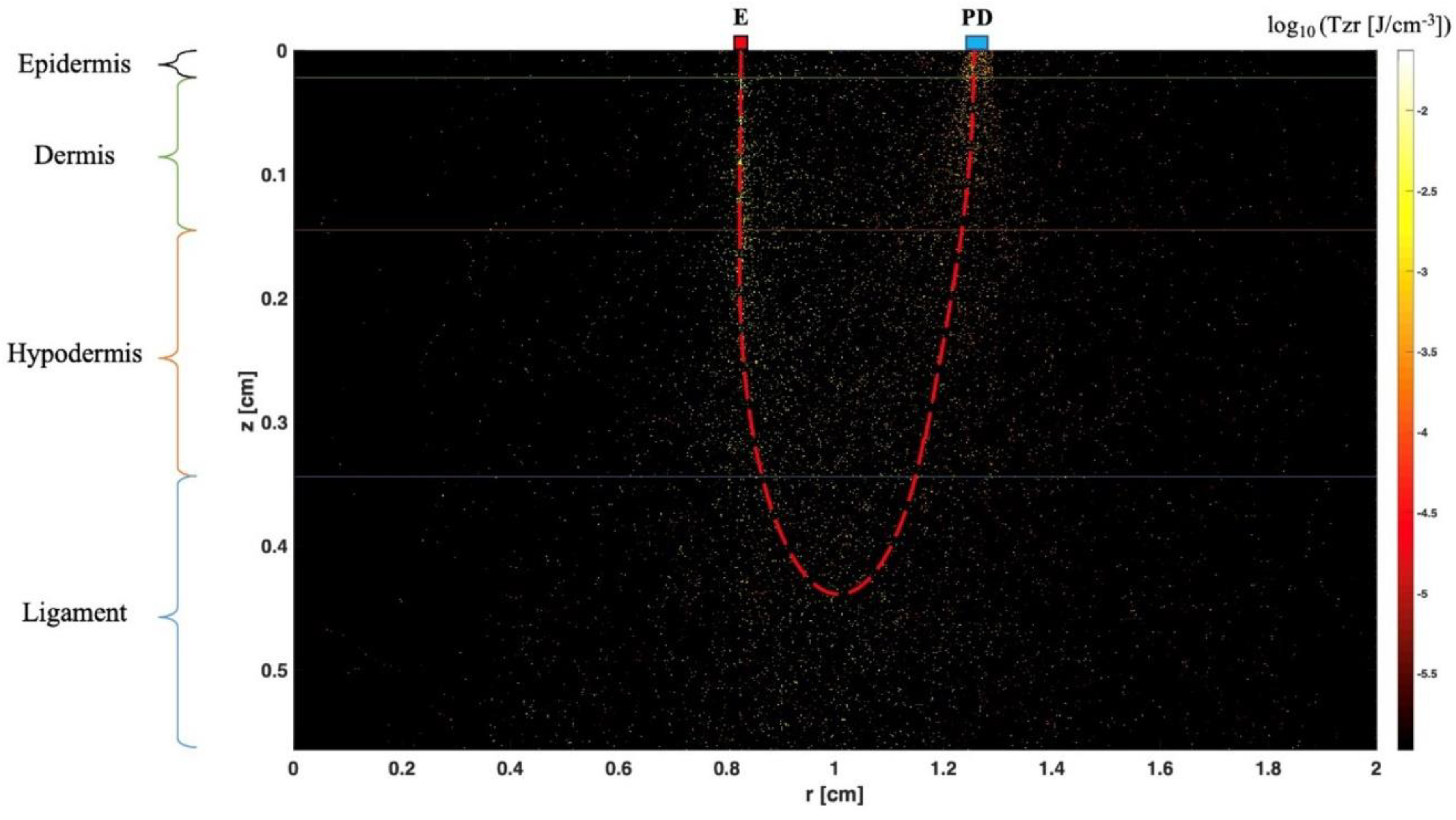
In 1977, F.F. Jöbsis first described the non-invasive in vivo application of NIRS by measuring the tissue oxygenation of tissue in real time [41]. His work was based on the principles of optical spectrophotometry. Technically, NIRS includes a light source defined as a light emitting diode (LED) and/or a laser diode, which covers the near-infrared (NIR) range of wavelengths between 650nm and 1000nm, and a detector. Flexible optic fibers are generally used in this method in order to transmit the light from the source and to the detectors (Figure 7). When NIR passes through a tissue, the light can be absorbed, reflected, scattered and transmitted. In fact, these physical phenomena occur simultaneously but at different extents depending on the emitted wavelength, the nature and heterogeneity of the tested tissue among other factors. Furthermore, NIRS can be used in transmission mode, reflection mode or both depending on the degree of transparency of the tested sample to NIR. It should be mentioned that NIRS has been used in many medical and biological fields including tissue oxygenation monitoring (central nervous system and somatic tissue), biological fluids and solutions composition analysis in addition to molecular structure and interaction analysis. Recent literature shows increasingly published studies describing the use of NIRS to characterize the optical parameters of human tissue including fibrous tissue like ligaments and tendons, and to estimate their mechanical properties [42,43]. In an experimental study, Torniainen et al. showed that NIRS can estimate the biomechanical properties of knee ligaments and patellar tendon [43]. In another experimental study of rat induced knee osteoarthritis model, Afara et al. demonstrated that NIRS data and spectral feedbacks enabled the separation of the cartilage samples relative to the severity of osteoarthritis with significant correlation between NIRS findings and the histologic Mankin score [44]. Finally, it should be noted that researchers can use sophisticated softwares which can allow tissue modeling and simulations performance that could help them estimate the possible pathways and penetration depth of the emitted photons [45].Thus, this allows for example to determine the ideal distance between light sources and detectors as well as the penetration depth of the light before the application of the technique on ex vivo and in vivo models (Figure 8).
Summary
- 1-
- Ankle sprain represents a frequent pathology among athletes and general population. Inversion-type is the most common mechanism of injury. Patients that do not respond to conservative management may develop CLAI.
- 2-
- CLAI is diagnosed following a thorough anamnesis, physical examination and medical imaging including stress radiographs, MRI and ultrasonography. AD testing is better to be replaced by ALD testing in clinical practice because it allows detection of both anteroposterior and rotational talar instability. Stress radiographs are limited by their low sensitivity. MRI may be better used to rule out injuries that could be associated with CLAI. Dynamic US is showing good outcomes in recent published studies, but these results are yet to be validated.
- 3-
- There is a wide variety of surgical procedures that address CLAI ranging from simple repairs to more complex reconstructions. Besides non-anatomic procedures which are increasingly abandoned due to their association with alteration of normal joint biomechanics, there is no superiority demonstrated of one technique over the others if the potential contraindications are taken into account.
- 4-
- The ideal postoperative management remains unknown. There is still a lack of accurate outcome assessment methods which can reflect the healing process histological stage and the mechanical stability of the repaired or reconstructed ligament. In most of the published studies regarding rehabilitation protocols and management of patients after CLAI surgery, the outcomes are being measured using a wide range of functional assessment scores and stress radiographs with the absence of meaningful, precise, reliable and uniform methods to assess those outcomes.
- 5-
- MRI is limited by its static character, and it seems that it cannot be a useful tool for postoperative management of patients after CLAI surgery because recent evidence showed that SNQ failed to predict the histological phase of the repaired or reconstructed healing ligament.
- 6-
- BEImp, MImp and NIRS are non-invasive robust measurement methods that have been used in many medical fields. Recent published literature shows the potential effectiveness and usefulness of these modalities in the assessment of ligament, tendon, cartilage and joint pathologies. We believe that larger high-quality studies should be performed to validate the accuracy of these methods separately or even simultaneously. This may represent in the future an important tool to help surgeons assess accurately the ability of the operated patients for CLAI to bear weight, and especially their readiness to RTW and RTS based on precise biomechanical data. Finally, these tools can be integrated in a wearable and easily portable device that could be used in the surgeon consultation room.
References
- Drakos M, Hansen O, Kukadia S. Ankle Instability. Foot Ankle Clin [Internet]. 2022 Jun;27(2):371–84. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1083751521001674. [CrossRef]
- Chang SH, Morris BL, Saengsin J, Tourné Y, Guillo S, Guss D, et al. Diagnosis and Treatment of Chronic Lateral Ankle Instability: Review of Our Biomechanical Evidence. J Am Acad Orthop Surg [Internet]. 2021 Jan 1;29(1):3–16. Available from: https://journals.lww.com/10.5435/JAAOS-D-20-00145. [CrossRef]
- Hunt KJ, Fuld RS, Sutphin BS, Pereira H, D’Hooghe P. Return to sport following lateral ankle ligament repair is under-reported: a systematic review. J ISAKOS [Internet]. 2017 Sep;2(5):234–40. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2059775421002492. [CrossRef]
- Vopat ML, Tarakemeh A, Morris B, Hassan M, Garvin P, Zackula R, et al. Early versus Delayed Mobilization Post-Operative Protocols for Primary Lateral Ankle Ligament Repair: A Systematic Review and Meta-analysis. Foot Ankle Orthop [Internet]. 2019 Oct 1;4(4):2473011419S0007. [CrossRef]
- Machado M, Amado P, Babulal J. Ankle instability – review and new trends. J Orthop Trauma Rehabil [Internet]. 2021 Jan 3;28:221049172110355. [CrossRef]
- Bestwick-Stevenson T, Wyatt LA, Palmer D, Ching A, Kerslake R, Coffey F, et al. Incidence and risk factors for poor ankle functional recovery, and the development and progression of posttraumatic ankle osteoarthritis after significant ankle ligament injury (SALI): the SALI cohort study protocol. BMC Musculoskelet Disord [Internet]. 2021 Dec 17;22(1):362. Available from: https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/s12891-021-04230-8. [CrossRef]
- Tourné Y, Besse J-L, Mabit C. Chronic ankle instability. Which tests to assess the lesions? Which therapeutic options? Orthop Traumatol Surg Res [Internet]. 2010 Jun;96(4):433–46. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1877056810000812. [CrossRef]
- Dromzée E, Granger B, Rousseau R, Steltzlen C, Stolz H, Khiami F. Long-Term Results for Treatment of Chronic Ankle Instability With Fibular Periosteum Ligamentoplasty and Extensor Retinaculum Flap. J Foot Ankle Surg [Internet]. 2019 Jul;58(4):674–8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1067251618305064. [CrossRef]
- Cho B-K, Kim Y-M, Shon H-C, Park K-J, Cha J-K, Ha Y-W. A Ligament Reattachment Technique for High-Demand Athletes With Chronic Ankle Instability. J Foot Ankle Surg [Internet]. 2015 Jan;54(1):7–12. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1067251614004372. [CrossRef]
- Porter DA, Kamman KA. Chronic Lateral Ankle Instability. Foot Ankle Clin [Internet]. 2018 Dec;23(4):539–54. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1083751518300561. [CrossRef]
- Clements A, Belilos E, Keeling L, Kelly M, Casscells N. Postoperative Rehabilitation of Chronic Lateral Ankle Instability: A Systematic Review. Sports Med Arthrosc [Internet]. 2021 Jun 1;29(2):146–52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/33972491. [CrossRef]
- Faure C, Deplus F, Besse JL, Moyen B, Bochu M. [Chronic external instability of the ankle. Contribution of dynamic radiographies, x-ray computed tomography and x-ray computed tomographic arthrography]. J Radiol [Internet]. 1997 Sep;78(9):629–34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9537181.
- van Groningen B, van der Steen MC, Janssen DM, van Rhijn LW, van der Linden AN, Janssen RPA. Assessment of Graft Maturity After Anterior Cruciate Ligament Reconstruction Using Autografts: A Systematic Review of Biopsy and Magnetic Resonance Imaging studies. Arthrosc Sport Med Rehabil [Internet]. 2020 Aug;2(4):e377–88. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2666061X20300158. [CrossRef]
- Schroeder JE, Barzilay Y, Hasharoni A, Kaplan L. Long-term outcome of surgical correction of congenital kyphosis in patients with myelomeningocele (MMC) with segmental spino-pelvic fixation. Evid Based Spine Care J [Internet]. 2011 Feb;2(1):17–22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22956932. [CrossRef]
- Vega J, Malagelada F, Manzanares Céspedes M-C, Dalmau-Pastor M. The lateral fibulotalocalcaneal ligament complex: an ankle stabilizing isometric structure. Knee Surg Sports Traumatol Arthrosc [Internet]. 2020 Jan;28(1):8–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30374570. [CrossRef]
- Umans H, Cerezal L, Linklater J, Fritz J. Postoperative MRI of the Ankle and Foot. Magn Reson Imaging Clin N Am [Internet]. 2022 Nov;30(4):733–55. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1064968922000393. [CrossRef]
- Brantigan JW, Pedegana LR, Lippert FG. Instability of the subtalar joint. Diagnosis by stress tomography in three cases. J Bone Joint Surg Am [Internet]. 1977 Apr;59(3):321–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/849942. [CrossRef]
- Tochigi Y, Amendola A, Rudert MJ, Baer TE, Brown TD, Hillis SL, et al. The role of the interosseous talocalcaneal ligament in subtalar joint stability. Foot ankle Int [Internet]. 2004 Aug;25(8):588–96. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15363382. [CrossRef]
- Ozeki S, Yasuda K, Kaneda K, Yamakoshi K, Yamanoi T. Simultaneous strain measurement with determination of a zero strain reference for the medial and lateral ligaments of the ankle. Foot ankle Int [Internet]. 2002 Sep;23(9):825–32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12356180. [CrossRef]
- Hintermann B, Boss A, Schäfer D. Arthroscopic Findings in Patients with Chronic Ankle Instability. Am J Sports Med [Internet]. 2002 May 30;30(3):402–9. [CrossRef]
- Vega J, Allmendinger J, Malagelada F, Guelfi M, Dalmau-Pastor M. Combined arthroscopic all-inside repair of lateral and medial ankle ligaments is an effective treatment for rotational ankle instability. Knee Surg Sports Traumatol Arthrosc [Internet]. 2020 Jan;28(1):132–40. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28983653. [CrossRef]
- Vega J, Peña F, Golanó P. Minor or occult ankle instability as a cause of anterolateral pain after ankle sprain. Knee Surgery, Sport Traumatol Arthrosc [Internet]. 2016 Apr 28;24(4):1116–23. Available from: http://link.springer.com/10.1007/s00167-014-3454-y. [CrossRef]
- Guillo S, Bauer T, Lee JW, Takao M, Kong SW, Stone JW, et al. Consensus in chronic ankle instability: Aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res [Internet]. 2013 Dec;99(8):S411–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S187705681300234X. [CrossRef]
- van Dijk CN, Lim LSL, Bossuyt PMM, Marti RK. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Jt Surg [Internet]. 1996 Nov 1;78(6):958–62. [CrossRef]
- Phisitkul P, Chaichankul C, Sripongsai R, Prasitdamrong I, Tengtrakulcharoen P, Suarchawaratana S. Accuracy of Anterolateral Drawer Test in Lateral Ankle Instability: A Cadaveric Study. Foot Ankle Int [Internet]. 2009 Jul 1;30(7):690–5. [CrossRef]
- Frey C, Bell J, Teresi L, Kerr R, Feder K. A Comparison of MRI and Clinical Examination of Acute Lateral Ankle Sprains. Foot Ankle Int [Internet]. 1996 Sep 21;17(9):533–7. [CrossRef]
- Peyre M, Rodineau J. L’auto varus: une technique d’exploration des instabilités externes de cheville. 3e Journées d’imagerie ostéo-articulaire de la Pitié Salpêtrière. Paris; 1993.
- Jolman S, Robbins J, Lewis L, Wilkes M, Ryan P. Comparison of Magnetic Resonance Imaging and Stress Radiographs in the Evaluation of Chronic Lateral Ankle Instability. Foot Ankle Int [Internet]. 2017 Apr 6;38(4):397–404. [CrossRef]
- Alshalawi S, Galhoum AE, Alrashidi Y, Wiewiorski M, Herrera M, Barg A, et al. Medial Ankle Instability. Foot Ankle Clin [Internet]. 2018 Dec;23(4):639–57. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1083751518300627. [CrossRef]
- Broström L. Sprained ankles. VI. Surgical treatment of “chronic” ligament ruptures. Acta Chir Scand [Internet]. 1966 Nov;132(5):551–65. Available from: http://www.ncbi.nlm.nih.gov/pubmed/5339635.
- Gould N, Seligson D, Gassman J. Early and Late Repair of Lateral Ligament of the Ankle. Foot Ankle [Internet]. 1980 Sep 17;1(2):84–9. [CrossRef]
- Karlsson J, Bergsten T, Lansinger O, Peterson L. Surgical treatment of chronic lateral instability of the ankle joint. Am J Sports Med [Internet]. 1989 Mar 23;17(2):268–74. [CrossRef]
- Viens NA, Wijdicks CA, Campbell KJ, LaPrade RF, Clanton TO. Anterior Talofibular Ligament Ruptures, Part 1. Am J Sports Med [Internet]. 2014 Feb 25;42(2):405–11. [CrossRef]
- Hunt KJ, Pereira H, Kelley J, Anderson N, Fuld R, Baldini T, et al. The Role of Calcaneofibular Ligament Injury in Ankle Instability: Implications for Surgical Management. Am J Sports Med [Internet]. 2019 Feb 20;47(2):431–7. [CrossRef]
- Camacho LD, Roward ZT, Deng Y, Latt LD. Surgical Management of Lateral Ankle Instability in Athletes. J Athl Train [Internet]. 2019 Jun 1;54(6):639–49. Available from: https://meridian.allenpress.com/jat/article/54/6/639/420901/Surgical-Management-of-Lateral-Ankle-Instability. [CrossRef]
- Karlsson J, Rudholm O, Bergsten T, Faxen E, Styf J. Early range of motion training after ligament reconstruction of the ankle joint. Knee Surgery, Sport Traumatol Arthrosc [Internet]. 1995 Sep;3(3):173–7. Available from: http://link.springer.com/10.1007/BF01565478. [CrossRef]
- Mabrouk S, Hersek S, Jeong HK, Whittingslow D, Ganti VG, Wolkoff P, et al. Robust Longitudinal Ankle Edema Assessment Using Wearable Bioimpedance Spectroscopy. IEEE Trans Biomed Eng [Internet]. 2020 Apr;67(4):1019–29. Available from: https://ieeexplore.ieee.org/document/8759081/. [CrossRef]
- Yoon K, Lee KW, Kim SB, Han TR, Jung DK, Roh MS, et al. Electrical impedance spectroscopy and diagnosis of tendinitis. Physiol Meas [Internet]. 2010 Feb 1;31(2):171–82. Available from: https://iopscience.iop.org/article/10.1088/0967-3334/31/2/004. [CrossRef]
- Ludvig D, Whitmore MW, Perreault EJ. Leveraging Joint Mechanics Simplifies the Neural Control of Movement. Front Integr Neurosci [Internet]. 2022 Mar 21;16. Available from: https://www.frontiersin.org/articles/10.3389/fnint.2022.802608/full. [CrossRef]
- Jakubowski KL, Ludvig D, Bujnowski D, Lee SSM, Perreault EJ. Simultaneous Quantification of Ankle, Muscle, and Tendon Impedance in Humans. IEEE Trans Biomed Eng [Internet]. 2022 Dec;69(12):3657–66. Available from: https://ieeexplore.ieee.org/document/9779431/. [CrossRef]
- Jöbsis FF. Noninvasive, Infrared Monitoring of Cerebral and Myocardial Oxygen Sufficiency and Circulatory Parameters. Science (80- ) [Internet]. 1977 Dec 23;198(4323):1264–7. [CrossRef]
- Fan C, Shuaib A, Yao G. Path-length resolved reflectance in tendon and muscle. Opt Express [Internet]. 2011 Apr 25;19(9):8879. Available from: https://opg.optica.org/oe/abstract.cfm?uri=oe-19-9-8879. [CrossRef]
- Torniainen J, Ristaniemi A, Sarin JK, Prakash M, Afara IO, Finnilä MAJ, et al. Near infrared spectroscopic evaluation of biochemical and crimp properties of knee joint ligaments and patellar tendon. Sakakibara M, editor. PLoS One [Internet]. 2022 Feb 14;17(2):e0263280. [CrossRef]
- Afara I, Prasadam I, Crawford R, Xiao Y, Oloyede A. Non-destructive evaluation of articular cartilage defects using near-infrared (NIR) spectroscopy in osteoarthritic rat models and its direct relation to Mankin score. Osteoarthr Cartil [Internet]. 2012 Nov;20(11):1367–73. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1063458412008837. [CrossRef]
- Wang L, Jacques SL, Zheng L. Conv—convolution for responses to a finite diameter photon beam incident on multi-layered tissues. Comput Methods Programs Biomed [Internet]. 1997 Nov;54(3):141–50. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0169260797000217. [CrossRef]
Figure 1.
This figure represents the lateral ankle ligament anatomy: superior (A) and inferior (B) bands of Anterior TaloFibular Ligament (ATFL), CalcaneoFibular (CF) ligament and Posterior TaloFibular Ligament (PTFL). ATIF= Anterior inferior TibioFibular ligament; PTIF= Posterior inferior TibioFibular ligament (This figure was created by the authors to be used in this paper).
Figure 1.
This figure represents the lateral ankle ligament anatomy: superior (A) and inferior (B) bands of Anterior TaloFibular Ligament (ATFL), CalcaneoFibular (CF) ligament and Posterior TaloFibular Ligament (PTFL). ATIF= Anterior inferior TibioFibular ligament; PTIF= Posterior inferior TibioFibular ligament (This figure was created by the authors to be used in this paper).
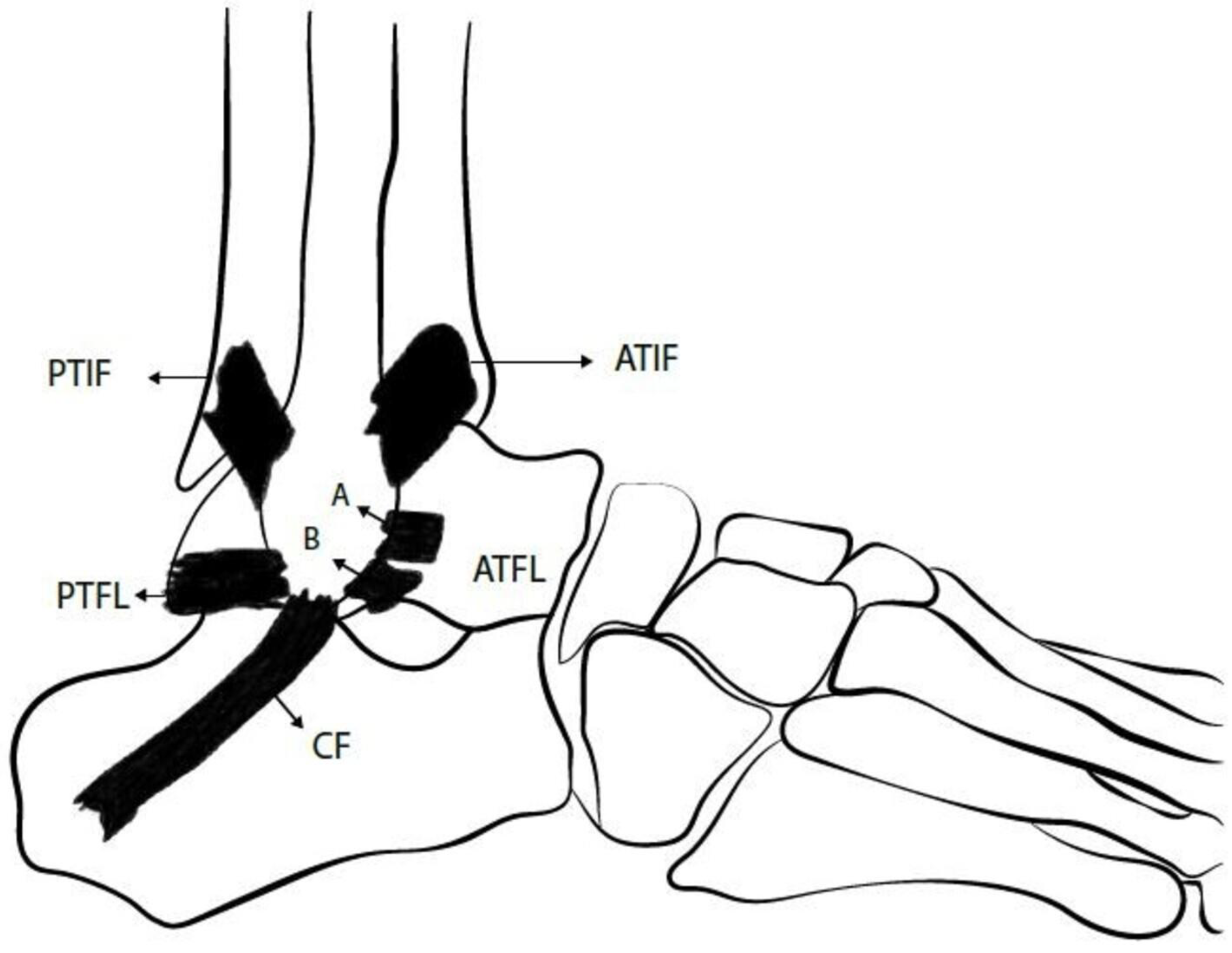
Figure 2.
The most common mechanism of injury in lateral ankle sprain is the inversion type (This figure was created by the authors to be used in this paper).
Figure 2.
The most common mechanism of injury in lateral ankle sprain is the inversion type (This figure was created by the authors to be used in this paper).
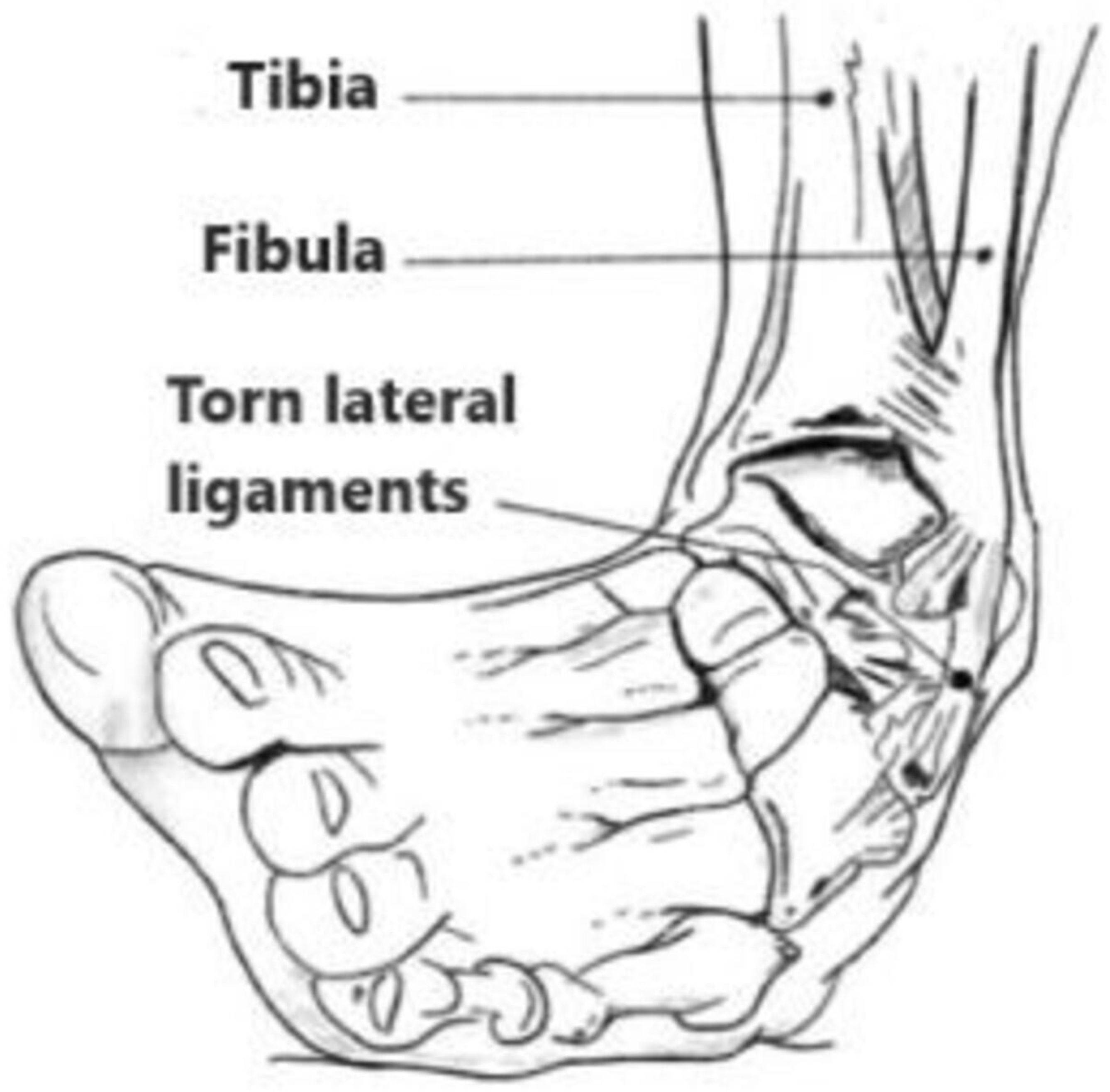
Figure 3.
This figure shows a combined rupture of both Anterior TaloFibular Ligament (ATFL) and CalcaneoFibular Ligament (CFL). This is found in about 20% of patients with lateral ankle instability (This figure was created by the authors to be used in this paper).
Figure 3.
This figure shows a combined rupture of both Anterior TaloFibular Ligament (ATFL) and CalcaneoFibular Ligament (CFL). This is found in about 20% of patients with lateral ankle instability (This figure was created by the authors to be used in this paper).
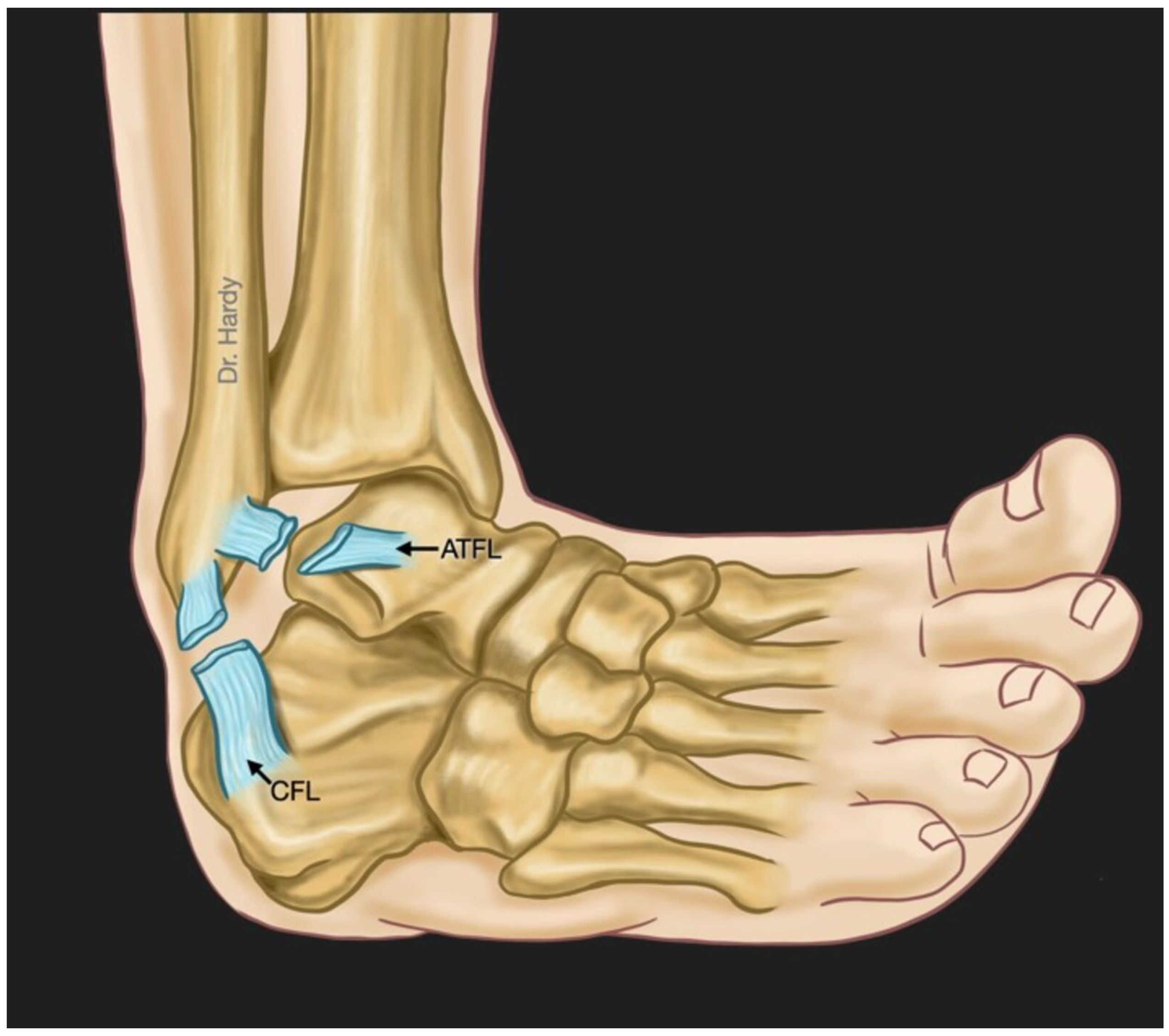
Figure 4.
This figure represents the anatomic surgical reconstruction of the lateral ankle ligaments using an autograft: the gracilis tendon harvested from the patient’s knee (This figure was created by the authors to be used in this paper).
Figure 4.
This figure represents the anatomic surgical reconstruction of the lateral ankle ligaments using an autograft: the gracilis tendon harvested from the patient’s knee (This figure was created by the authors to be used in this paper).
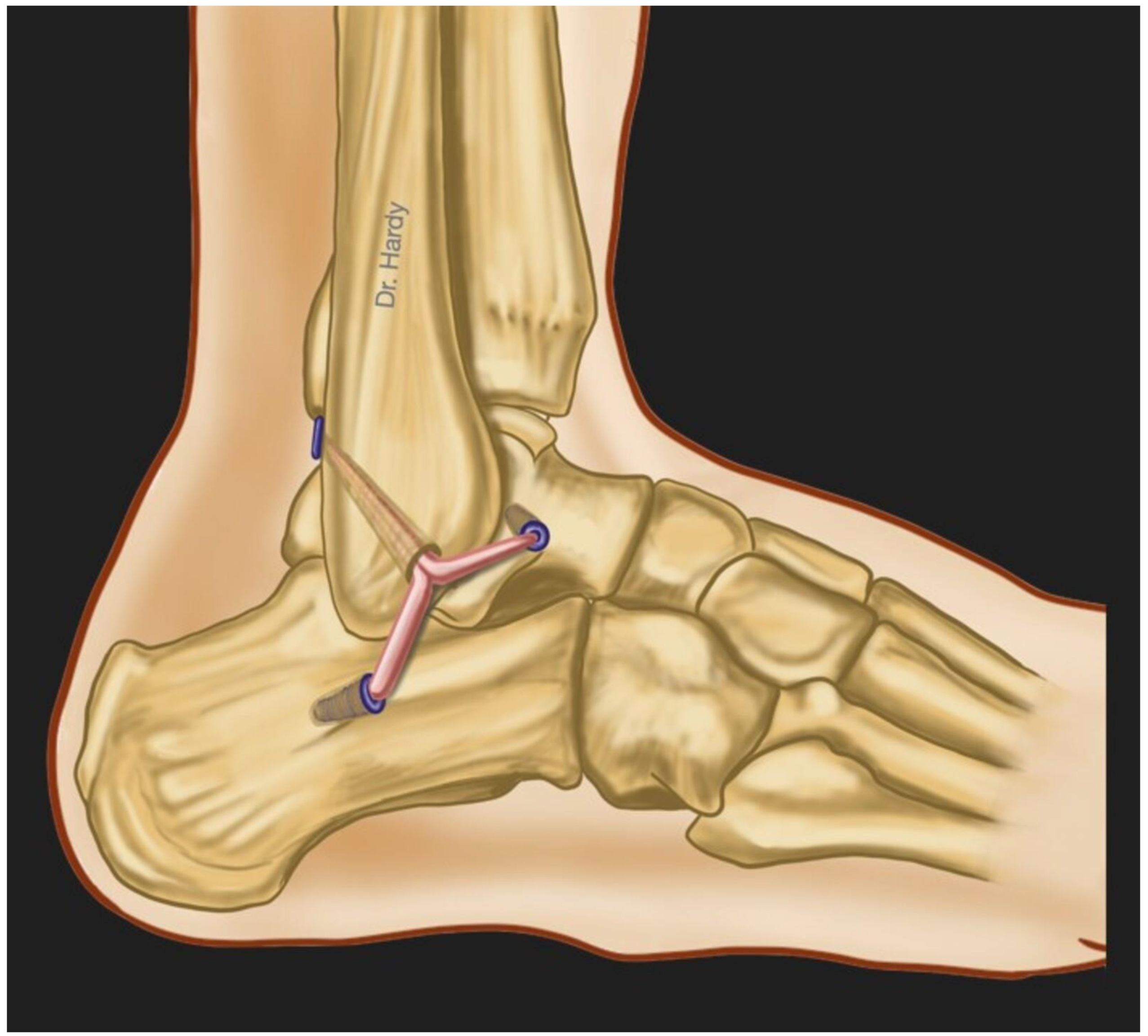
Figure 5.
Bioelectrical impedance of the ankle ligaments can be measured by injecting an electrical current using an injection electrode and detecting the resultant voltage decrease across the biological sample via another electrode. The two electrodes are placed on either side of the joint (This figure was created by the authors to be used in this paper).
Figure 5.
Bioelectrical impedance of the ankle ligaments can be measured by injecting an electrical current using an injection electrode and detecting the resultant voltage decrease across the biological sample via another electrode. The two electrodes are placed on either side of the joint (This figure was created by the authors to be used in this paper).
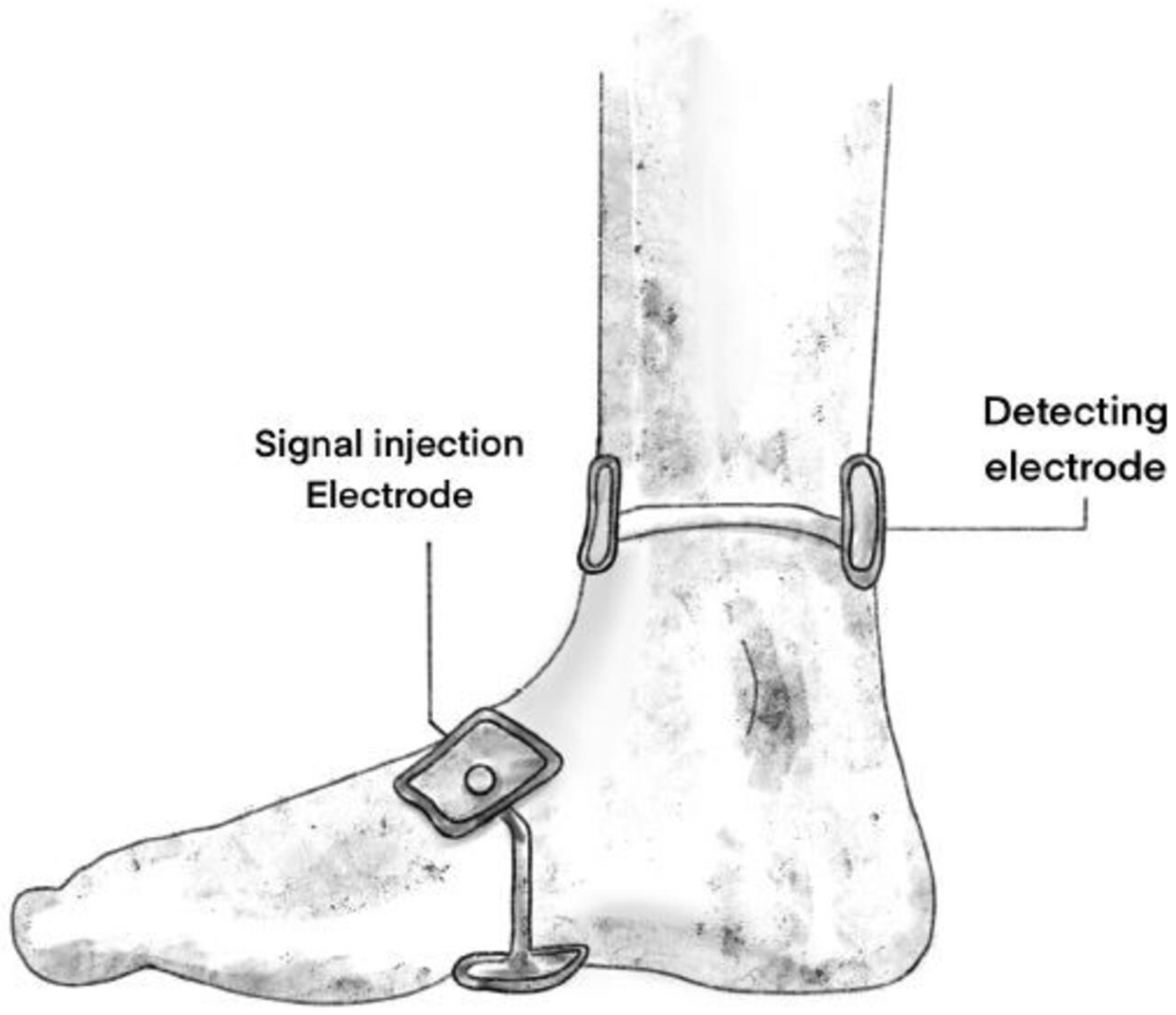
Figure 6.
Mechanical impedance represents the dynamic relationship between imposed deformations or motions (through the rotatory motor as shown in this figure) and the resulting torques determined by using a strain sensor (This figure was created by the authors to be used in this paper).
Figure 6.
Mechanical impedance represents the dynamic relationship between imposed deformations or motions (through the rotatory motor as shown in this figure) and the resulting torques determined by using a strain sensor (This figure was created by the authors to be used in this paper).
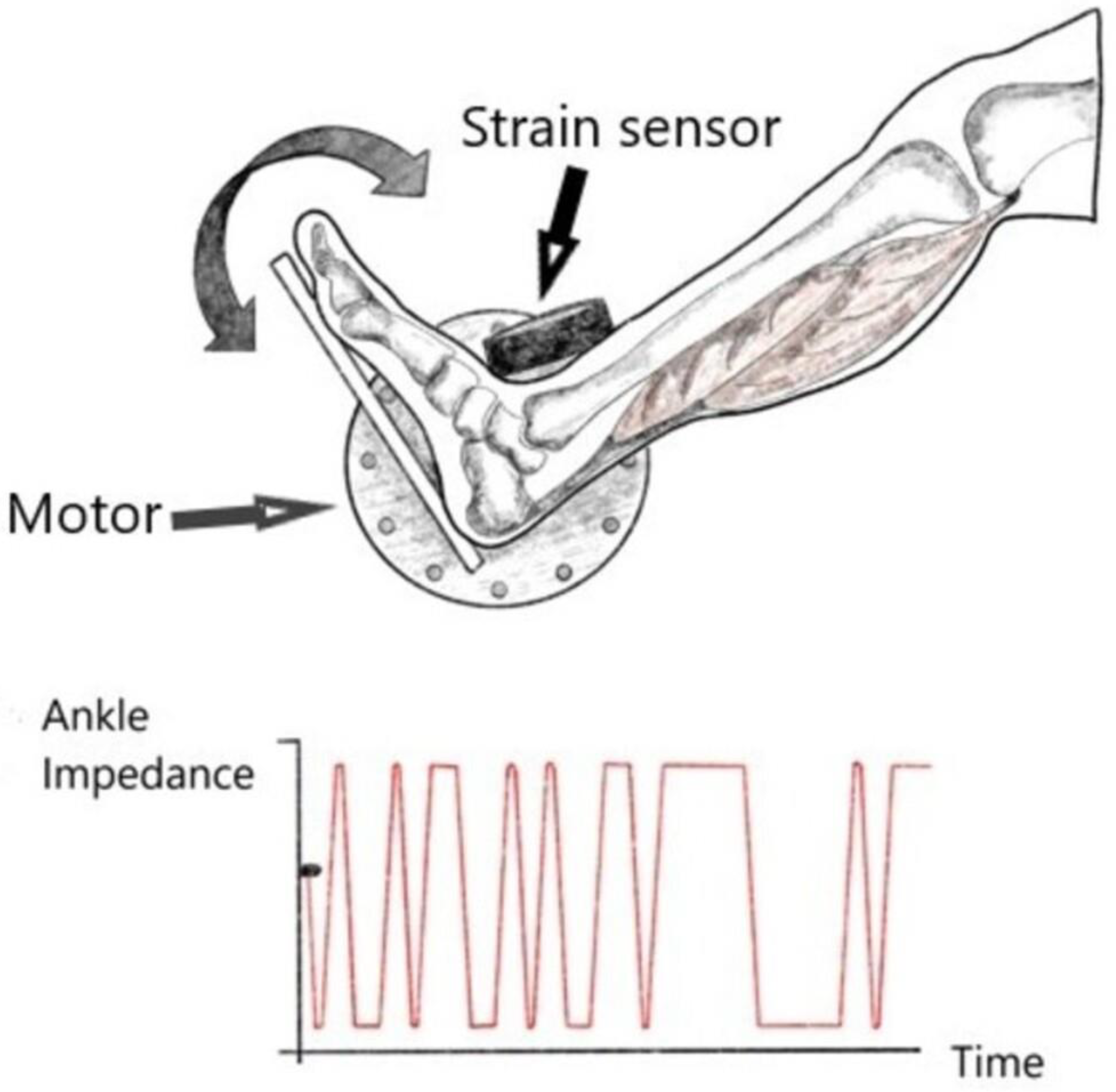
Figure 7.
A: Reflectance measurement of the Anterior Talo-Fibular Ligament (ATFL) of the ankle by using an optical fiber (Left). Inside this fiber, there are light transmitting and detecting fibers. The reflected light is converted into an electrical signal and visualized using a specific software (Right) (in this example, we used AvaSoft Version 8.14.0.0 to visualize the reflectance of ATFL with respect to wavelength). B: White reference is needed when converting hyperspectral data into reflectance.
Figure 7.
A: Reflectance measurement of the Anterior Talo-Fibular Ligament (ATFL) of the ankle by using an optical fiber (Left). Inside this fiber, there are light transmitting and detecting fibers. The reflected light is converted into an electrical signal and visualized using a specific software (Right) (in this example, we used AvaSoft Version 8.14.0.0 to visualize the reflectance of ATFL with respect to wavelength). B: White reference is needed when converting hyperspectral data into reflectance.
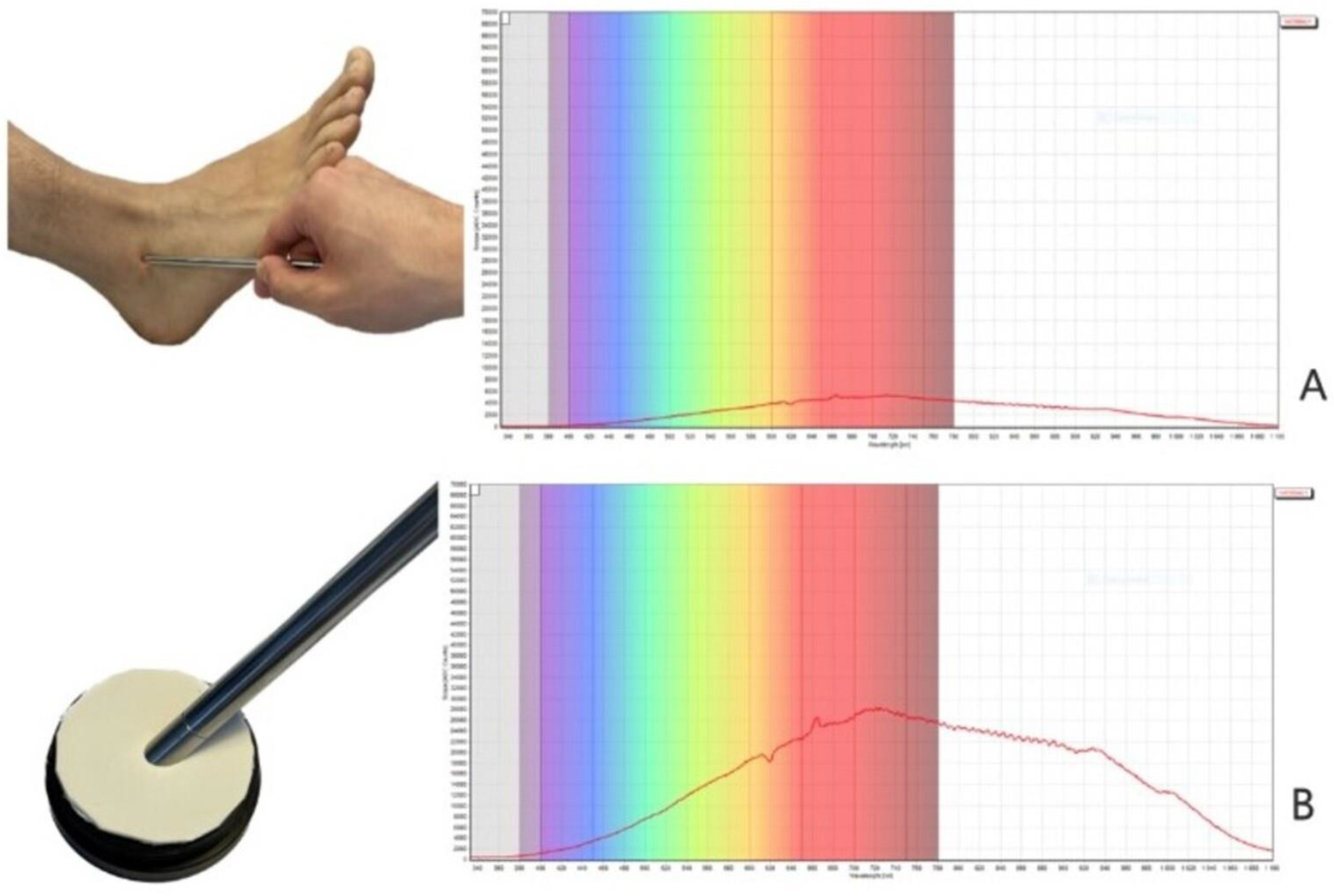
Figure 8.
This figure represents a simulation realized by the authors of this paper using MCML software. It shows the penetration depth (z) of the light through the different layers of the ankle before reaching the ligament. In this example, we chose the distance between the light emitting source (λ = 1300nm) and the photodetector to be 0.4 cm (the positions of E and PD correspond to r = 0.8cm and r = 1.2cm, respectively).
Figure 8.
This figure represents a simulation realized by the authors of this paper using MCML software. It shows the penetration depth (z) of the light through the different layers of the ankle before reaching the ligament. In this example, we chose the distance between the light emitting source (λ = 1300nm) and the photodetector to be 0.4 cm (the positions of E and PD correspond to r = 0.8cm and r = 1.2cm, respectively).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



